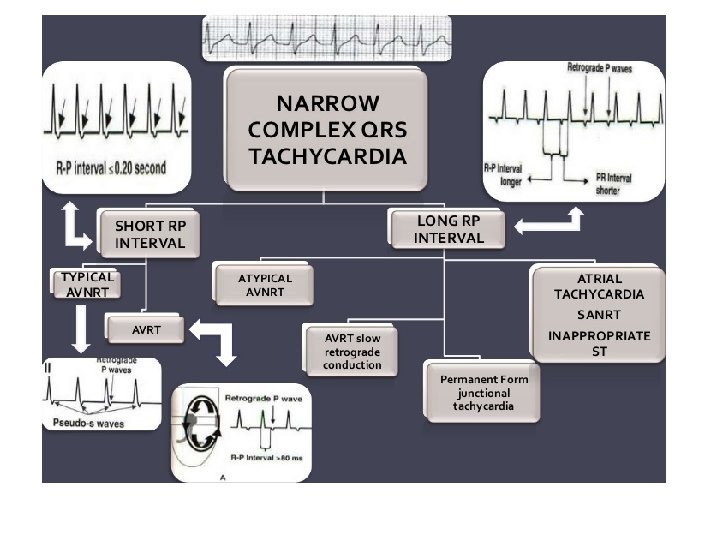
Approach to narrow QRS tachycardia The normal RMP

















 rate 240 -350/mt can be entraine d")







 ERAA Typical AVNRT(slow – fast) ˃1 ˂60 ms RHs,")







- Slides: 65
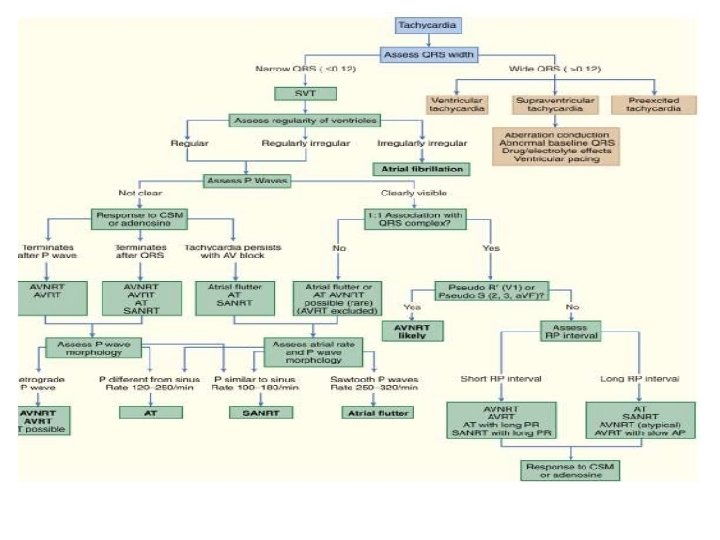
Approach to narrow QRS tachycardia
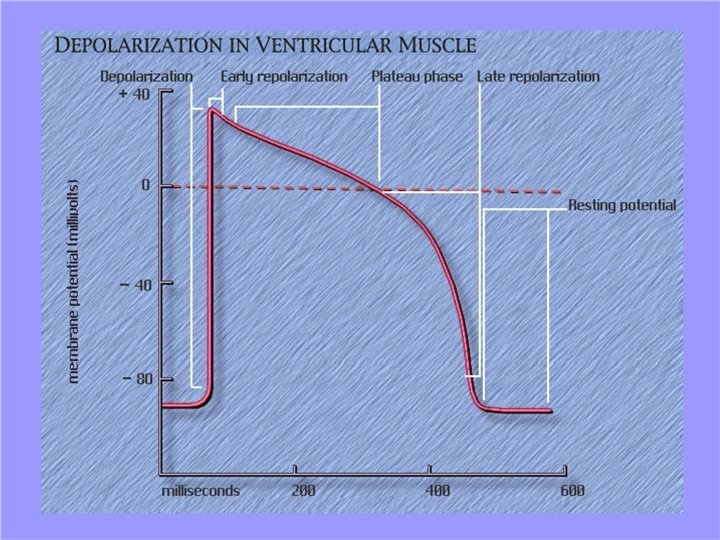
Ø The normal RMP in myocardium is -90 mv Ø SA node differs from myocardium by Ø RMP is -65 mv Ø low overshoot Ø short duration Ø The phase 1 repolarisation corresponds to isoelectric ST segment of ECG
RELATIONSHIP OF INTRACELLULAR POTENTIAL TO SURFACE EKG
RELATIONSHIP OF INTRACELLULAR POTENTIAL TO SURFACE EKG SN P VP ARP RRP
RELATIONSHIP OF INTRACELLULAR POTENTIAL TO SURFACE EKG
Properties resposible for any arrythmia is abnormal automaticity conductivity refractoriness
Mechanism of Tachyarrhythmia Abnormal impulse formation Automaticity Enhanced Abnormal impulse conduction Reentry Triggered EADs DADs Anisotropy Anatomic F
CLINICAL EVALUATION • • • History Palpitations - Greater than 96% Dizziness - 75% Shortness of breath - 47% Syncope - 20% Chest pain - 35% Fatigue - 23% Diaphoresis - 17% Nausea - 13%
• CLINICAL CLUES FROM • PULSE • JVP • HEART SOUNDS
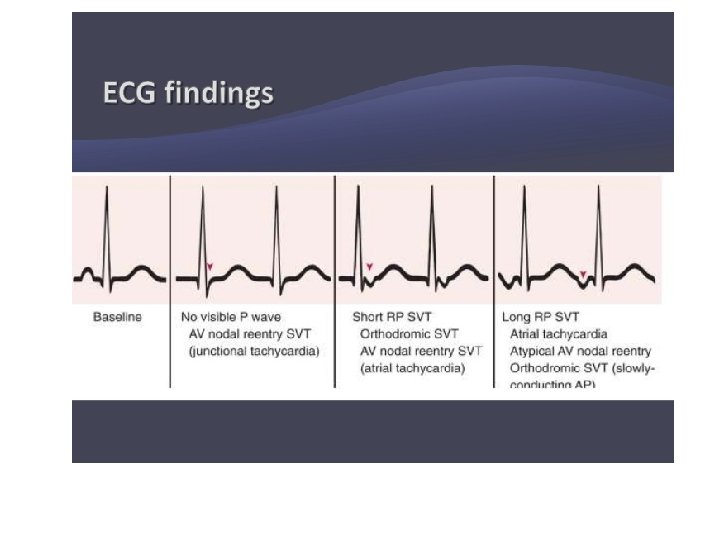
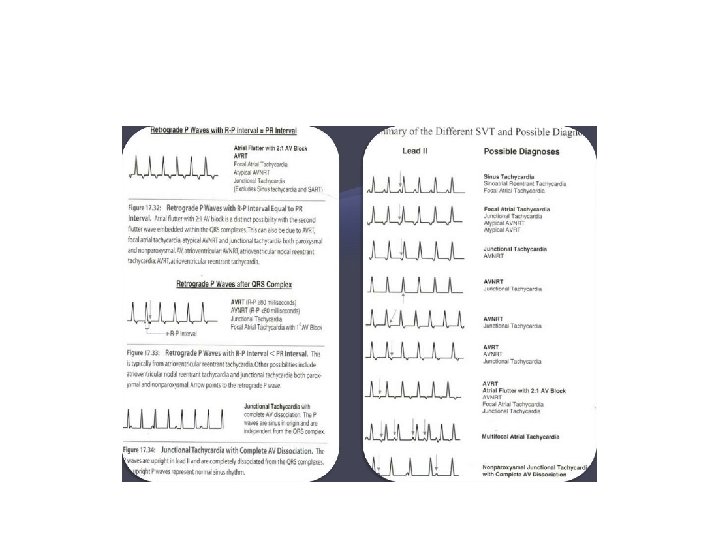
• Diagnosis of arrythmias is made by • rate and regularity of P wave, P-P interval • relationship of P and QRS • configuration of P and QRS
If the P wave is not found modifications LEWIS lead RA to Rt 2 nd ICS LA to Rt 4 th ICS Esophageal lead Intracardiac lead
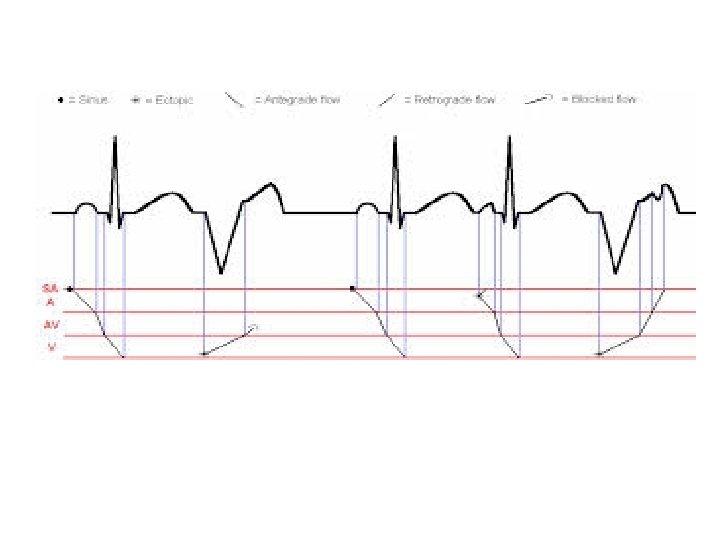
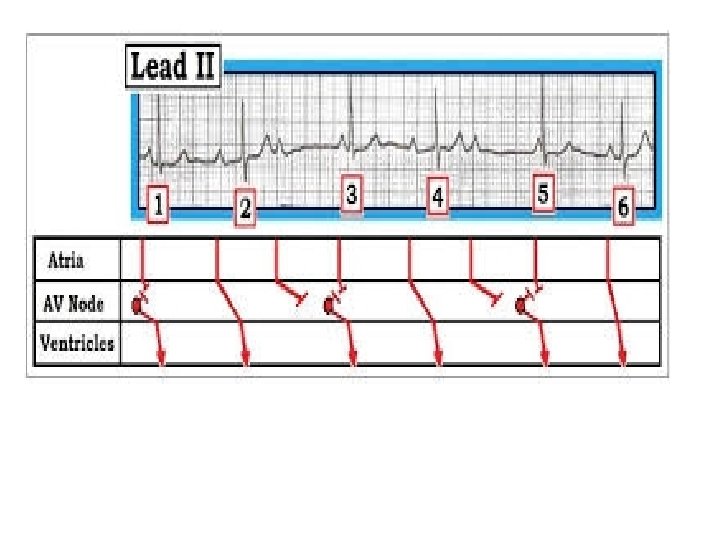
LADDERGRAM OR LADDER DIAGRAM • Depicting temporal relationship between atrial and ventricular repolarisation • Timing correlates with ecg in horizontal direction • A---- Pwave duration • A-V ------P-R segment • V------QRS duration
Approching ECG
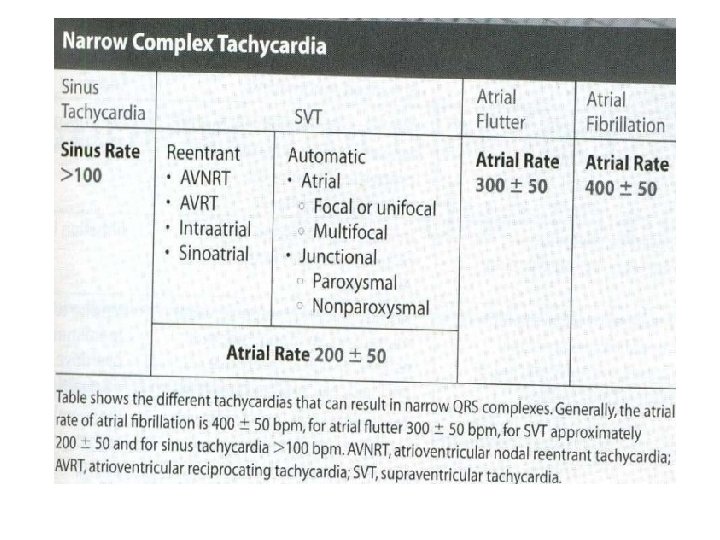
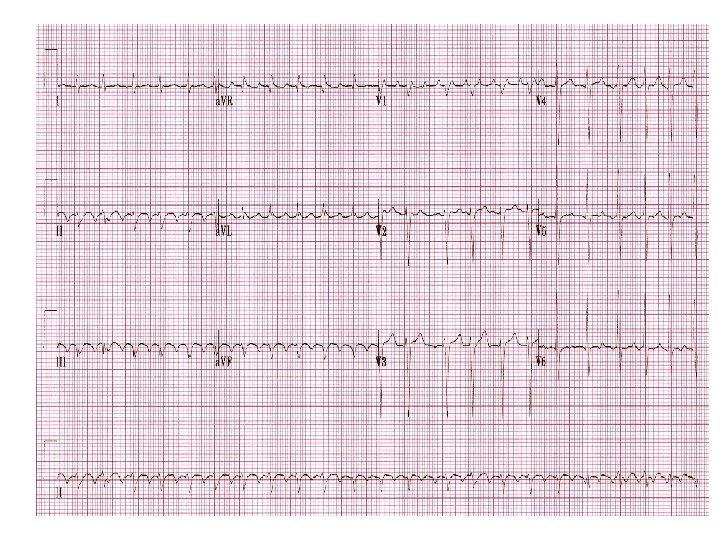
Atrial flutter features • Rapid , regular atrial rhythm at a rate of 200 -400/min • Waves are regular , uniform amplitude in morphology and amplitude. No iso electric segment in between • Usually 2: 1 or 4: 1 conduction to ventricle • Wenkebach type conduction can occur • 1: 1 conductive response suggests Accesery pathway Class 1 A, 1 C drugs slowing rate of AFL (Hence Class IA and IC drugs should be administered in conjunction with an AV nodal blocking agent (beta blocker or calcium channel blocker) of Catecholamine excess like exercise, excitement, induction Anesthesia IV atropine
• Usually transient • Associated with underlying structural heart disease • Digoxin convert AFL to AF • Sodium blocking drugs convert AF to AFL then to sinus rhythm • Markedly enlarged atria tend to have slow rate • Ectopic atrial tachycardia and AFL seldom coexist in same pt
Mechanisms • A large or small re entrant loop • Single or multiple focus of automaticity • “Isthmus of slow conduction” It is in postero septal part of rt atrium betwn orifices of IVC, coronary sinus , tricuspid annulus ring – It is the promising target for ablation to interrupt AFL : Ablation is commonly performed at the 6: 00 position on the tricuspid valve isthmus
Types of atrial flutter Type 1 (common/typical) rate 240 -350/mt can be entraine d byatrial pacing subdivided into counterclock wise (cephalad)(Most common) inverted in Lead 2, 3, a. VF positive in V 1 clockwise (cranial to caudal) positive in Lead 2, 3, a. VF either positive or negative in V 1 Type 2 (less common) rate 340 -430 cant be entrained by pacing
Type I Atrial Flutter • Typical atrial flutter, or "isthmus-dependent" flutter, is a macroreentrant arrhythmia that involves a long slow path with an excitable gap, forming a circuit within the right atrium. • Slowly conducting reentrant circuit is located in the low right atrial isthmus. • The isthmus of tissue is between the inferior vena cava and tricuspid annulus.
Type I
Type I
Type II Atrial Flutter • Atypical atrial flutter lacks an excitable gap and is not isthmus-dependent. • Usually this rhythm results from an intra-atrial reentrant circuit that is very short. • May be due abnormal anatomy within the right or left atrium (i. e. surgical scars, irregular pulmonary veins, disturbed mitral annulus)
Diagnosis: EKG • EKG will typically show 2: 1 conduction across the AV node (even ratios of conduction are more common than odd ratios) – May need to administer adenosine to slow conduction through AV node
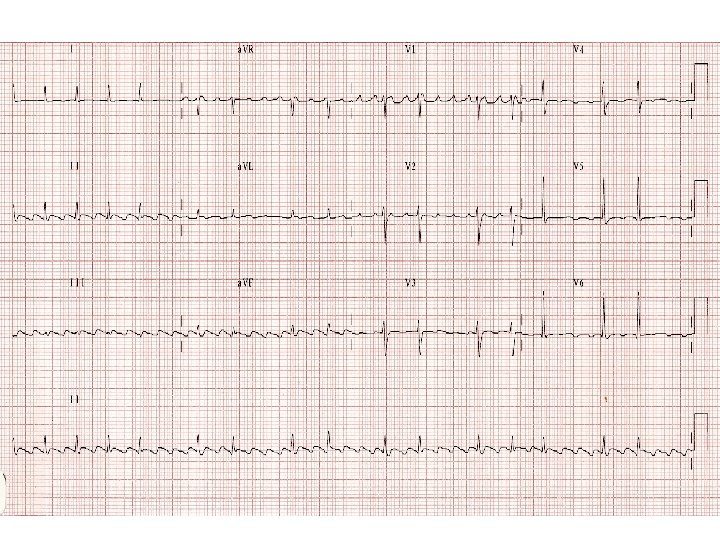
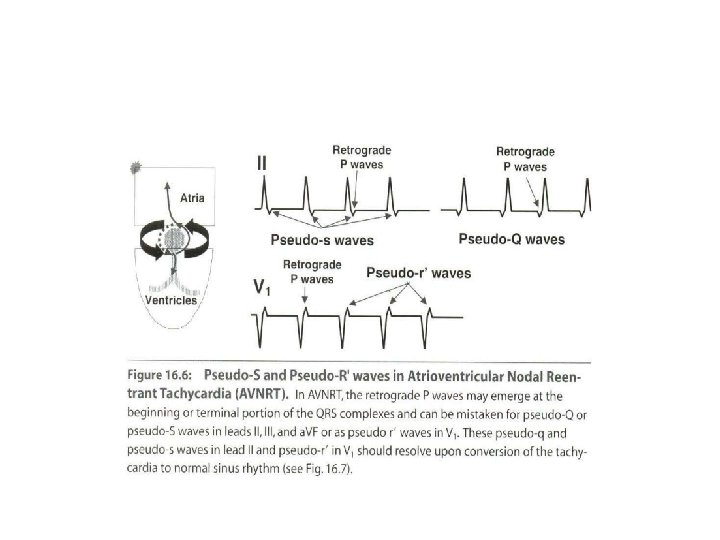
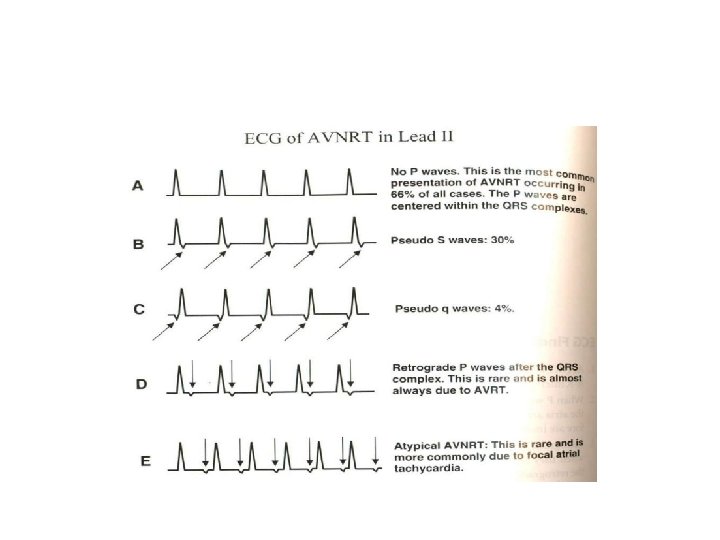
Typical Atrioventricular Nodal Reentry tachycardia ( AVNRT(
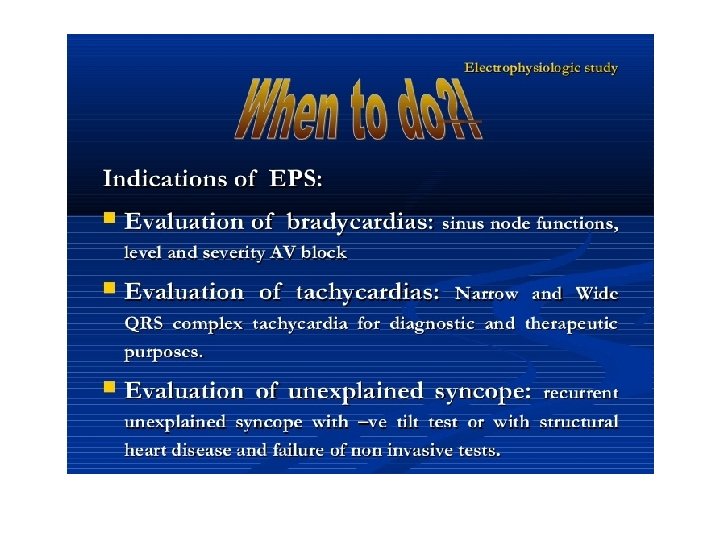
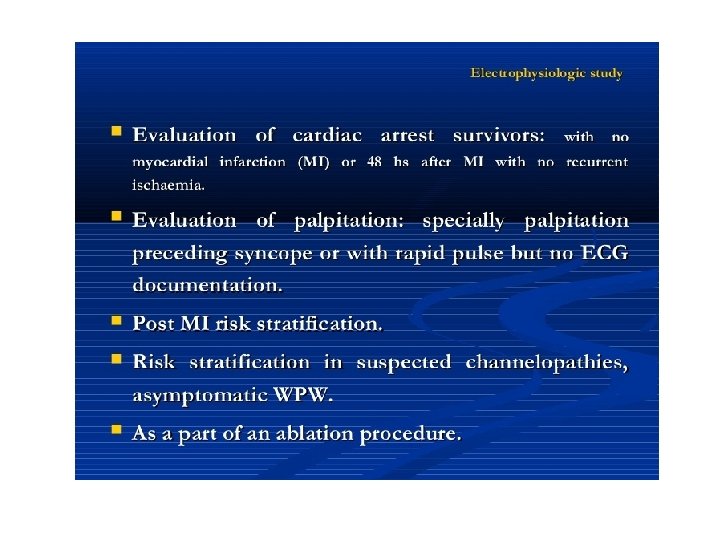
Electrophysiology study
CLASSIFICATION OF AVNRTS AH/HA VA(Hs) ERAA Typical AVNRT(slow – fast) ˃1 ˂60 ms RHs, CS os, LHs Atypical AVNRT(fastslow) ˂1 ˃60 ms CS os, LRAS, d. CS Atypical AVNRT ˃1 (slow-slow) ˃60 ms CS os, d. CS VA indicates interval measured from the onset of ventricular activation on surface ECG to the earliest deflection of the atrial activation in the His bundle electrogram; ERAA, earliest retrograde atrial activation; RHis, His bundle electrogram recorded from the right septum; LHis, His bundle electrogram recorded from the left septum; LRAS, low right atrial septum; CS os, ostium of the coronary sinus; and d. CS, distal coronary sinus. *Variable earliest retrograde atrial activation has been described for all types of AVNRT