ANATOMY OF THORACOLUMBAR SPINE 12 thoracic vertebra Typical

ANATOMY OF THORACOLUMBAR SPINE

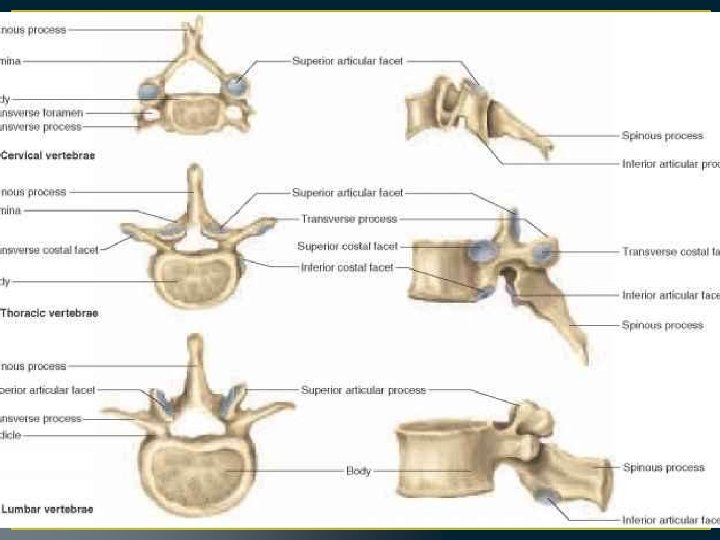
• 12 thoracic vertebra • Typical thoracic are 2 -9

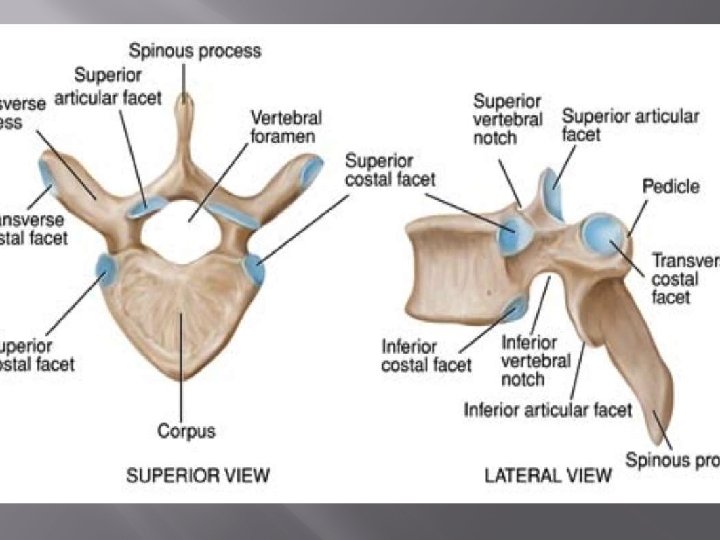
• Vertebral body is heart shaped. • Presence of demi-facets on the sides of each vertebral body – these articulate with the heads of the ribs.

• Presence of costal facets on the transverse processes – these articulate with the tubercles of the ribs. They are present on T 1 -T 10 only. • The spinous processes are long

The superior facet articulates with the head of the adjacent rib, and the inferior facet articulates with the head of the rib below

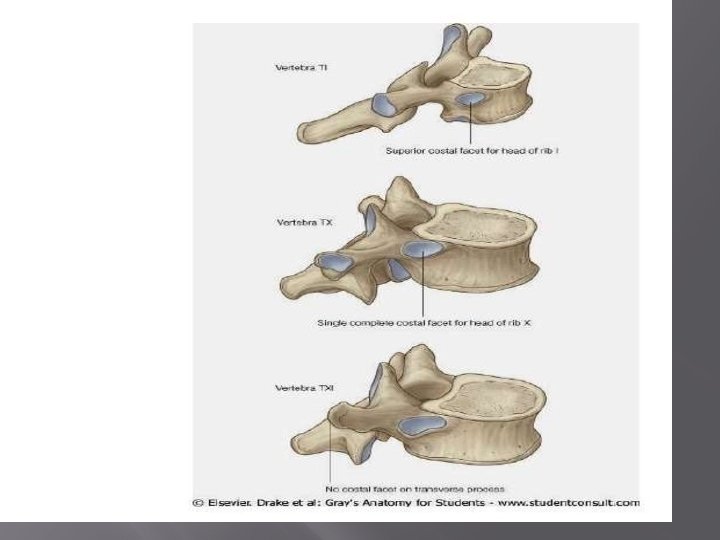
T 2 - T 9 is a typical vertebra, these facets are demi-facets.

• T 1 – Superior facet is not a demifacet, as this is the only vertebrae to articulate with the 1 st rib. • T 10 – A single pair of whole facets is present which articulate with the 10 th rib. These facets are located across both the vertebral body and the pedicle. • T 11 and T 12 – Each have a single pair of entire costal facets, which are located on the pedicles.
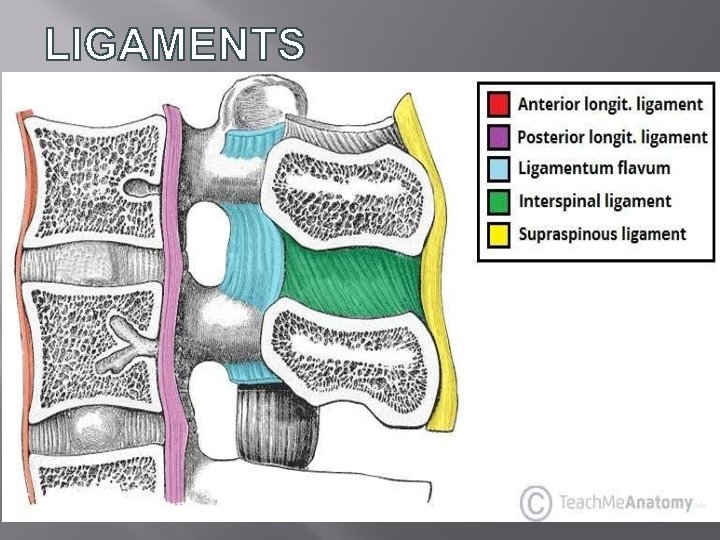

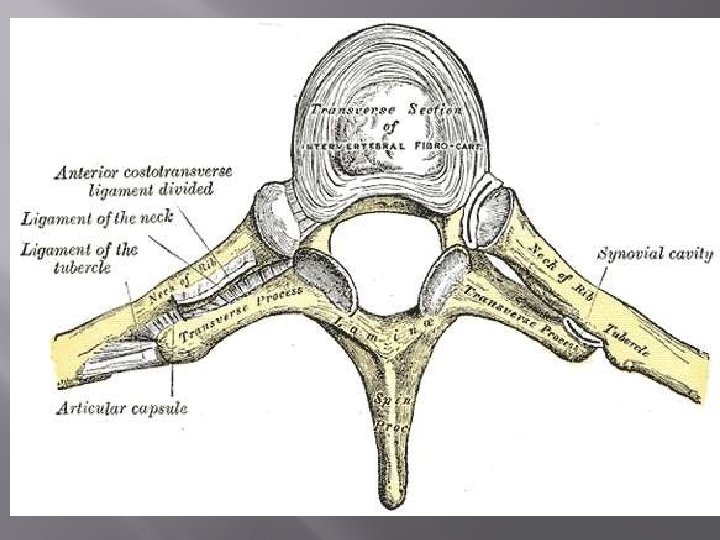
• Radiate ligament of head of rib – from the head of the rib to the bodies of the two vertebrae and intervertebral disc. • Costotransverse ligament – Connects the neck of the rib and the transverse process • Lateral costotransverse ligament – from the transverse process to the tubercle of the rib. • Superior costotransverse ligament – Passes from the upper border of the neck of the rib to the transverse process of the vertebra superior to it. •

• L 1 TO L 5 BODY SIZE INCREASE • the L 5 vertebra has the heaviest body, smallest spinous process, and thickest transverse process.
 APPROACH TO THE THORACIC SPINE • Posterolateral (Costotransversectomy) Approach to")
• ANTERIOR (TRANSTHORACIC) APPROACH TO THE THORACIC SPINE • Posterolateral (Costotransversectomy) Approach to the Thoracic Spine • Posterior Approach to the Thoracic and Lumbar Spines

• Effective in • Treatment of infections, such as tuberculosis of the thoracic vertebral bodies 20 • Fusion of the vertebral bodies • Resection of the vertebral bodies for tumor and reconstruction with bone grafting • Correction of scoliosis (Dwyer instrumentation technique and rods) • Correction of kyphosis • Anterior spinal cord decompression • Biopsy

• On the side • Move arm above his head • Approach from right side

• Inferior angle of the scapula • Spinous process • Inframammary crease • Incision

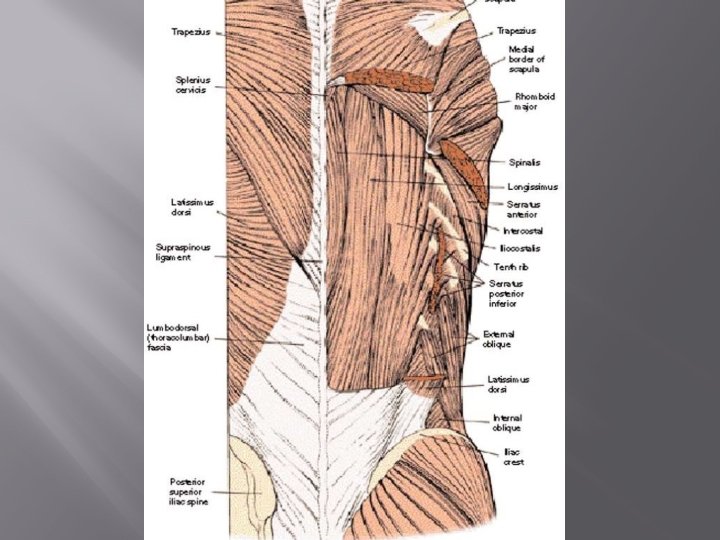
• Latismus Dorsi division • Serratus anteriorelevate scapula • Rhomboids? • Bleeding • Resect ribs

• Cut the periosteum on the upper border of the rib.

• • Deflate lungs Retract anteriorly Identify oesophagus Incise pleura

• Retract the oesophagus • IC vessels that cross the field need to be ligated • Cord ishemia

• Indication • Abscess drainage • Vertebral body biopsy • Partial verterbral body resection • Limited anterior spinal fusion • Ant. Lateral decompression of the spinal cord

• Prone • Bolsters • Drape widely

• Curvilinear lateral to spinous process • Center over th. Incisione involved rib

• No true internervous plane • Trapezius is cut

• Cut onto the posterior aspect of the rib to be resected • Incise the periosteum over the rib

• Separate muscles from the rib using subperiosteal resection

• Divide rib 8 cm from the midline • Cut muscle attachment and costotransverse ligaments

• Enter the retropleural space by blunt dissection and digital palpation • Safe in disease only

• Nerves- Dura • intercostal vessels • Lungs- pneumo thorax

• Indications • Scoliosis • Posterior spine fusion • Removal of tumour of the posterior aspect of the vertebra • Open biopsy • Stabilization of fractures vertebrae

• Prone • Bolsters • Landmarks – gluteal cleft, C 7 T 1

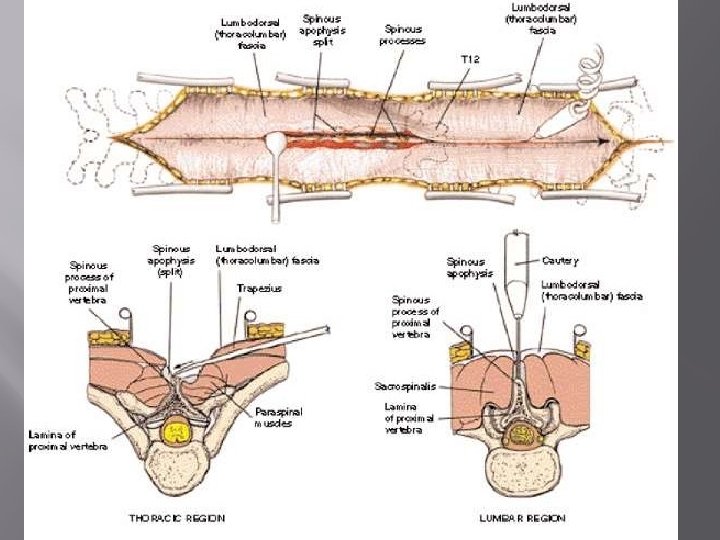
• Midline straight • Internervous planemidline paraspinal muscles • it is truly internervous; the nerves do not cross the midline

• The paraspinal muscles are innervated segmentally by the posterior primary rami of the individual nerve roots in the thoracic and lumbar spines.

• Palpate the individual spinous processes • dissect down to the middle of the spinous processes and move the muscle origins to either side of the surface

• Remove the paraspinal • remove the short rotators from the base of the spinous processes to the leading edges of the laminae

• The posterior primary rami emerge posteriorly from between the transverse processes, close to the facet joints. Because of the significant overlap of innervation in the paraspinal muscles • Segmental vessels
- Slides: 44