RICKETS OSTEOMALACIA Def reduction in bone mineralization OSTEOMALACIA

RICKETS & OSTEOMALACIA Def. : reduction in bone mineralization !

OSTEOMALACIA and RICKETS Clinical syndromes that result from inadequate bone mineralization

Vitamin D Deficiency Osteomalacia & Rickets Osteomalacia occurs in adults n Rickets occurs in children n Defective mineralization of the skeleton n

VITAMIN D DEFICIENCY n Vitamin D deficiency leads to decreased absorption of calcium by the GI tract. n As serum calcium starts to fall, secondary hyperparathyroidism occurs.

VITAMIN D DEFICIENCY n Elevated Pth levels may maintain serum calcium in the normal range, but at the cost of phosphaturia, hypophosphatemia and increased bone reabsorption n Low serum phosphate results in inadequate bone mineralization and osteopenia.

VITAMIN D DEFICIENCY n In severe cases, secondary hyperparathyroidism is not adequate to maintain serum calcium levels, and hypocalcemia occurs.

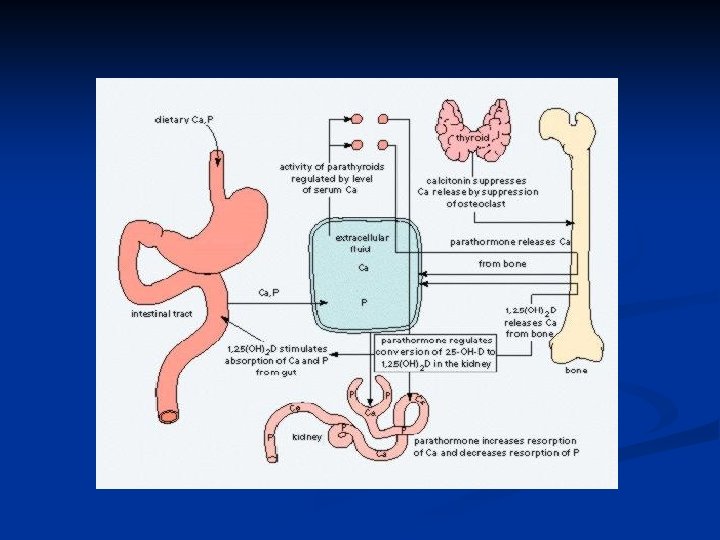
OSTEOMALACIA, RICKETS Normal bone metabolism n CALCIUM 99% in bone. Main functions- muscle /nerve function, clotting. Plasma calcium- 50% free, 50% bound to albumin. n Dietary needs- Kids- 600 mg/day, Adolesc. -1300 mg/day, Adult-750 mg/day, Pregnancy-1500 mg/day, Breastfeeding-2 g/day, Fractures - 1500 mg/day n Absorbed in duodenum (active transport) and jejunum (diffusion), 98% reabsorbed in kidney prox. tubule, may be excreted in stool.

OSTEOMALACIA, RICKETS Normal bone metabolism n n PHOSPHATE 85% in bone. Functions-metabolite and buffer in enzyme systems. Plasma phosphate mainly unbound. Daily requ. 1 -1. 5 g/day

OSTEOMALACIA, RICKETS Regulation of Calcium & Phosphate Metabolism: Peak bone mass at 16 -25 years. Bone loss 0. 3 - 0. 5% per year (2 -3% per year after 6 th decade). 1. Parathyroid Hormone (PTH) 2. Vitamin D 3 3. Calcitonin 4. Other Hormones: Estrogen: Prevents bone loss Corticosteroids: Increases bone loss Thyroid hormones: Leads to osteoporosis Growth hormones: Cause positive calcium balance Growth factors

Vitamin D n RDA Range Adult males: 5 – 10 mg/day n Adult females: 5 – 10 mg/day n n Primary source of Vitamin D n n Sunlight Dietary source of Vitamin D n Fortified milk

Sources of Vitamin D Cod liver oil n Egg yolk n
 is synthesized")
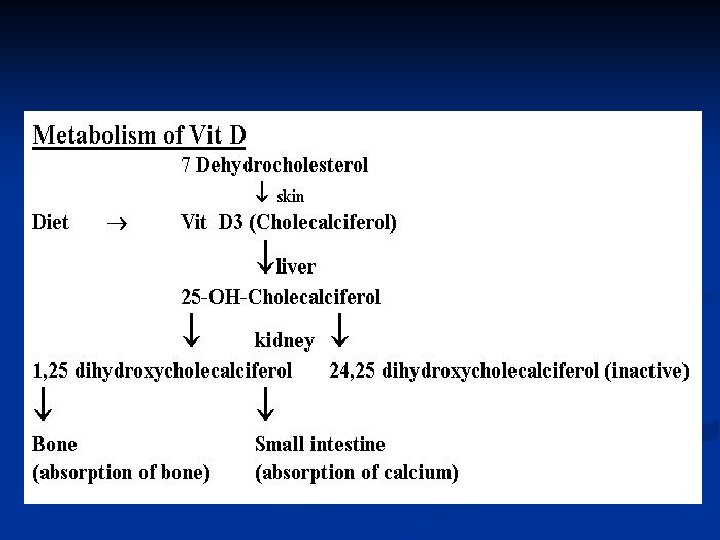
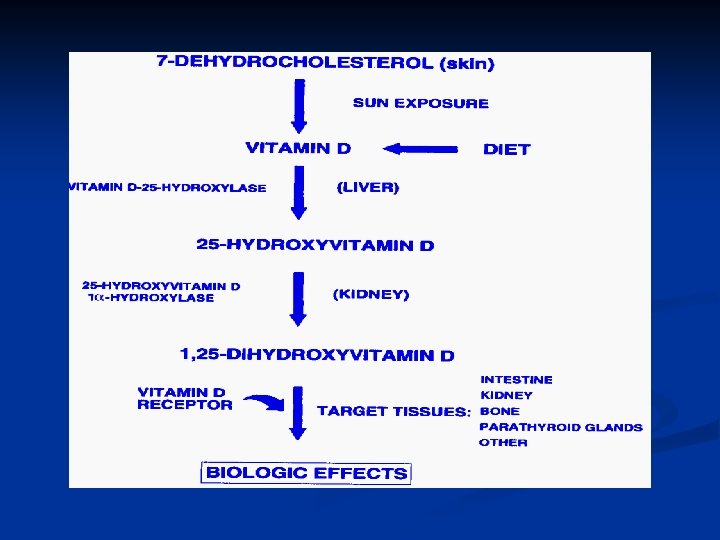
Biochemistry of Vitamin D 3 – Brief Review Vitamin D 3 (cholecalciferol) is synthesized in the skin, with UV light, from 7 -dehydrocholesterol n Vitamin D 3 is hydroxylated twice – first in the liver, to 25 hydroxycholecalciferol, then in the kidney, to 1, 25 dihydroxycholecalciferol, the most potent form of Vitamin D n

Vitamin D metabolism

Vitamin D Metabolism
 n Primary role of Vitamin D n n Increase calcium and")
Vitamin D (cont’) n Primary role of Vitamin D n n Increase calcium and phosphate absorption from the intestines Other tissues that Vitamin D acts on Parathyroid glands n Bone, Kidneys n Skin, Brain, Pituitary n Lymphocytes, Tumors n

Vitamin D Deficiency n Secondary to Insufficient sun exposure n Malabsorption, Malnutrition n Liver disease n Renal disease, nephrotic syndrome n Anticonvulsants (generics Phenytoin, Carbamazepine, Valproate, Phenobarbital) can inhibit hepatic hydroxylation of Vitamin D n

Other conditions that can cause Osteomalacia Hereditary or acquired disorders of vitamin D metabolism Kidney failure and acidosis Phosphate depletion associated with not enough phosphates in the diet Cancer Side effects of medications used to treat seizures (Dilantin) Liver disease

RICKETS, OSTEOMALACIA PATHOLOGY: Sufficient osteoid, poor mineralization (Rickets is found only in children prior to the closure of the growth plates, while OSTEOMALACIA occurs in persons of any age. Any child with rickets also has osteomalacia, while the reverse is not necessarily true).

RICKETS, OSTEOMALACIA CAUSES: 1. 2. 3. 4. 5. Nutritional deficiency 1. Vit D 2. chelators of calcium- phytates, oxalates, phosphorous 3. Antacid abuse, causing reduced dietary phosphate binding GI Absorption defects 1. Post gastrectomy 2. Biliary disease (reduced absorption of Vitamins ) 3. Small bowel disease 4. liver disease Renal tubular defects Renal osteodystrophy Miscellaneous causes
 n Secondary to many things, including Vitamin")
Vitamin D Deficiency Osteomalacia & Rickets (cont’) n Secondary to many things, including Vitamin D deficiency as discussed above n Dietary calcium deficiency n Phosphorus deficiency n Aluminum toxicity n Hypophosphatasia n Fibrogenesis imperfecta ossium n

Clinical features n n n Osteomalacia in adults starts insidiously as aches and pains in the lumbar (lower back) region and thighs, spreading later to the arms and ribs. Pain is non-radiating, symmetrical, and accompanied by tenderness in the involved bones. Proximal muscles are weak, and there is difficulty in climbing up stairs and getting up from a squatting position. Physical signs include deformities like and lordosis. Pathologic fractures due to weight bearing may develop. Most of the time, the only alleged symptom is chronic and bone aches are not spontaneous but only revealed by pressure or shocks.

RICKETS, OSTEOMALACIA CLINICAL FEATURES: n Rickets - Tetany , convulsions, failure to thrive, restlessness, muscular flaccidity. Flattening of skull (craniotabes), Thickening of wrists from epiphyseal overgrowth, Stunted growth, Rickety rosary, spinal curvature, Coxa vara, bowing, # of long bones n Osteomalacia, - Aches and pains, muscle weakness loss of height, stress #s.

Manifestations of Osteomalacia Localized bone pain Difficulty walking Low back pain Fractures are common, and delayed healing occurs Muscular weakness Weight loss Progressive deformities of the spine (kyphosis)

Kyphosis

RICKETS, OSTEOMALACIA XRAY FINDINGS: RICKETS Thickening and widening of physes, Cupping of metaphysis, Wide metaphysis, Bowing of diaphysis, Blurred trabeculae.

RICKETS, OSTEOMALACIA XRAY FINDINGS: OSTEOMALACIA Loosers zones - incomplete stress # with healing lacking calcium, on compression side of long bones. Codfish vertebrae due to pressure of discs Trefoil pelvis, due to indentation of acetabulae stress #s

Source Undetermined

Source Undetermined



Osteomalacia & Rickets – Clinical Manifestations Asymptomatic at onset n Muscle weakness, especially of pelvic girdle n Bone pain n Atraumatic fractures n X-rays assist in diagnosis n
 n Vitamin D deficiency can cause Osteoporosis n Osteomalacia and")
Vitamin D Deficiency (cont’) n Vitamin D deficiency can cause Osteoporosis n Osteomalacia and Rickets n

Source Undetermined

Extra skeletal findings in Rickets n Extraskeletal manifestation of rickets vary depending upon the 1 ry mineral deficiency. n Hypoplasia of the dental enamel is typical for hypocalcemic rickets, whereas abscesses of the teeth occur more often in phosphopenic rickets. n Hypocalcemic seizures, decreased muscle tone leading to delayed motor milestones, recurrent infections, increased sweating.



RICKETS, OSTEOMALACIA INVESTIGATIONS: BLOOD TESTS Calcium Reduced, Phosphate reduced Alkalline Phosphatase increased Urinary excretion of calcium diminished Calcium phosphate products (= serum [Ca] x serum [PO 4]) normally 30. In rickets and osteomalacia is less than 24

Osteomalacia & Rickets Diagnosis n Other laboratory abnormalities may include Hypocalcemia n Hypophosphatemia n Elevated serum alkaline phosphatase n

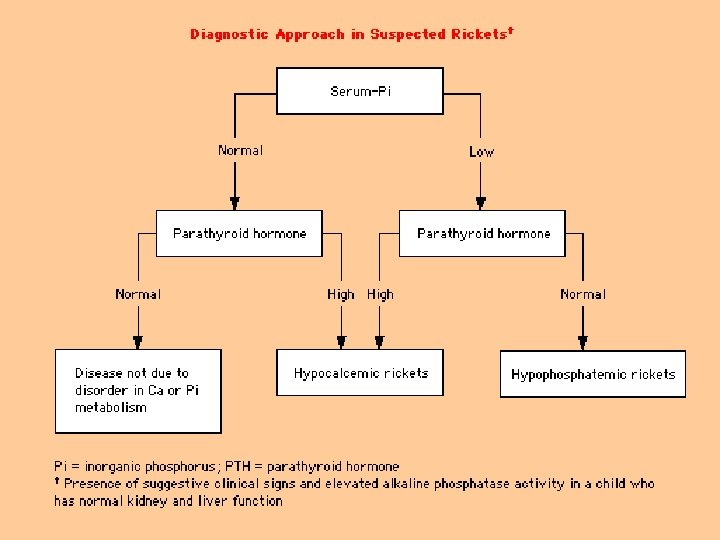
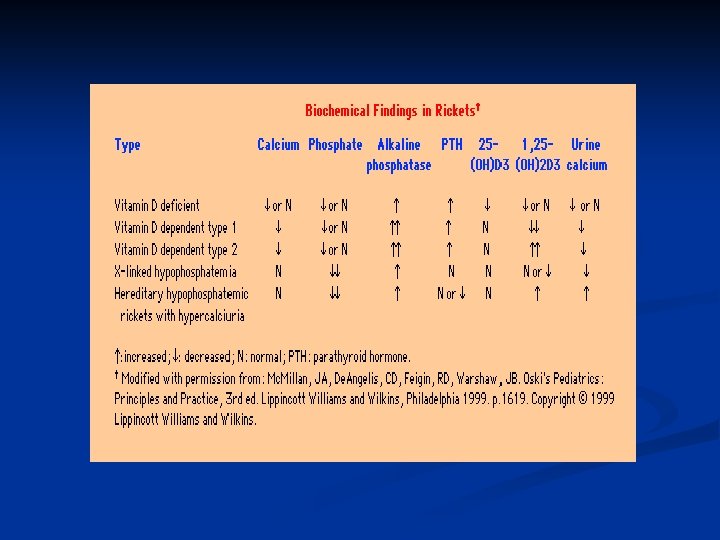
Biochemical findings in rickets n Alkaline phosphatase usually is ↑in all forms of rickets. n Serum phosphorus concentrations usually are↓ in both hypocalcemic and hypophosphatemic rickets. n Serum Ca is ↓only in hypocalcemic rickets. n Serum parathyroid hormone typically is ↑in hypocalcemic rickets, in contrast it is N in hypophosphatemic rickets. n 25 -OH vitamin D reflect the amount of vitamin D stored in the body, and is ↓in vit D deficiency. n 1, 25 -OH 2 vitamin D can be↓, N or ↑in hypocalcemic rickets and usually is N or slightly ↑in hypophosphatemic rickets.

Osteomalacia & Rickets Diagnosis Bone biopsy is diagnostic n Serum 25 -hydroxycholecalciferol <50 nmol/L indicates Vitamin D deficiency n

OSTEOMALACIA: EVALUATION n Careful diet and sunlight history n Renal function n Fecal fat determination n Anti Ig. A tissue transglutaminase antibodies. Small bowel biopsy

RICKETS, OSTEOMALACIA MANAGEMENT: Depends on the cause Nutritional Vitamin D deficiency Dietary chelators of calcium Phytates Oxalates Phosphorus deficiency (unusual) Antacid abuse Treatment- vitamin D (50000 u/w`/up to 3 -12 w) and Calcium (1. 5 -2 g/day)

RICKETS, OSTEOMALACIA MANAGEMENT: Depends on the cause Gastro-intestinal absorption defects Post-gastrectomy Biliary disease Enteric absorption defects Short bowel syndrome Rapid onset (gluten-sensitive enteropathy) Inflammatory bowel disease Crohns Celiac

RICKETS, OSTEOMALACIA MANAGEMENT: Depends on the cause Renal tubular defects Vitamin D dependant type I type II Treatment; High levels of vit D Vitam in D resistant (familial hypophosphatemic rickets) Treatment; Phosphate 1 -3 gm daily, Vit D 3 high dose Fanconi syndrome I, III Renal tubular acidosis

Collaborative Care of Osteomalacia n Correction of the vitamin D deficiency Vitamin D 3 and vitamin D 2 can be supplemented (patient shows dramatic response) n Calcium salts or phosphorus supplements may also be prescribed n Encourage dietary ingestion of eggs, low-fat milk, fish and vegetables n Exposure to sunlight is valuable n Encourage weight bearing exercises n

RICKETS, OSTEOMALACIA MANAGEMENT: Depends on the cause Renal Osteodystrophy – in chronic renal failure Miscellaneous Hypophosphatasia Anticonvulsant therapy SURGERY For deformities

Vitamin D Deficiency Treatment 50, 000 IU of oral Vitamin D 2, once or twice weekly for 6 – 12 w, followed by 1000 IU/day n Appropriate exposure to sunlight n Phosphate and Calcium replacement, if needed n


OSTEOMALACIA: ETIOLOGY n Vitamin D deficiency or resistance n Inadequate intake and sunlight n Malabsorption n Severe liver disease n Renal failure n Hereditary syndromes

OSTEOMALACIA: ETIOLOGY n Phosphate deficiency n Renal tubular disorders n Tumor associated osteomalacia n X-linked hypophosphatemia n Phosphate binders

OSTEOMALACIA: ETIOLOGY n Inhibitors of mineralization n Aluminum n Fluoride

OSTEOMALACIA: CLINICAL MANIFESTATIONS n Bone pain and pathologic fractures n Decreased bone density n Hypophosphatemia, increased alkaline phosphatase, and increased PTH

OSTEOMALACIA: CLINICAL MANIFESTATIONS n Late hypocalcemia n Pseudofractures n In children, bowing of the legs and rachitic rosary, short stature

OSTEOMALACIA: DIAGNOSIS n Low levels of 25 -hydroxyvitamin D n Elevated parathyroid hormone and alkaline phosphatase n Bone biopsy
 Vitamin D deficiency resulting in decalcification and softening of the")
Osteomalacia (adult bone disease) Vitamin D deficiency resulting in decalcification and softening of the bone n Same as Ricketts in children n
 Not enough vitamin D in the diet n Not enough exposure to")
Etiology (osteomalacia) Not enough vitamin D in the diet n Not enough exposure to sunlight, which produces vitamin D in the body n Malabsorption of vitamin D by the intestines n

Osteomalacia n Clinical features? n In child In adult n Investign n Ca/PO 4 decr, alk ph incr, Ca excr decr n Ca x PO 4 <2. 4 n Bone biopsy n

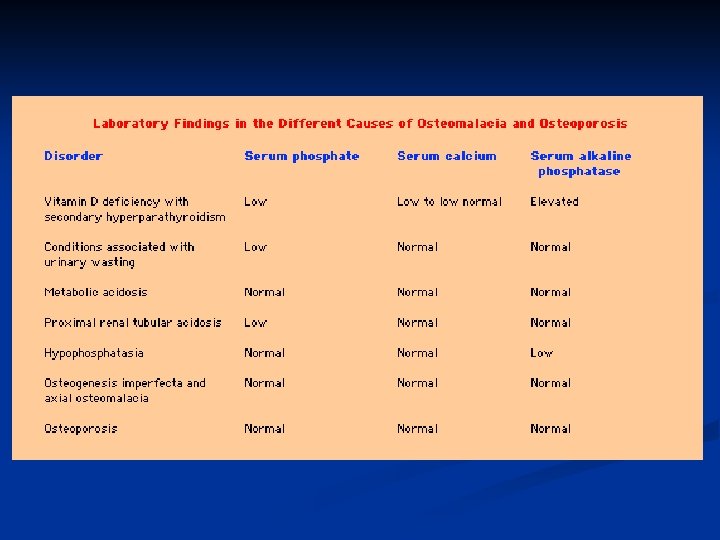
Laboratory findings in Osteomalacia Decreased serum calcium levels n Decreased serum phosphorus levels n Elevated serum alkaline phosphatase n Xrays show bone demineralization n

Laboratory findings in Osteomalacia Decreased serum calcium levels n Decreased serum phosphorus levels n Elevated serum alkaline phosphatase n Xrays show bone demineralization n

Introduction n Normal bone growth & mineralization require adequate availability of calcium & phosphate. n Deficient mineralization can result in rickets and/or osteomalacia. n Rickets refers to the changes caused by deficient mineralization at the growth plate. n Osteomalacia refers to impaired mineralization of the bone matrix. n Rickets & osteomalacia usually occur together as long as the growth plates are open; only osteomalacia occurs after the growth plates have fused.

Causes of Rickets n VITAMIN D DISORDERS Nutritional vitamin D deficiency; Congenital vitamin D deficiency; Secondary vitamin D deficiency; Malabsorption ; Increased degradation; Decreased liver 25 hydroxylase; Vitamin D-dependent rickets type 1; Vitamin D-dependent rickets type 2 ; Chronic renal failure. n CALCIUM DEFICIENCY Low intake Diet Premature infants (rickets of prematurity) Malabsorption Primary disease Dietary inhibitors of calcium absorption n PHOSPHORUS DEFICIENCY Inadequate intake Premature infants (rickets of prematurity) Aluminum-containing antacids n RENAL LOSSES X-linked hypophosphatemic rickets; Autosomal dominant hypophosphatemic rickets; Hereditary hypophosphatemic rickets with hypercalciuria; Overproduction of phosphatonin ( Tumor-induced rickets, Mc. Cune-Albright syndrome’ Epidermal nevus syndrome, Neurofibromatosis) , Fanconi syndrome, Dent disease n DISTAL RENAL TUBULAR ACIDOSIS

Treatment of Rickets n Vitamin D. stoss therapy: 300, 000 -600, 000 iu orally or IM in 2 -4 divided doses over one day. n High dose vit D 2000 -5000 iu orally for 4 -6 wks followed by 400 iu daily orally as maintenance. n Adequate dietary Calcium & phosphorus provided by milk, formula & other dairy products. n Symptomatic hypocalcaemia need IV cacl as 20 mg/kg or ca gluconate as 100 mg/kg as a bolus, followed by oral calcium tapered over 2 -6 weeks.

Osteomalacia Disorder of mineralisation of newly formed bone matrix n Vitamin D deficiency n Hypophosphatemia (Fanconi syndrome, X-linked hypophosphatemic rickets) n Bone matrix disorders (Fibrogenesis imperfecta, Hypophosphatasia) n Aluminium n

Osteomalacia Skeletal pain, proximal muscle weakness n X-ray – Looser’s zones n Laboratory – low PO 4 -, (vitamin D deficiency: low Ca 2+, increased alkaline phosphatase) n n Treat underlying deficiency

Osteomalacia Skeletal pain, proximal muscle weakness n X-ray – Looser’s zones n Laboratory – low PO 4 -, (vitamin D deficiency: low Ca 2+, increased alkaline phosphatase) n n Treat underlying deficiency

Osteomalacia n Definition? n n Rickets - growth plates affected, children Osteomalacia - incomplete mineralisation of osteoid, adults Types - vit D def, vit-D resist (fam hypophos) n Aetiology? n Decr intake/production(sun/diet/malabs) Decreased processing (liver/kidney) Increased excretion (kidney) n n n

Osteomalacia Types n Vitamin D deficient n Hypophosphataemic n growth decr +++ and severe deformity with wide epiphyses n x-linked dominant n decreased tubular reabs of PO 4 n Ca normal but low PO 4 n Rx PO 4 and vit D n

Osteomalacia vs osteoporosis Osteomal Osteopor Ageing fem, #, decreased bone dens Ill Not ill General ache Asympt till # Weak muscles normal Loosers nil Alk ph incr normal PO 4 decr normal Ca x PO 4 <2. 4 Ca x PO 4 >2. 4

What are osteomalacia / Rickets Osteomalacia n Disorder of mature bone in which mineralisation of new osteoid bone is inadequate or delayed Rickets n Disease of growing bones in which defective mineralisation occurs in both bone and cartilage of epiphyseal growth plate, associated with: n n Growth retardation Skeletal deformities

Rickets The primary pathology is defective mineralisation of bone matrix n The primary bone matrix mineral = hydroxyapatite = Ca 10(Po 4)6(OH)2 n Any disease that limit the availability of calcium or phosphate will lead to rickets n 2 main categories n n Hypocalcaemia rickets n Disorders of vitamin D metabolism or action n Hypophosphatemic rickets n Disorders of phosphate metabolism

Causes n Nutritional: commonest cause in the developing countries n Malabsorption n Drugs that increases metabolism of vitamin D in the liver n Chronic liver disease n Renal rickets n n n Chronic renal failure RTA Hereditary rickets n n Vitamin D dependent rickets ( Type 1& 2) Vitamin D resistant rickets

Celiac disease n Pancreatic insufficiency n n n Cystic fibrosis Hepato-biliary disease Biliary Artesia n Cirrhosis n neonatal hepatitis n n Drugs n Anti-convulsants n Phenobartbitone n Phenytoin n Diet n Excess of phytate in diet with impaired

Chronic liver disease Cirrhosis reduces 25 -hydroxylation of vitamin D n Biliary obstruction: n prevents absorption of fat soluble vit D n Interrupts its enterohepatic circulation n

Chronic renal failure n n n Reduces 1 hydroxylation of 25 hydroxy vitamin D leads to low concentration of 1, 25 -di hydroxy vitamin D Consequently impair calcium absorption from the gut Renal osteodystrophy n n Osteitis fibrosa cystica due to long standing secondary hyperparathyroidism When GFR falls below 30 ml/min/1. 73 m 2 n n Impaired growth Osteitis fibrosa results n n n Sub-periosteal resorption at middle and distal phalanges Bone pain Muscle weakness
 n Vitamin D dependent rickets")
Hereditary Rickets n Hypophosphatemic rickets (Vit D resistant) n Vitamin D dependent rickets

Vitamin D dependent rickets Type 1 n Rare, autosomal recessive n Lack of 1 hydroxylase enzyme n Clinically and Biochemically similar to nutritional rickets except it appears early at 3 -4 months Type 2 n Rare autosomal recessive disorder n 1 hydroxylase enzyme is present n Lack of Calcitriol receptors n Common in Arabs n Baldness n Severely affected individuals n Unresponsive to treatment

Hypophosphatemic rickets Nutritional phosphate deficiency n Prematurity n Decreased intestinal absorption of phosphate n n n Ingestion of phosphate binders (aluminum hydroxide) Renal phosphate wasting RTA n Vitamin D resistant rickets n n Tumor induced osteomalacia (oncogenic osteomalacia)

Hypophosphatemic Rickets X-linked dominant / Autosomal dominant n Males affected more than females n Commonest inherited form of rickets n Prevalence 1: 25000 n Phosphate wasting by renal tubules leads to: n Low serum phosphate n Normal calcium n n In-appropriate low or normal 1, 25 -di hydroxy vitamin D n phosphate is the major stimulus for 1 hydroxylase

Clinical features n n The earliest sign of rickets in infant is craniotabes (abnormal softness of skull) Delayed closure of anterior fontanel Widening of the forearm at the wrist (widened metaphysis= area between epiphysis and diaphysis) Rachitic rosary n n Harrison’s groove n n Swelling of the costo-chondral junction Lateral indentation of the chest wall at the site of attachment of diaphragm Bowing of tibia and fibula may be observed at any age Growth retardation due to impaired calcification of bone epiphysis (epiphysis= area of growth plates) Hypocalcaemic manifestations n n hypotonia Seizure, tetany, muscle weakness, paraesthesia, numbness

Biochemical findings of rickets n Vitamin D deficiency rickets Low- normal serum calcium level n Increased secretion of PTH (secondary hyperparathyroidism) to compensate for low calcium n Hyperparathyroidism will increase renal excretion of phosphate, leads to low serum phosphate level n Elevated alkaline phosphatase enzyme n Reduced urinary calcium level n Low level of both 25 and 1, 25 - di hydroxy n

Biochemical findings of rickets Hypophosphatemic rickets n Low serum phosphate level n Normal calcium level n Normal parathyroid hormone level n High alkaline phosphatase level n In-appropriate low or normal 1, 25 -di hydroxy vitamin D n phosphate is the major stimulus for 1 hydroxylase

Radiological findings of rickets n n n Generalized osteopenia Widening of the unmineralised epiphyseal growth plates Fraying of metaphysis of long bones Bowing of legs Pseudo-fractures (also called loozer zone) n n n Transverse radio lucent band, usually perpendicular to bone surface Complete fractures Features of long standing secondary hyperparathyroidism (Osteitis fibrosa cystica) n n Sub-periosteal resorption of phalanges Presence of bony cyst (brown Tumor)

Therapy n Administration of vitamin D preparation Vit D 2 = ergocalciferol n 25 -hydroxy vitamin D = calcifedol n 1 hydroxy vitamin D = one alpha n 1, 25 Di hydroxy Vitamin D = Calcitriol n n Calcium supplement initially in severe disease n n To avoid hungry bone hypocalcaemia Phosphate supplements in Hypophosphatemic rickets

Osteomalacia is the general term for the softening of the bones due to defective bone mineralization. n Osteomalacia in children is known as rickets, and because of this, osteomalacia is often restricted to the milder, adult form of the disease. n It may show signs as diffuse body pains, muscle weakness, and fragility of the bones. n

General characteristics n n Osteomalacia is derived from Greek: osteo refers to bone, and malacia means softness. Osteomalacia in the adult is most commonly found in confined, dark-skinned, or diet-disbalanced subjects. Many of the effects of the disease overlap with the more common osteoporosis, but the two diseases are significantly different. Osteomalacia is specifically a defect in mineralization of the protein framework known as osteoid. This defective mineralization is mainly caused by lack in vitamin D.

Physiology Serum Ca & Phosphate in equilibrium with Ca , Phosphate in bone. n There is relation: . ( Ca X Phosphate) =constant product. n Important of this relation to keeping Ca , Phosphate cross product constant. n So, more ppt. in vascular system or soft tissue, there is no metastasis calcification. n

PATHO PHYSIOLOGY Kidney disease Defect in phosphate execration § No hydroxylation of Vit. D 3 § §

PATHO PHYSIOLOGY Hypocalcaemia So, Stimulation of PTH Bone. . § Relase of Ca. § § Kidney § Ca absorption §

Treatment Nutritional osteomalacia responds well to administration of 200, 000 IU weekly of vitamin D for 4 to 6 weeks, followed by a maintenance dose of 1600 IU daily or 200, 000 IU every 4 to 6 months. n Natural sources cheese, sardines, salmon, dark leafy vegetables & sesame seeds. n
- Slides: 97