Health Care Reform Universal Health Care The Only























")
")















 Past Chairman, Health & Retirement")



")
- Slides: 53
Health Care Reform Universal Health Care: The Only Solution Diljeet K. Singh, MD, Dr. PH Physicians for a National Health Program 29 E Madison Suite 602, Chicago, IL 60602 Phone (312) 782 -6006 | Fax: (312) 782 -6007 email: info@pnhp. org www. pnhp. org
PERSPECTIVE - Philosophical Health care is… • A Human Right • A social service distributed according to need • Not a commodity distributed according to ability to pay • Not a business whose “beneficiaries” are company executives and investors not patients • Most Americans believe everyone should have access to good care without financial hardship
PERSPECTIVE - Philosophical • We are the only developed nation that does not provide comprehensive health care to all its citizens • 47 million Americans are uninsured • Many are underinsured - lack comprehensive coverage egs preventive care, long-term care & drug costs • 45, 000 die a year from lack of coverage • Markets are good for many things, but they are not a good way to distribute health care
PERSPECTIVE- Practical Current system is unsustainable • Burden it places on our economy/businesses • Private health insurance premiums are at unsustainable rate of 13%/year – & as much as 25% in some areas of country • Coverage is shrinking, as more employers decide to cap their contributions to health insurance & workers find they cannot pay their rapidly growing share • Most expensive health care system in the world
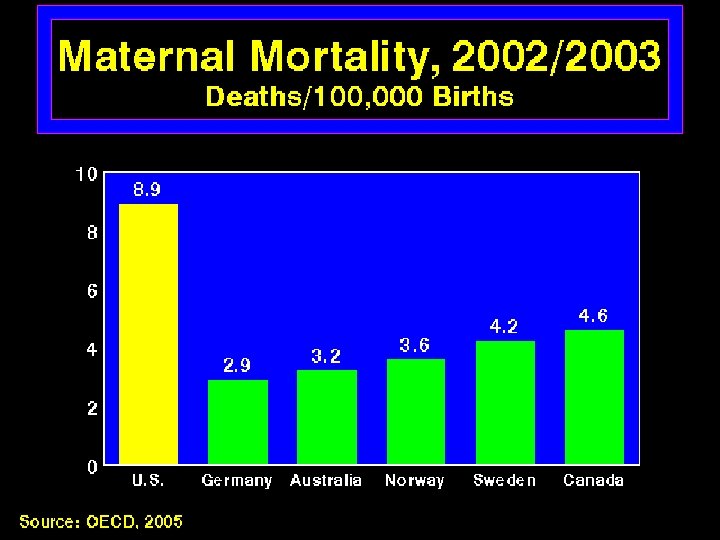
PERSPECTIVE - Practical • Spend twice as much as other developed nations • But we don’t get more care - Canadians, see their doctors more often & spend more time in hospital • We don’t get better results - do worse than most other developed countries on usual measures of health such as life expectancy, infant mortality, immunization rates • & we still don’t cover everyone - 47 million uninsured • In sum, our health care system is outrageously expensive, yet inadequate. Why? • There’s something enormously inefficient about the way we finance & deliver health care
Problem with For-Profit Payers • Investor-owned firms compete not by quality or costs, but by avoiding unprofitable patients & limiting services • Creates paradox of a health care system based on avoiding the sick • It generates huge administrative costs, which, along with profits, divert resources from clinical care to demands of business. • Doctors & hospitals maintain costly admin staff to deal with bureaucracy • Adminstration consumes 31% of our health care $
Solution - Single-Payer • Simpler & more efficient than our private health care system • Health care $ distributed by one entity, so that health care could be coordinated to eliminate gaps • Conceptual extension of Medicare to entire population. • Medicare is: • Government-financed single-payer system embedded within our private, market-based system. • Most efficient part of our health-care system, with overhead costs of < 3% • Covers virtually everyone over 65 • Most popular part of U S health care system
Solution - Single-Payer • Universal, Comprehensive Coverage • No out-of-pocket payments Co-payments & deductibles are barriers to access, administratively unwieldy, & ineffective for cost containment • Single insurance plan in each region, administered by public or quasi-public agency • Global operating budgets for hospitals, nursing homes, allowed group & staff model HMOs & other providers with separate allocation of capital funds Billing on per-patient basis creates unnecessary administrative complexity & expense. A budget separate from operating expenses will be allowed for capital improvements
Key Features of Single-Payer • Free Choice of Providers Patients should be free to seek care from any licensed health care provider, without financial incentives or penalties • Public Accountability, Not Corporate Dictates The public has an absolute right to democratically set overall health policies & priorities, but medical decisions must be made by patients & providers in the region rather than dictated by corporate executives. Market mechanisms principally empower employers & insurance bureaucrats pursuing narrow financial interests • Ban on For-Profit Health Care Providers Profit seeking inevitably distorts care & diverts resources from patients to investors • Protection of health care & insurance workers
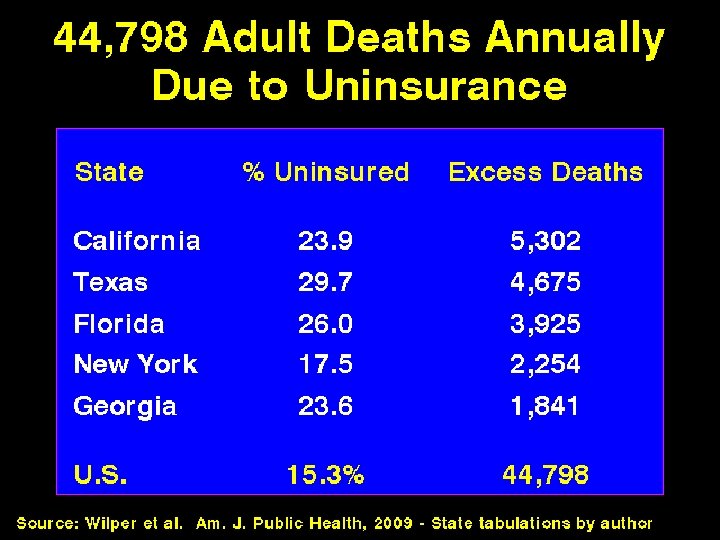
47 Million Uninsured 45, 000 Deaths Per Year But simply helping them buy private insurance is not a
Meet Thomas Wilkes • Born in 2004 with Severe Hemophilia A. • Dad: Senior Engineer at a small high-tech computer firm with good benefits. • 2005: Develops an inhibitor to his hemophilia treatment. • $750, 000 annual claims.
Private Insurance for Thomas • • Company faces 40% to 55% in premiums. Only insurer that will cover them requires $10, 000 out-of-pocket & $1 million cap. • Thomas is projected to reach the $1 million benefit cap in summer 2009 • Options 1. Dad can quit job he loves & work for megafirm that will take longer to be affected by high claims 2. Mom can go to work for a mega-firm. 3. Thomas’ father can divorce his mother to leave her & Thomas legally destitute & eligible
Who Are the Uninsured? » Children » 25% » Employed » 50% » Unemployed » 5% » *Out of labor force » 20%
“…, people have access to health care in America. After all, you just go to an emergency room. ” -No Longer President Bush
America’s Underinsured Proportion of Americans Going Without Care due to Costs, 2005 (skipping doctor visit, specialist appointment, treatment or prescription when needed) Source: Commonwealth Fund Biennial Health Insurance Survey, 2005
Medical Bankruptcy Illness & Medical Bills Contributed to 1, 000 Personal Bankruptcies in 2004. (Half of All Bankruptcies) Insurance Status at Onset of Illness Uninsure d Had Insurance Source: Himmelstein, Health Affairs 2005 (state estimates provided by author)
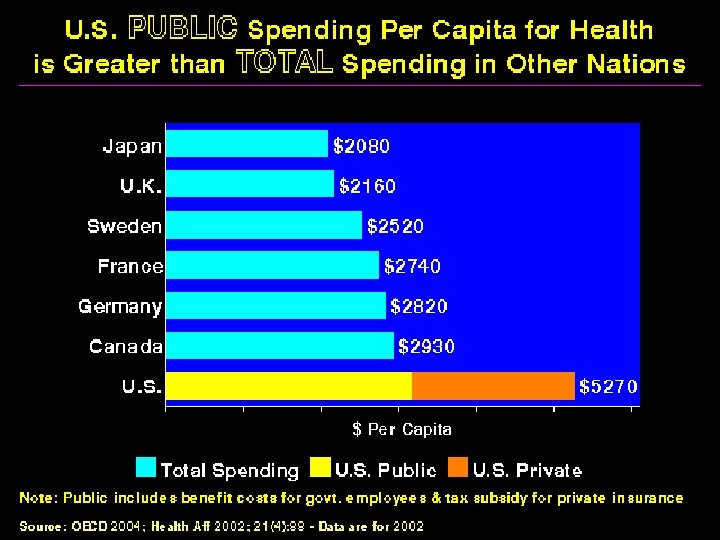
International Health Spending, U. S. Public Spending is 2005 Greater than Other Nations’ Public/Private Spending Combined Source: OECD 2007; Japan data are from 2004
The Healthcare Americans Want • Guaranteed access • Free choice of doctor • High quality • Affordability • Trust & respect
Other Industrialized Nations • • Have similar demographics Availability of expensive technology Rising drug costs Similar levels of service Why are their costs so much lower?
Why are costs lower in other countries? • Administrative simplicity • Lower prices • Higher ratio of primary care to specialists • Health planning • Global budgets
If you were in an insurance CEO, who would you want to insure? 73% Percent of health Care Costs 80% uses less than $1000 of care per year 0% 0% 0% 1% 1% Source: Agency for Healthcare Research & Quality MEPS 2% 4% 6% 13%
The Health & Profitable to the “Market, ” the Sick & Poor to the Taxpayer 73% Government Programs Percent of health Care Costs Private Insurers 0% 0% 0% 1% 1% Source: Agency for Healthcare Research & Quality MEPS 2% 4% 6% 13%
Rising Costs = Less Benefits = Under/Uninsurance Proportion of Americans Covered by Employer Insurance Source: US Census
Life Expectancy, 2005 (Data in Years)
Infant Mortality, 2005 (Deaths in first year of life per 10, 000 live births)
Growth of Physicians & Administrators 1970 -2005 Source: Bureau of Labor Statistics & NCHS
One-Third of Health Spending is Consumed by Administration 31% Potential Savings: $350 billion per year Enough to Provide Comprehensive Coverage to Everyone Source: Woolhandler, et al, New England Journal of Medicine, August 2003 & Int. Jrnl. Of Hlth. Services, 2004
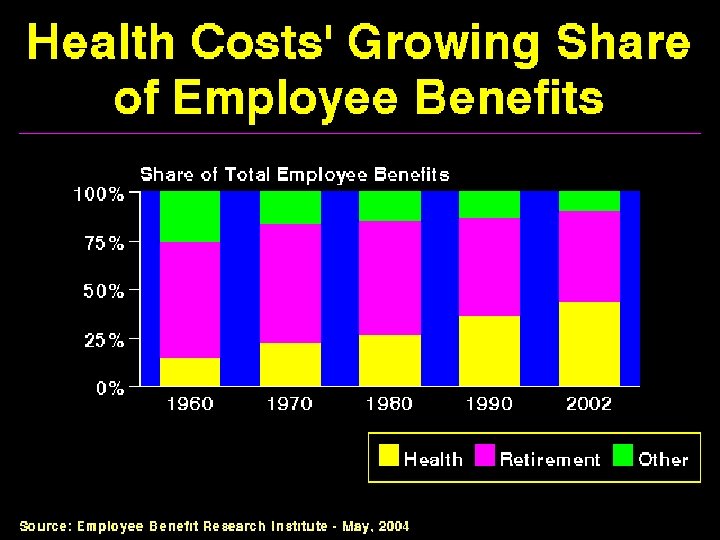
Costs to Business Skyrocketing costs for health care hurting U. S. business: • Health care cost General Motors $5. 6 billion in 2005 adding $1500 to the price of each car • Companies that offer coverage often pay 10% or more of payroll on health benefits and are at a disadvantage competing with companies that don’t offer coverage or where there is public coverage • Toyota located a new plant in Canada and Lifesavers moved a Michigan factory to Ontario
GM retiree cost is $60 Billion! Source: Wall St. Journal, March 11, 2004
Lesson #1: Simply Giving More People Existing Private Insurance Policies Is Not Solution: • Current Private Insurance Policies Offer Inadequate Protection. • Any Gains in Coverage Will Be Quickly Offset as Costs Rise & Employers Shed Benefits. Lesson #2: Real Solution to Health Crisis Must Do 2 Things: 1) Offer Coverage More Comprehensive than that Currently Available on the Private Market. 2) Control Costs so that Benefits are Sustainable.
Only Two Paths to Reform 1. Preserve Private Insurance Companies & their Waste 2. Create a National Health Insurance System
Single-Payer Benefits • Comprehensive Coverage for all medically necessary services (doctor, hospital, long-term care, mental health, vision, dental, drug, etc. ) in a single-tier system. • Free Choice of doctor & hospital. • Health Workers Unleashed from corporate dictates over patient care. • Hospitals guaranteed a secure, regular budget.
Financing Single-Payer Medicare Medicaid Payroll Tax Single-Payer Health Care Fund $$$ Income Tax Bonus: Negotiated formulary with physicians, global budget for hospitals, primary & preventive care, bulk purchasing of drugs & medical supplies = long term cost control.
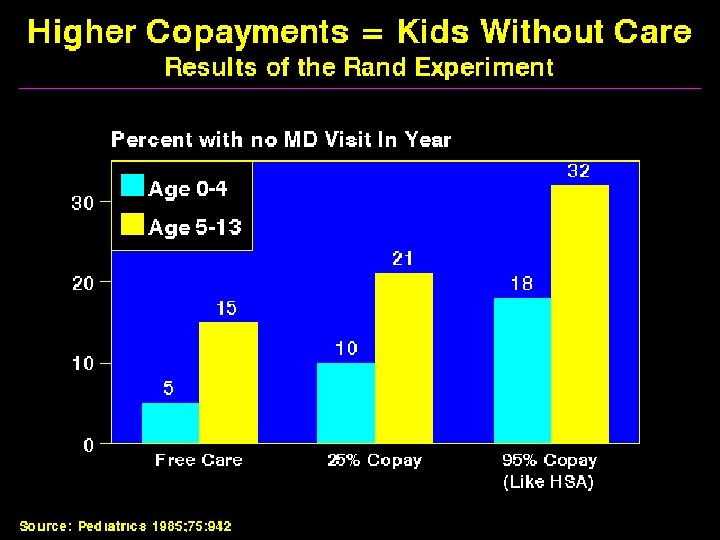
Health Savings Accounts • A bank account in which a limited amount of money may be deposited tax-free for expenditures on health services. • Must be paired with a “high-deductible” health plan. (e. g. , $5, 000). • First few thousand dollars are paid from the HSA, at some point, “catastrophic” coverage kicks in. • Theory: Patients now using “their own money” = better consumers = lower costs.
High-Deductibles = No Savings 73% Percent of health Care Costs 0% 0% 0% 1% 1% Source: Agency for Healthcare Research & Quality MEPS 2% 4% 6% 13%
Health Savings Accounts Won’t • Provide Meaningful Choice for Patients • Reduce Administration • Produce Savings Health Savings Accounts Will • Discourage Preventive & Primary Care • Create Huge New Administrative Waste • Produce Few Savings (a few sick people cost the most)
“Individual Mandate” “Let them buy insurance. ”
Criminalizing the Uninsured: A Massachusetts Punitive Index # The Crime 1 2 3 4 5 6 7 The Fine Violation of Child Labor Laws $50 Illegal Sale of Firearms, First Offense $500 max. Driving Under the Influence, First Offense $500 min. Domestic Assault $1000 max. Cruelty to or Malicious Killing of Animals $1000 max. Communication of a Terrorist Threat $1000 min. Being Uninsured* $1500 min. *Note: Original version of House Bill would have suspended individuals’ driving licenses for uninsurance as well.
Subsidy & Individual Mandate Schemes • Substandard Coverage: forces uninsured to buy defective insurance industry products that are already causing families to face bankruptcy & go without needed care. • Unaffordable: Without savings achievable with single-payer, taxes must raised or funds diverted from other needy programs. • Micro-coverage, Macro-costs: Preserves wasteful private insurers & adds yet another layer of state administrative waste. Rather than provide care to uninsured through a relatively efficient program like Medicare, the plan launders tax dollars through wasteful private insurers. • No Realistic Cost Control: Any gains in public coverage will be unsustainable due to rising costs.
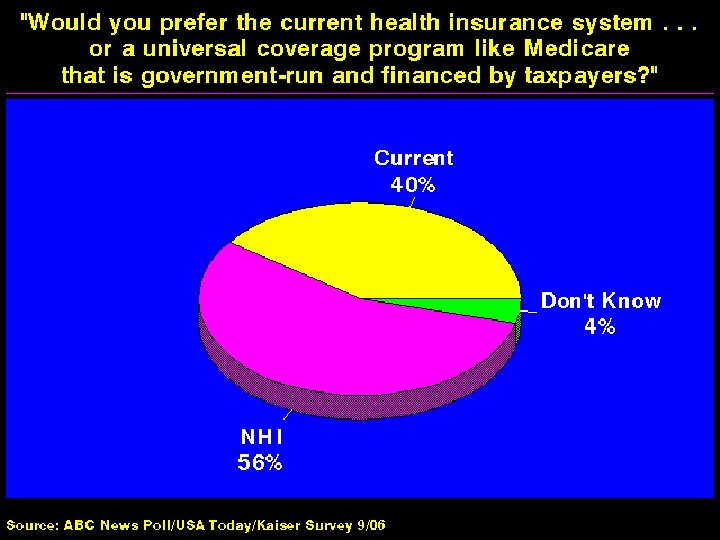
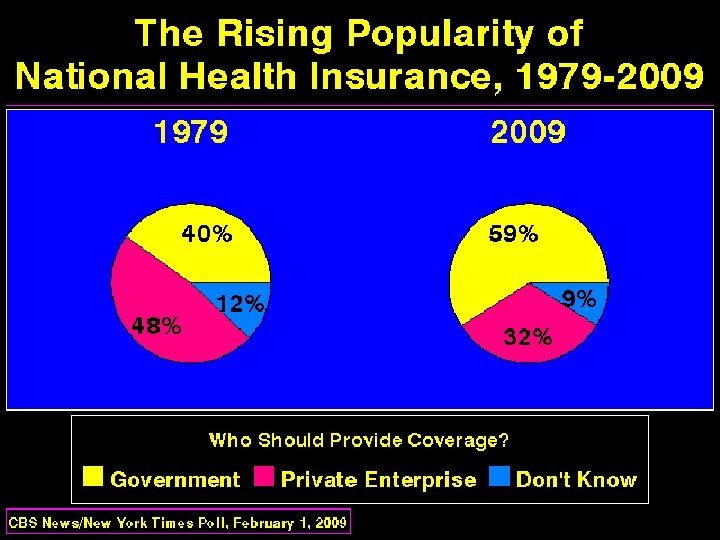
“Sounds Great, but it’s not politically feasible” • 2/3 rds of population want it • Most (59 percent) of physicians want it • Business community is now realizing the need for it.
Single-Payer: Glen Barton Former CEO, Caterpillar Inc. (Fortune 100) Past Chairman, Health & Retirement Task Force Business Roundtable Represents 150 Largest Employers Total Assets: $4. 0 Trillion “The quickest & simplest solution… is to go to a single-payer system” - Written Testimony to AHCTF, Feb. 1 2006
“If done right, health care in America could be dramatically better with true single-payer coverage. ” -Ben Brewer, WSJ, April 18, 2006 “[single-payer] is an idea that's so easy to slam politically yet so sensible for business that only Republicans can sell it! …it may take a Republican President to bless the socialization of health spending we need. ” -Matt Miller, Fortune, April 18, 2006 CNBC / MSN Money “Think, as a small business, how you could benefit from a single-payer system: you wouldn’t lose potential employees to larger firms that offer more attractive health benefits; health insurance costs would cease to be a line item in your budget. A serious illness befalling you or an employee wouldn’t be a companywide financial crisis. You might even save money. ” -Joseph Antony, CNBC / MSN Money, Winter 2003
Is “The Perfect the Enemy of the Good? ” • The central flaws of the “Obama” plan remain the central flaws of our current system – Uncontrolled Costs – Lack of Universal Coverage • Without eliminating the overhead of a patchwork for-profit system we will not achieve the system we deserve
Is “The Perfect the Enemy of the Good? ” The Radical & the Republican “Many of Lincoln’s admirers have painted him as a man who wanted exactly what the abolitionists did but cannily waited for a perfect moment to achieve it. [In fact], radicals like Douglass set an agenda Lincoln gradually adopted as his own. Without abolitionists, there would have been no Lincoln. ”
Single-Payer: “Politically Feasible? ” Other “Politically Infeasible” Movements Abolition of Human Slavery (1860 s) Women’s Suffrage Movement (1840 -1920) Civil Rights Act (1964)