JUNCTIONAL RHYTHMS Judy Santo RN BSN Junctional Dysrhythmias

JUNCTIONAL RHYTHMS Judy Santo RN BSN

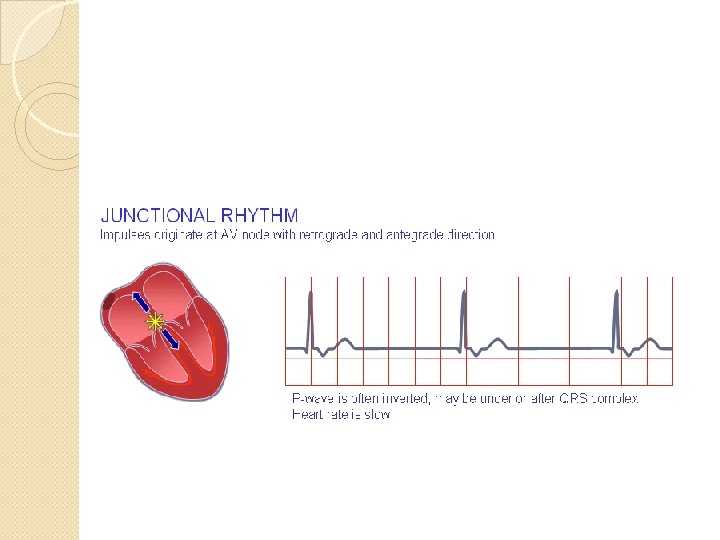
Junctional Dysrhythmias �Ectopic impulse originates at A-V Junction � Supraventricular—see narrow QRS �Ventricular rate regular �Analyze the P wave: ◦ Inverted before QRS ◦ Inverted after QRS ◦ Absence of P waves

Junctional Rhythm Origin

Junctional Rhythm �Regular rhythm-- Vent rate 40 -60/min �P waves will be inverted before or after the QRS, or absent �QRS should be narrow-supraventricular

Junctional Rhythm

Junctional Rhythm

Causes and Treatment of Junctional Rhythm �May be caused by disease of the SA node, increased vagal effect on the SA Node, an acute MI, or drugs (digitalis, quinidine, a beta blocker, or calcium channel blocker). Can also occur with complete heart block. �The slow rate and loss of atrial kick may cause a decrease in cardiac output. Treatment of symptomatic Junctional rhythm includes increasing the heart rate with atropine or pacing. �Identify and correct the underlying cause.

Premature Junctional Contractions �Premature beats �Premature P wave will be inverted before, after or hidden in the QRS— see no P wave �PR interval is less than. 12 sec �QRS duration normal and looks like sinus QRS

Premature Junctional Contraction

Premature Junctional

Premature Junctional Beat with inverted P after the QRS

PJC’s �Causes of PJC’s include digitalis toxicity, enhanced automaticity of the AV Junction, coronary artery disease, heart failure, and valvular disease. May occur without apparent cause. �PJC’s do not normally require treatment. �PJC’s may initiate more serious junctional dysrhythmias

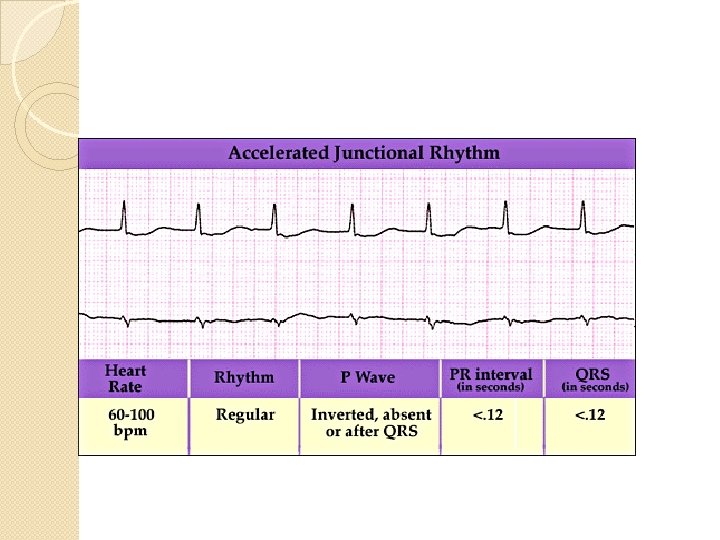
Accelerated AV Junctional Rhythm �Ventricular rate is 60 -100 �P waves inverted before, after, or buried in the QRS �Short PR--. 12 sec. �Accelerated Junctional Rhythm: Vent Rate is 60 -100 with inverted Ps before, after, or no P wave

Accelerated Junctional or Junctional Tachycardia

AV Junctional Tachycardia �Ventricular Rate is Greater than 100 �Ventricular rhythm is regular �P waves are inverted before, after the QRS, or not present at all.

Junctional Tachycardia

Junctional Tachycardia

Junctional Tachycardia Treatment �Treat similar to PAT—if patient is stable—try vagal maneuver first �Adenosine IV next (6 mg, 12 mg) �Treat recurrence with longer acting AV nodal blocking agents (diltiazem, Beta blockers). �If Junctional Tach has a wide QRS and uncertain if it is SVT or Ventricular, treat with Amiodarone 150 mg over 10 minutes and prepare for elective synchronized shock.

Unstable Junctional Tachycardia �If patient is hemodynamically unsteady, perform immediate synchronized cardioversion

Junctional Escape are Late Beats

Escape Beats are Late Beats

Escape Beats �Escape beats are more likely to occur as a result of an increase vagal effect on the SA Node �Common after a pause in the underlying rhythm (like sinus arrest or exit block, nonconducted PAC’s) �Escape beats are protective mechanisms to maintain the heart rate �Must find the cause of the initiating pause
- Slides: 24