Opthalmologic Emergencies Dave Dyck R 3 Preceptor Dr

")


 • Range from 20/15 to")







, various")











 • Increase")















































 -cycloplegic -don’t")







 • Rebleeding 4 -38% usually")
 • Slit lamp")












: • Lid margins • Canalicular system involvement")





")

: cool compresses,")







 •")




















- Slides: 143
Opthalmologic Emergencies Dave Dyck R 3 Preceptor: Dr. Bryan Young Sept. 26/02
Objectives: • Briefly review ocular anatomy and exam • Recognize pathology (yeah – pictures!) • Discuss treatment options • Discuss areas of controversy • Slit lamp review
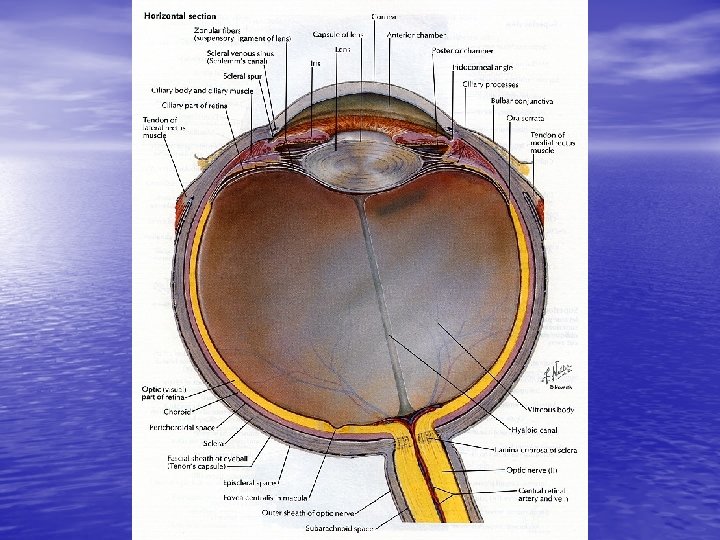
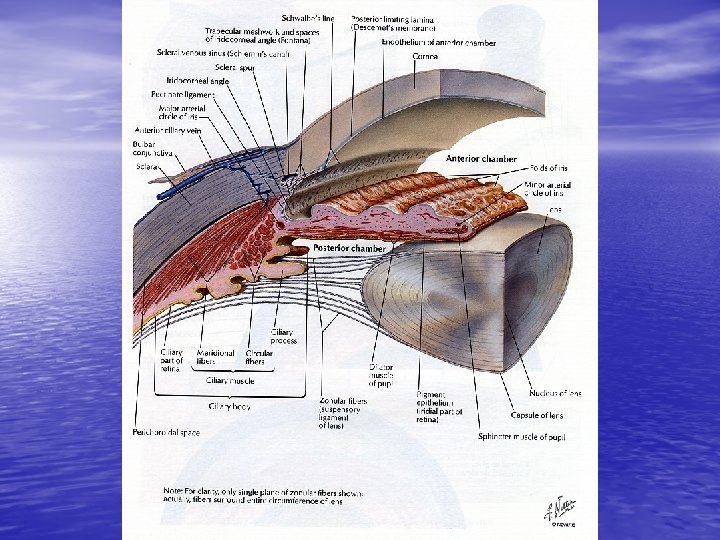
Ocular Anatomy:
Eye Exam: • Visual acuity • Pupils • Motility • Confrontation visual fields • Anterior segment • Posterior segment • Intraocular pressure
Visual Acuity: • Perform at 20 feet (6 meters) • Range from 20/15 to 20/400 then counting • • • fingers, hand movements, light perception, and no light perception Near vision uses a reading card at 14 inches OD= right eye; OS= left eye; OU= both eyes If vision< 20/20 use pinhole to check for correctable refractive errors
Pupils: • Size and reaction to light • Swinging flashlight test – Afferent pupillary defect • Differential= retinal detachment, central retinal artery or vein occlusion, optic neuritis, optic neuropathy • Cataract, hyphema, vitreous hemmorhage, corneal ulcer, and iritis are associated with decreased vision but not an afferent pupillary defect
Pupils cont. • Dilated – Third nerve palsy – Trauma – Adie’s pupil – Drug induced (dilating drops) – Acute glaucoma
Pupils cont. • Constricted – Drug induced – Iritis – Horner’s syndrome * Anisocoria >4 mm seen in 19% of normals
Motility:
Confrontation Visual Fields: To help localize lesions to the retina, optic nerve, optic chiasm, or visual cortex
Anterior Segment: • Lids, puncta, conjunctiva, sclera, cornea, anterior chamber, and lens • Fluorescein – Remove contact lenses
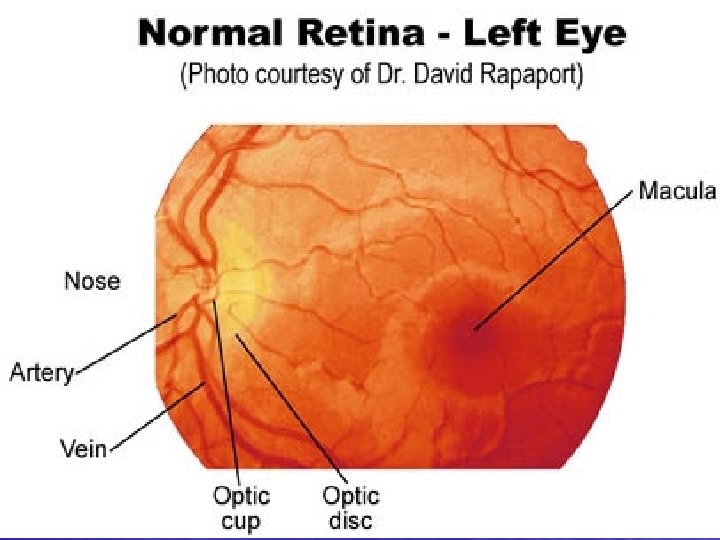
Posterior Segment: • Vitreous, disc, vessels, macula, and peripheral retina • Through dilated pupil UNLESS shallow anterior chamber (or hx of angle closure glaucoma), iris supported intraocular lens (rare), head injury, ruptured globe
Optic Disc: • Normally slightly oval in the vertical meridian, central depression (cup), various pigmentation • Cup-to-disc ratio <0. 5 • Distinct disc margins
Intraocular Pressure: • Normal < 23 mm. Hg. • Acute angle glaucoma often > 40 mm. Hg. • Tonopen- easy • Schiotz tonometry (Roberts) • Applanation tonometry • Air-puff tonometry
Case 1: 66 y lady watching TV tonight in a dark room. Took 50 mg Benadryl for itch increased eye pain with dec. vision
Glaucoma: • Imbalance of aqueous humor production and drainage leading to increased intraocular pressure optic neuropathy
Types: • Primary angle closure glaucoma • Secondary angle closure glaucoma • Primary open angle glaucoma • Secondary open angle glaucoma
Acute Angle Closure Glaucoma: • Symptoms: Redness, severe pain, headache, • • photophobia, decreased vision, halos, +/- N/V Signs: Increased IOP, acute anterior angle, corneal edema, conjunctival injection, nonreactive or sluggish mid-dilated pupil More common if history of far-sightedness (Hyperopia), Asian/Eskimo descent
Treatment: • Pilocarpine 2% - 1 drop q 15 min until pupillary • • constriction. (+ 1 drop q 6 h in unaffected eye for prophylaxix) Timolol 0. 5% - 1 drop (works within 30 -60 min) Apraclonidine HCl 1% - 1 drop Diamox – 250 -500 mg po q 6 h or 500 mg IV If not < 35 mm. Hg in 30 -60 minutes give Mannitol 20% - 2 -7 ml/Kg IV or isosorbide 1 -1. 5 g/Kg po
Treatment cont. • Opthamology : for peripheral iridectomy or laser iridotomy • When to refer urgently for surgery? • When to expect a pressure drop with medications? • What is a satisfactory pressure drop?
Primary Open-Angle Glaucoma: • Most common cause of blindness in NA • Due to increased aqueous humor outflow through the trabecular meshwork • Insidious, slowly progressive, bilateral, painless vision loss (peripheral) ie. NOT AN EMERGENCY • Increased cup-to-disc ratio
Fundoscopic lesions:
Case 2: • 58 y male presents with acute vision loss in L eye x 90 minutes.
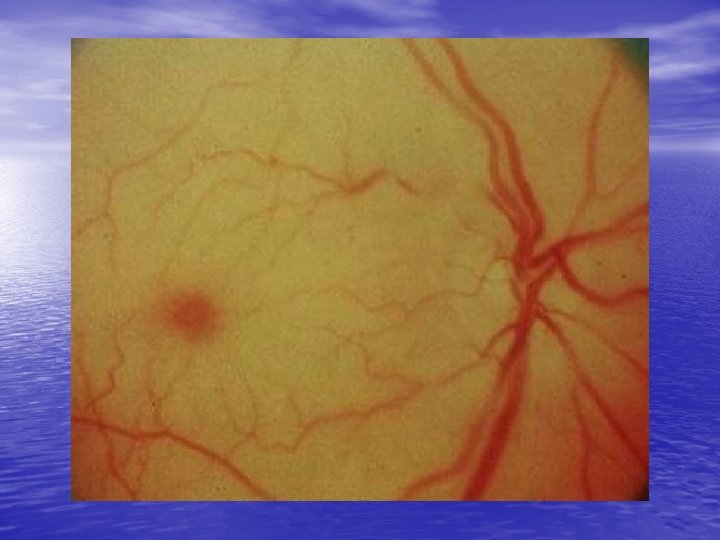
Central Retinal Artery Occlusion: • Painless, ages 50 -70, vasculopathic hx • R/O glaucoma • Signs= Decreased visual acuity, afferent pupillary defect, pale fundus with cherryred fovea • Experimentally, 100 min until irreversible ischemia
Treatment: • Digital global massage (5 sec on – 5 sec off) • Increase PCO 2 by breathing into paper bag for 10 min every hour vs Carbogen • IV acetozolamide + ASA • R/O and Treat glaucoma • Emergent Opthamology referral and outpatient Cardiology • R/O neuritis 2% (ESR, hx, etc)
Case 3: 60 y male with painless blurry vision r eye
Branch Retinal Artery Occlusion: • Same treatment as for CRAO
Case 4: • 60 y female with vision loss L eye
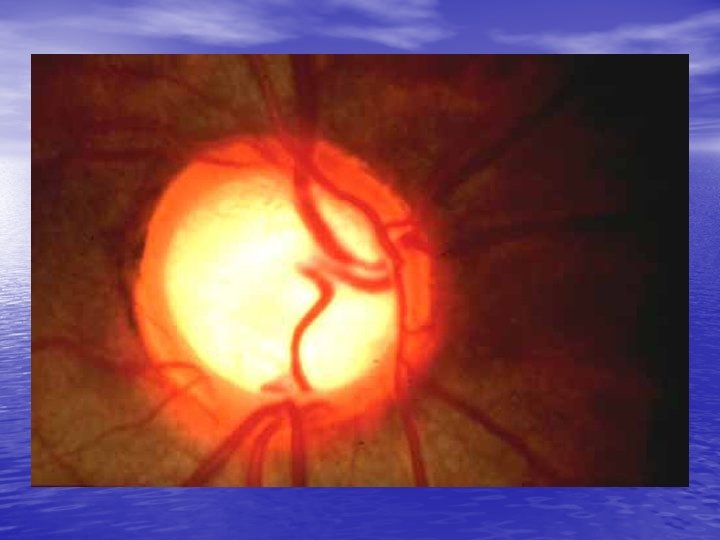
Central/Branch Retinal Vein Occlusion: • Symptoms: variable vision loss, usually painless • Signs: ischemic (neovascular glaucoma) or non-ischemic (macular edema with leaking capillaries) Dilated tortuous veins, retinal hemmorhages and disc edema
Treatment: • Expectant • Referral to Opthomology within 24 hrs to R/O neovascular glaucoma
Case 5: • 55 y myopic male with light flashes and complete vision loss acutely 2 hrs ago in L eye. No pain
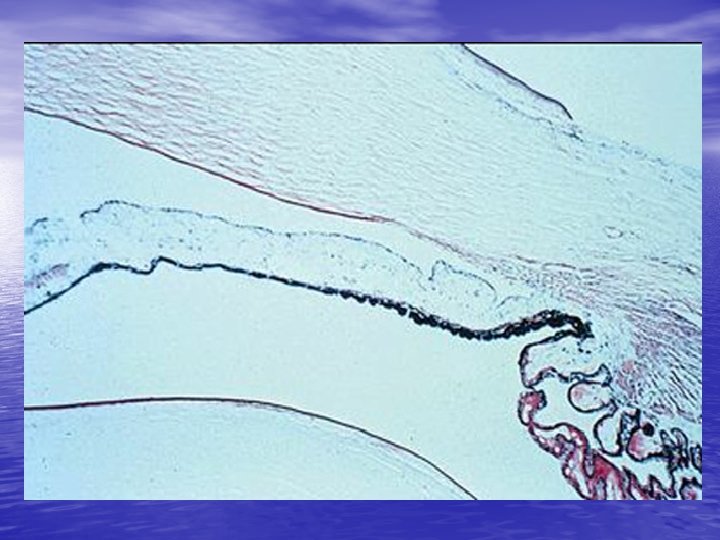
Retinal Detachment: • Separation of the inner neuronal retina layer from the outer retinal pigment epithelial layer • 3 types: – i. rhegmatogenous – ii. Exudative – iii. Tractional
Rhegmatogenous: • Due to tear/hole in the neuronal layer causing vitreous fluid to enter and separate the 2 retinal layers • Often due to vitreous gel pulling on retina as one ages or related to trauma • Men, myopia, age>45
Exudative: • From blood/fluid leakage from vessels within the retina • HT, eclampsia, CRVO, papilledema, vasculitis, choroid tumor
Tractional: • Due to fibrous band formation in the vitreous and the contraction of these bands
Retinal Detachment: • Symptoms: light flashes, floaters, variable vision loss depending on macular involvement (cloudy or curtainlike), painless • Signs: area out of focus on fundoscopy • Cannot be ruled out by direct fundoscopy
Treatment: • Emergent opthamologic consultation • When?
Case 6: • 72 y IDDM female with 2 hr hx of “cobwebs” L eye leading to marked decrease in vision now
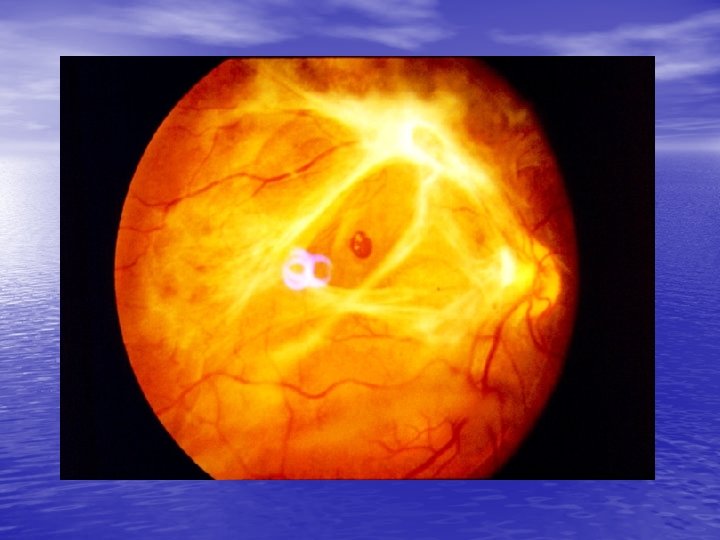
Vitreous Hemmorhage: • Bleeding into the preretinal space or vitreous • • • cavity Usually due to diabetic retinopathy or retinal vessel tears secondary to vitreous collapse but various other causes Symptoms: initially floaters or cobwebs with subsequent vision loss Fundoscopy findings are widely variable (reddish haze to black reflex)
Vitreous hemmorhage: • If afferent pupillary defect present retinal detachment likely behind hemmorhage • Treatment: bedrest, elevate HOB, avoid ASA and refer to opthomology
Case 7: • 75 y male with progressive vision loss x years with acute worsening central vision today. No pain.
Macular Hemmorhage: • Refer to opthomology
Macular Disorders: • Loss of central vision with preservation of • • peripheral vision, central vision distortion, abnormal retinal changes at macula Due to trauma, radiation, inflammation, vascular disease, toxins, genetics, idiopathic Drusen Neovascularization *no afferent defect and optic nerve normal
Drusen:
Macular Star:
ER role: • Recognition primarily and referral to opthamology for fluorescein angiogram within 24 -48 hrs
Non-Penetrating Ocular Trauma: • Orbit and globe • Cornea and conjunctiva • Anterior chamber and iris • Lens • Posterior Segment
Case 8: • 22 y male hit in L eye with puck. Vision slightly blurry (20/60) and decreased up gaze. Tender inferior orbit.
Orbital Wall Fractures: • Orbital floor is weakest point and orbital tissues • • • may prolapse inferiorly enopthalmos, ptosis, diplopia, aneasthesia of ipsilateral cheek/upper lip, and decreased up gaze Medial orbital wall # into ethmoid sinus (look for orbital emphysema) Globe injuries in 10 -25% Facial x-rays (imperfect) – Teardrop sign – AF level
Treatment: • Consultation with plastic surgery for possible surgical repair • Abx unnecessary unless involved sinus previously infected • Avoid nose blowing (dec emphysema)
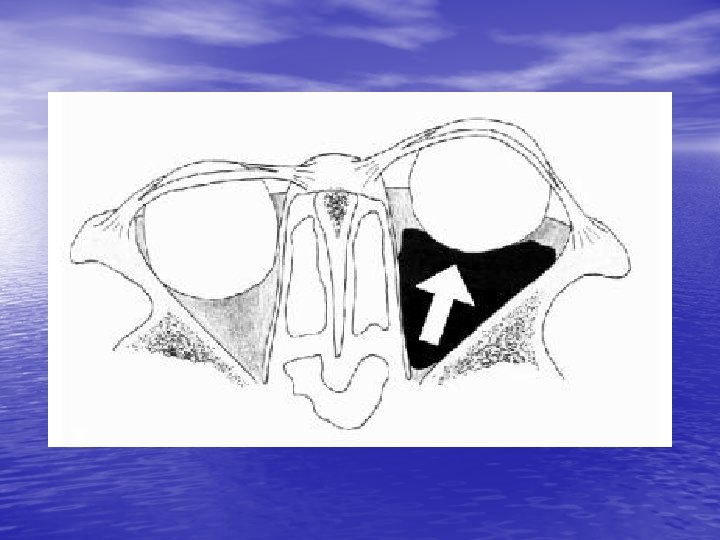
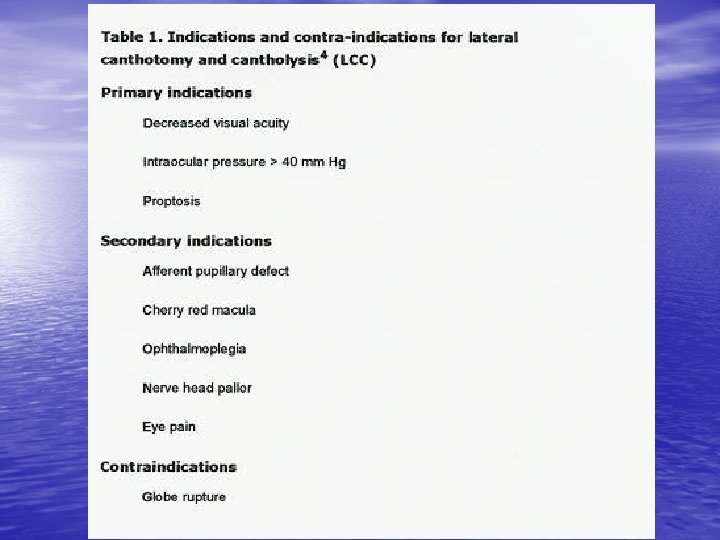
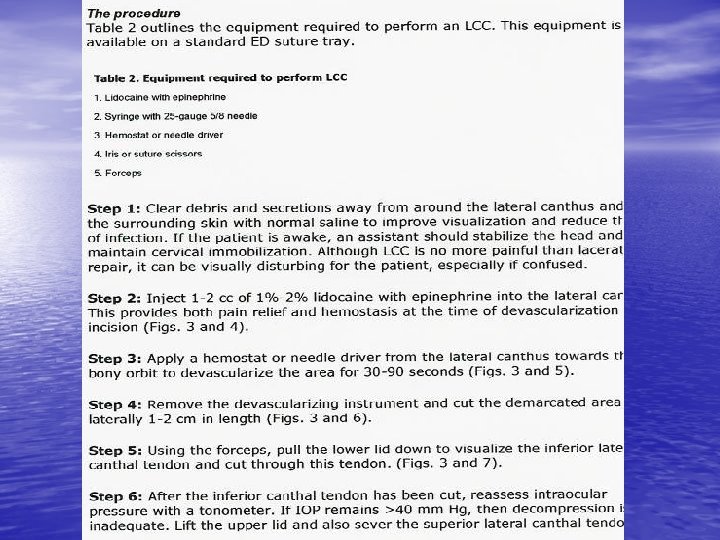
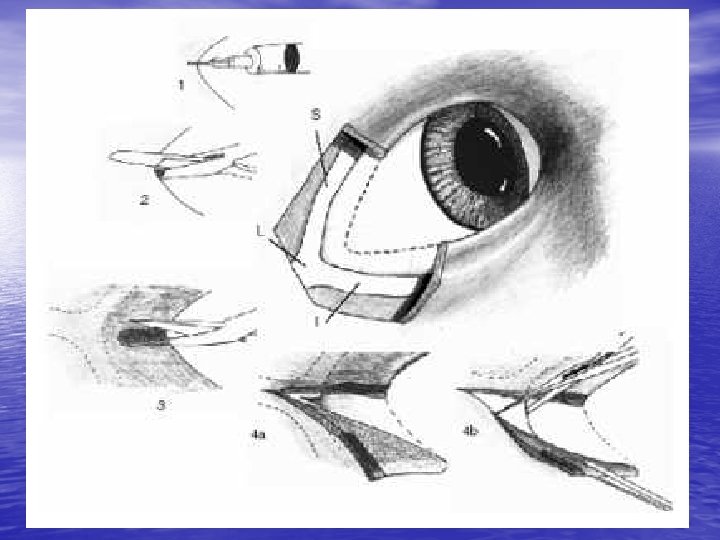
Retrobulbar Hemmorhage: • Hemmorhage in potential space surrounding • • globe may increase intraorbital pressure and cause CRAO. Symptoms=proptosis, visual loss, increased IOP Signs= CRAO Dx= above + orbital CT scan Tx=immediate optho consult, IV mannitol +/lateral canthotomy or anterior chamber paracentesis
Complications: • Infection, hemmorhage, injury to globe • Rare • Canthotomy wounds heal well without suturing or significant scarring
Case 9: 22 y male in MVA
Globe Rupture: • Most common at EOM insertions into sclera or at limbus • Pain and decreased vision • Examination: various = teardrop pupil (iris plugging limbal hole), distortion of anterior chamber, others
Diagnosis: • Hx/Px +/- CT or U/S • Fluorescein • Avoid tonometry
Treatment: • Protective shield, avoid manipulation, NPO, tetanus, IV Abx, urgent opthalmology • Avoid succ or use defasciculator if must use it
Case 10: 32 y male with drain cleaner in eye
Alkali burns: • Liquefaction necrosis • Severe injury= (severity judged by degree of corneal whitening)
Treatment: • Prehospital- copious irrigation with clean water x 15 min prior to transport. Bring in chemical • Hospital- topical anaesthesia, lid retraction and 2 L continuous irrigation NS. Continue until p. H=7. 4 -7. 6. Remove foreign bodies. Urgent optho consult.
Complications: • Perforation, scarring and corneal neovascularization. Lid adhesions, glaucoma, cataracts, and retinal damage
Neovascularization:
Acid burns: • Less devastating • Coagulation necrosis precipitates tissue proteins to limit depth of injury • If p. H>2 usually min damage unless very high concentration or long duration of exposure • Treatment as for alkali burns
Miscellaneous exposures: • Treat as if acid/alkali • Superglue= If eyelids sealed shut in normal position leave alone. If eyelids in abnormal position may require surgery. Optho should see both in consultation
Thermal Burns: • Eyelid usually worse than globe • If superficial treat with irrigation and Abx ointment. If deeper as above + involve optho
Case 11: 16 y male scratched in eye
Corneal Abrasion: • Symptoms: pain, photophobia, foreign body sensation, dec vision. • Signs: injected conjunctiva, fluorescein defect
Treatment: • R/O foreign body and herpes keratitis (evert lids, • • • use slit lamp) Refer immed if pain not relieved with top anaesthetics or if large abrasion esp if in central field of vision Cycloplegics (cyclogyl 1%) Abx drops (sulfacetamide 10%, polytrim, ocuflox, etc) Patch vs no patch (Kaiser 1995; Hart 1997; Patterson 1996) If no patch give topical NSAID for pain control eg ketorolac 0. 5% QIDx 3 d
Contact lens related abrasions: -remove contact lens -gram neg coverage (gentamycin, ocuflox) -cycloplegic -don’t patch -may require opth follow-up so that a corneal ulcer doesn’t develop
Follow-up: • Bring back in 24 hrs or not? • Optho follow-up?
Case 12: 38 y male feels something got in his eye while chopping wood
Corneal foreign body: • Dx. =topical aneasthetic and slit lamp exam • r/o intraocular foreign body • Treatment= irrigation or needle removal (25 guage) and then as for abrasion • Rust ring removal
Case 12: 42 y male with acute redenning of eye after rubbing it. No other sx
Subconjunctival Hemmorhage: • Treatment= reassurance, cool compresses • Resolves in 2 -3 weeks
Case 13: 22 y male struck in eye by squash ball
Hyphema: • Blood in anterior chamber • Due to disruption of blood vessels in the iris or • • ciliary body (trauma or spontaneous) Typically lasts 4 -6 days if uncomplicated Classification: – – Grade 1 = less than 1/3 of ant chamber filled (72%) Grade 2 = 1/3 to ½ (20%) Grade 3 = greater than ½ (5%) Grade 4 = complete filling of ant chamber (3%) v “eight ball hyphema”
Complications • Glaucoma 1/3 (esp if Sickle Cell Anemia) • Rebleeding 4 -38% usually at 2 -5 days • Corneal staining 2 -5%
Management: • Document VA, pupils, IOP, aff pupillary defect (eight ball) • Slit lamp and complete eye exam to r/o other injuries
Treatment: • Shield • Rest, elevate HOB, no straining/bending/valsalva • No near viewing activities eg reading • Control IOP (avoid acetazolamide in Sickle Cell • • Anemia) Stop anticoagulation and avoid ASA/NSAIDs Steroids controversial – leave up to optho Systemic antifibrinolytics (aminocaproic acid) – controversial (dec rebleeding but inc N/V) Cycloplegics ok and tx corneal abrasions w abx
Treatment: • To admit or not? – No answer in literature – Growing opinion to allow grade 1 -11 hyphemas with controlled IOP to be treated at home with close optho follow-up daily
Indications for Surgery: • Uncontrolled increased IOP • Persistent total/near total hyphema x days • Prolonged clot duration • Corneal blood staining • Surgery required in 5%
Traumatic Iridocyclitis: • Contusion to iris/ciliary body ciliary spasm • Photophobia and deep eye pain • Exam= ciliary flush, anterior chamber cells (WBCs and protein) • Tx=long acting cycloplegics x 7 -10 days • Steroids may be given by optho
Case 14: 12 y boy 2 wk f/u post hyphema
Iridodialysis: • Tearing of the iris root from the ciliary body • ED tx- only if hyphema present • May require non-urgent surgical correction
Case 16: Tall thin 32 y male presents with diplopic vision L eye after minor eye trauma
Lens subluxation/dislocation: • Due to trauma, Marfan’s, homocystinuria, and tertiary syphilis • Tx. = optho referral
Anterior chamber lens dislocation:
Penetrating Trauma:
Case 17: 18 y male hit in eye by TV remote
Lid lacerations: • What can ED do? – Simple horizontal and oblique partial thickness lacerations
Complex lid lacerations needing referral (24 hrs): • Lid margins • Canalicular system involvement (medial lower eyelid) • Levator or canthal tendon involvement • Lacs with tissue loss
Conjunctival, Corneal, Scleral lacerations and punctures: • Conjunctival lac: small, superficial no suturing, topical abx. O/W optho • Corneal lac: Dx. = fluorescein flow. Tx as for globe rupture. • Scleral lac: Dx and Tx as for globe rupture
Case 17:
Orbital and Intraocular Foreign Body: • May have normal physical exam. Therefore high index of suspicion is crucial. • Low threshold for plain orbital plain films or orbital CT scan if non radioopaque substance • Tx=optho
Case 18: 70 y male 3 days post L cataract surgery. Increased pain and dec. vision.
Endophthalmitis: • Infection involving the deep structures of the eye • Tx=early diagnosis, IV abx (Vanco + 3 rd gen antipseudomonal ceph. +/- clinda), prompt optho referral for intravitreal abx, vitreous tap/vitrectomy, and possible steroids.
Non-traumatic red eye (other than glaucoma)
Conjuncitivitis key points: • Bilateral findings less likely bacterial • Gonococcus only bacterial conjunctivitis with a preauricular node • Always fluorescein eyes to r/o herpes lesions • Never prescribe steroids from ER
Treatments: • Allergic: cool compresses, remove allergens, • • meds Viral (non-herpetic): cool compresses, reassurance, some advocate for prophylactic abx (adenovirus may take 3 weeks to resolve) Bacterial: warm compresses, Na Sulamyd, tobramycin, polymyxin, or erythro (chloramphenical); if o/w healthy avoid topical fluoroquinolones. Culture if non responders. (gonococcus systemic tx, ocular lavage, topical erythro, notification).
Treatment cont. • No evidence comparing one abx to another, but good evidence that abx ameliorate symptoms faster than placebo. (Sheikh & Hurwitz, 2001)
Case 19:
Herpetic keratoconjunctivitis: • Tx. = trifluridine 1% 8 x/day, acyclovir 400 mg 5 x/day (no clinically significant evidence), new topical acyclovir ointment 5 x/day
Case 20:
Herpes Zoster Opthalmica: • PO acyclovir 600 -800 mg 5 x/day or famcyclovir 500 mg po tid. • Start within 72 hrs • +/- po prednisone under guidance of opthamology
Disorders of Lids and Ocular Soft Tissues:
Case 21:
Hordeolum: • Localized, nodular acute infection of an eyelid (staph aureus most common) • Can point to either skin or conjunctival side • Tx=warm compresses 4 -6 x/day, topical abx. I&D if large
Case 22:
Chalazion: • Chronic inflammatory process develops after incomplete resolution of a meibomian gland • Conjunctival or skin side • Non-tender • Tx as for hordeolum (most resolve on own) Sx if still present x 3 -4 wks
Case 23:
Dacrocystitis: • Acute infection of lacrimal sac from Nasolacrimal obstruction • Staph aur. • May express pus from puncta • Tx. Po abx and hot compresses, massage
Case 24:
Preseptal Cellulitis: • Hx URTI, eyelid trauma, external eye infection • Normal vision, no proptosis, normal ocular motility, no pain with eye movements • Staph, strep, heamophilus • PO/IV Abx and optho referral to r/o orbital involvment
Case 25:
Orbital Cellulitis: • Pain, decreased vision, +/- diplopia • Proptosis, limited EOM, Dec visual acuity, +/- afferent pupillary defect • w/u=CT scan, blood/eye c&s • Tx= admit, broad spectrum Abx. Consider mucormycosis
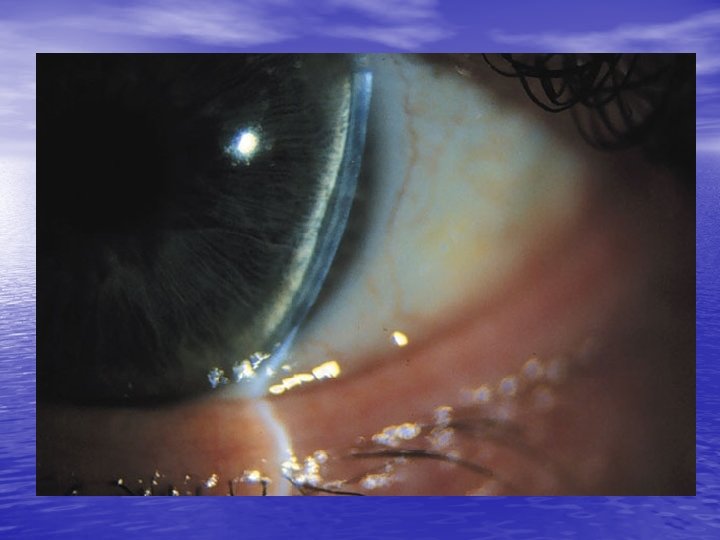
Blepharitis: • Chronic condition • Due to staph infection or seborrheic gland inflammation • Tx=warm compresses, eyelid scrubs (diluted baby shampoo) erythro ointment & chronic eyelid hygeine. PO doxycycline added in severe cases
Case 26:
Phlyctenule: • R/O foreign body • Due to hypersensitivity rxn to antigen such as staph or TB • CXR/mantoux as outpt - refer to optho for ? Topical steroids • Tx coexistant blepharitis
Case 27:
Episcleritis: • “Salmon pink” hue of the superficial layer of the eye between conjunctiva/sclera • Usually idiopathic • 1/3 tender, 2/3 sectoral • Tx. Outpatient referral to optho for topical steroids only if severe.
Case 28:
Scleritis: • More painful, often bilateral • 50 % have systemic dx (Crohns, UC, collagen vasc dx, sarcoid, etc) • Simple vs nodular (immobile nodules with q tip) vs necrotizing • Tx: NSAIDs, Optho referral for steroids and systemic w/u
Case 29:
Iritis: • Redness, photophobia, tearing and decreased vision • Ciliary flush and pupillary constriction • Slit lamp= anterior chamber rxn with WBCs, flare (protein leakage), and keratic precipitates • Always fluorescein to r/o abrasion/herpes • Tx=cycloplegics & Topical NSAIDs and referral to optho for steroids
Dry Eyes:
Summary: • Always do a complete eye exam with documentation of acuity and fluorescein • Never prescribe steroids from ER • Very low threshold to x-ray orbits • When in doubt consult your opthomologist
END