Atrial Fibrillation Key Concepts Dr Dave Dyck R

Atrial Fibrillation: Key Concepts Dr. Dave Dyck R 3 April 10/2003

Today’s Objectives: • Review some of the landmark papers on rate vs rhythm control in detail. • Review the literature on a few questions I had one day on atrial fibrillation: – – Why 48 hours? Use of TEE “Lone” atrial fibrillation Low Molecular Weight Heparin in atrial fibrillation • +++ Discussion/Questions at the end • (Will not discuss antiarrhythmics and no epidemiology, pathophysiology, etc. )

Rate vs Rhythm • Historically goal of treatment has been maintenance of sinus rhythm. • Majority of trials in the literature are on antiarrhythmics looking at conversion/maintenance of sinus rhythm as the primary outcome • Recent literature is providing good evidence that for most cases rate control is equal to, and possibly better than, rhythm control

3 papers to know: • PIAF • Recurrent Persistent Atrial Fibrillation • AFFIRM (landmark paper)

“Hot Café” Study: • Initial randomized attempt to look at rate vs. rhyhm control in non-valvular chronic a fib. • Small prospective Polish study (plan to include 200 pts) • No final results published – Opolski et. al. in Polskie Archiwum Medycyny Wewnetrznej. 101(5): 413 -8, 1999, May
 trial: • Hohnloser S. H, Kuck K. H.")
Pharmacological Intervention in Atrial Fibrillation (PIAF) trial: • Hohnloser S. H, Kuck K. H. , and Lilienthal J. Rhythm or rate control in atrial fibrillation-Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial. Lancet 2000; 356: 1789 -94 • Open randomized trial at 21 German sites • Inclusion criteria: – Symptomatic persistent atrial fibrillation (7 -360 d) – Ages 18 -75

Exclusion Criteria: • • • CHF NYHA class IV Unstable angina or acute MI within 30 d HR<50 bpm Sick sinus syndrome Accessory pathway (WPW) CABG/Valve repair within 3 months Hypertrophic cardiomyopathy Amiodarone tx within 6 months Acute thyroid disease Pacemaker Pregnancy CI to anticoagulants
 = diltiazem 90 mg bid or tid +/-")
Methods: • Group A (Rate control) = diltiazem 90 mg bid or tid +/- additional rate control therapy at discretion of MD • Group B (Rhythm control) = amiodarone 600 mg od x 3 weeks +/- electrical cardioversion + amiodarone 200 mg od • All patients anticoagulated (INR 2 -3)

Primary Endpoints: Change from baseline in the 3 most reported a fib symptoms: - palpitations - dyspnea - dizziness
 Change in")
Secondary Endpoints: • • • Ease of fatiguability (6 min walking tests) Change in mean HR Stabilization of sinus rhythm # hospital admissions Quality of Life questionnaire. (SF-36)

Trial Profile:

Baseline Characteristics:

Intention To Treat Analysis: * • Results:

Secondary Endpoints: * HR change Group A 88 81 Group B 86 78 # in NSR 6 min walk 10% Approx 505 m Hospital admissions 24% 56% Approx 545 m (p=. 008) 69% (p=. 001) Quality of Life NSS (but SS improvement from baseline) Drug Tolerance 14% stopped tx due to SE 25% stopped tx due to SE p=. 036

Summary: • 1 st good randomized trial showing no difference between improvement of symptoms due to a fib in a rate vs rhythm treatment strategy • (BUT – No Mortality End-points)
: • Van Gelder et. Al. A Comparison of")
Recurrent Persistent Atrial Fibrillation Trial (RACE): • Van Gelder et. Al. A Comparison of Rate Control and Rhythm Control in Patients with Recurrent Persistent Atrial Fibrillation. New England Journal of Medicine 347 (23): 1834 -1840. December 5, 2002. • Multicentered Randomized Dutch Trial • N=522 • Inclusion Criteria: – Recurrent persistent A fib or flutter <1 year – 1 or 2 electrical cardioversions within 2 years

Exclusion Criteria: • CHF NYHA class IV • Current/previous amiodarone treatment • pacemaker

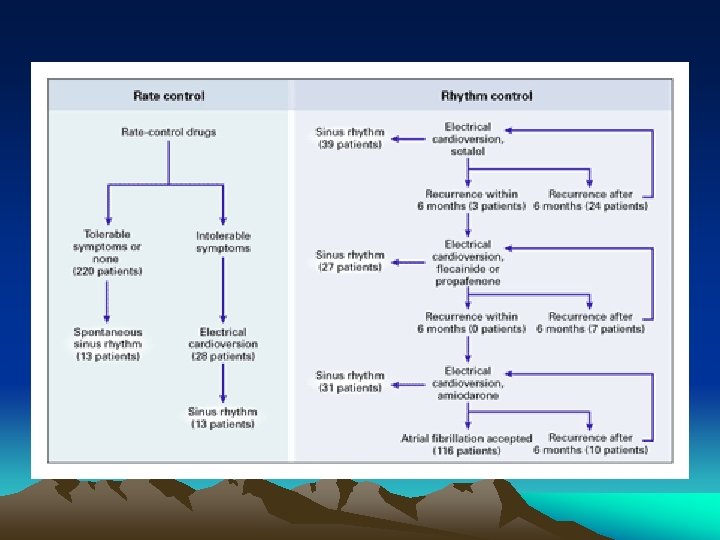
Rate control: • Use of digoxin, Ca channel blocker, and Bblocker alone or in combination • Target HR<100 • Cardioversion or AV node ablation + pacemaker if intolerable symptoms

Rhythm Control • Electrical cardioversion without antiarrhythmic pretreatment then sotalol 160 -320 mg od • If recurrence within 6 months DC cardioversion + flecainide or propafenone if recurrance amiodarone + DC cardioversion • If recurrence after 6 months of any treatment above no changes

Methods Cont. • All anticoagulated 4 weeks prior and post cardioversion (goal INR 2. 5 -3. 5) • If NSR at 1 month ASA or no anticoag. • ASA allowed in rate control group if <65 and no cardiac disease (o/w anticoag. )

Primary End Point* • Composite of death from cardiovascular causes, heart failure, thromboembolic complications, bleeding, pacemaker need, or severe adverse antiarrhythmic drug effects • Over 3 years of maximum follow-up

Baseline characteristics: • Only statistically significant difference was more hypertension in rhythm control group (p. 007)

Outcome: *

Summary: • No advantage to rhythm control vs rate control in recurrent persistent a fib. (trend in favor of rate control which was almost significant) • (esp. HT & women on POST-HOC analysis)* • (note – not applicable to 1 st time a fib pts)

AFFIRM trial: • Wyse DG et al, A Comparison of Rate Control and Rhythm Control in Patients with Atrial Fibrillation (AFFIRM investigators), New England Journal of Medicine, 347 (23), 1825 -1833, December 5, 2002. • Multicentered Randomized North American Trial • N=4060

Inclusion Criteria: • A fib which was likely to be recurrent and cause illness or death • Age >65 or other CVA/death risk factors • Expected long term treatment • Anticoagulation not contraindicated • Eligible to undergo trials of at least 2 drugs in both treatment strategies

Rate Control: • Goal HR < 80 bpm at rest and < 110 bpm during 6 min walk test • Options: beta blockers, Ca channel blockers, digoxin (alone or in combination) • Anticoagulated INR=2. 0 -3. 0

Rhythm Control: • Antiarrhythmic chosen by treating physician (amiodarone, disopyramide, dofetilide, flecainide, moricizine, procainamide, propafenone, quinidine, sotalol, and combinations allowed) • Anticoagulation encouraged but could be dc’d if NSR at 4, or preferably, 12 weeks if the physician chose to

Other considerations: • If 2 trials of either a rate or rhythm control drug failed, then non-pharmacologic therapies could be considered (ablation, maze procedure, pacing etc)

Primary End Point: • Overall mortality

Secondary End Points: • Composite of death, disabling stroke, disabling anoxic encephalopathy, major bleeding, and cardiac arrest. • Mean follow-up time of 3. 5 years

Of Note: * • More than 1/3 were enrolled after having had a first episode of a fib* • More than 2/3 had duration > 2 days • No significant differences in baseline characteristics • Only 12% had no associated cardiac disease (may not apply well to lone a fib) • 7401 patients were eligible and offered enrollment, but only 4060 were enrolled**

Drugs Used: *

Rate control f/u: • At 5 year visit: 34. 6% in NSR, and over 80% in a fib had adequate HR control. 5% had radiofrequency ablation. • 248/2027 crossed over to rhythm control at some point with 86 of these returning to rate control by the end of the study. (uncontrolled a fib/CHF were most common reasons)

Rhythm Control f/u: • At 5 year visit: 62. 6% in NSR. Electrical cardioversion attempted x 1 (18%), x 2 (11%), x 3 or more (9%) • 594/2033 crossed over to rate control at some point with 61 returning to rhythm control by the end (inability to maintain NSR and drug intolerance)

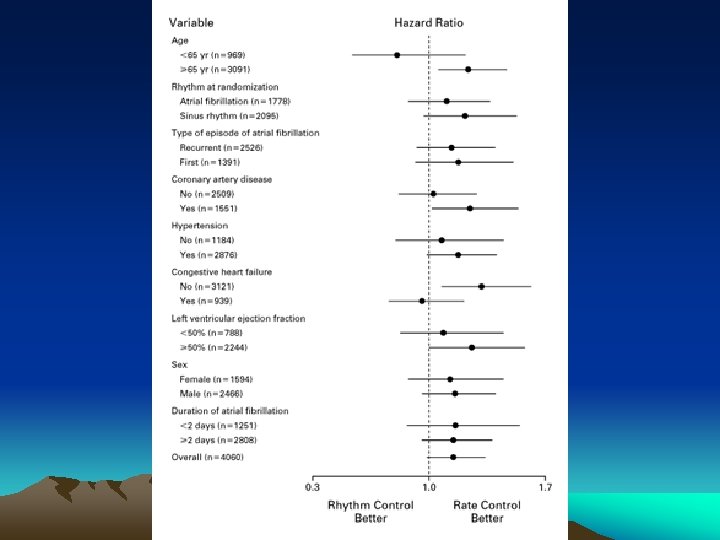
Results: * • Intention to treat analysis
 vs rhythm control (23. 8%) and")
No significant difference between rate control (21. 3%) vs rhythm control (23. 8%) and a trend towards benefit of rate control p=. 08*

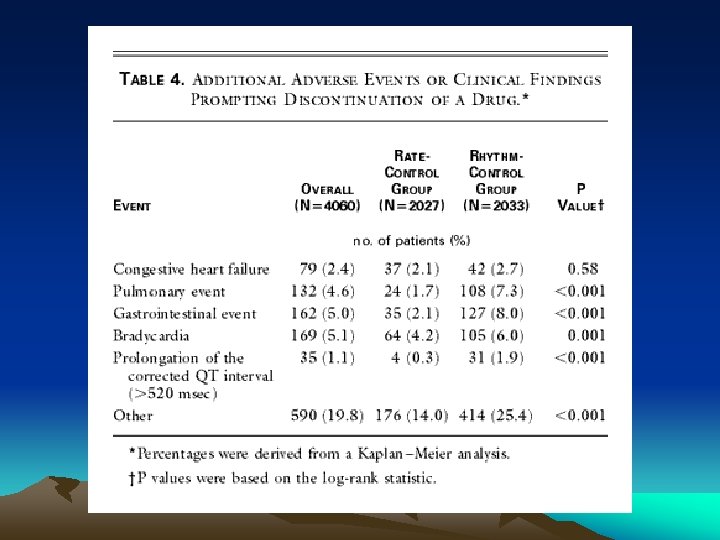
Secondary End Points: *

Summary: • LANDMARK PAPER! • There is no benefit to rhythm control over rate control in patients > 65 or with other stroke risk factors who have persistent/recurrent atrial fibrillation. In these patients there is even a trend towards benefit of rate control. • This is also one of the first trials to show that in first presentation a fib, if selected as likely to be recurrent/persistent and mandate treatment, then there is also a trend to benefit of rate control. • Does not apply to lone a fib; especially in the younger population*

Question 2: Why 48 hrs?

Risks of Thromboembolism with Cardioversion: Why 48 hrs? • Weigner et. Al. Risk for clinical thromboembolism associated with conversion to sinus rhythm in patients with atrial fibrillation lasting less than 48 hours. Annals of Internal Medicine Vol 126 (8); April 15, 1997. • Prospective chart review of admitted patients with atrial fibrillation clinically estimated to be < 48 hrs in duration. • Outcome= thromboembolic events during hospitalization or within 30 days of conversion • (excluded those who were therapeutically anticoagulated on presentation)
* • 357 (95. 2%)")
Results: • 375 patients (mean age 68 +/- 16 yrs)* • 357 (95. 2%) patients converted to NSR (250 spontaneously and 107 actively converted) • 228 (61%) patients were anticoagulated or given ASA upon admission (IV heparin= 133; 35. 5%, coumadin= 26; 6. 9%, ASA= 69; 18. 4%) • 3 patients (0. 8%) (95% CI=. 2 -2. 4%) had clinical thromboembolic events (This is the same rate as for patients >48 hrs treated with the conventional coumadin for 4 weeks pre/post conversion)**
 with 24 hrs")
Affected patients: • 1. 86 y female w HTN (on ASA) with 24 hrs a fib converted spontaneously to NSR with rate control and had a L parietal embolic stroke <12 hrs later (pt was not anticoagulated) • 2. 83 y female w CAD and a fib < 24 hrs on presentation converted with rate control after 2 days and heparin was DC’d. The next day she had a brachial artery embolus. • 3. 89 y female w HTN and a fib < 24 hrs converted to NSR with rate control the next day (<48 hrs). 12 hrs post conversion the patient became aphasic which then resolved within hours. (pt was not anticoagulated until after her TIA) • (2 of these patients did not have anticoagulants started)*

Summary: • This study provides fairly good evidence that the risk of thromboembolism after cardioversion of AF<48 hrs is low. • (This study also recommended that IV heparin be initiated on admission for all patients with AF < 48 hours, and continued for at least 24 hours post cardioversion. )

More Evidence: • Gallagher MM et al. Embolic complications of direct current cardioversion of atrial arrhythmias: Association with low intensity of anticoagulation at the time of cardioversion. Journal of the American College of Cardiology. 40(5): 926 -33, 2002 Sep 4. • DC cardioversion performed within 2 days of onset of AF/flutter in 443 episodes (352 pts not on prolonged anticoagulation) • 1 embolic event

More evidence: • Mitchell et. al. , Cardioversion related stroke rates in atrial fibrillation and atrial flutter, Circulation, 1997; 96: I-453. • Reviewed the Ibutilide database to review the cardioversion related (<7 d) stroke rate in patients who were cardioverted at <48 hrs and not given prolonged anticoagulation • In 688 patients 1 stroke occurred. **

Summary: • Reasonable evidence that there is a very low risk of thromboembolism if cardioversion occurs in atrial fibrillation < 48 hrs duration. *

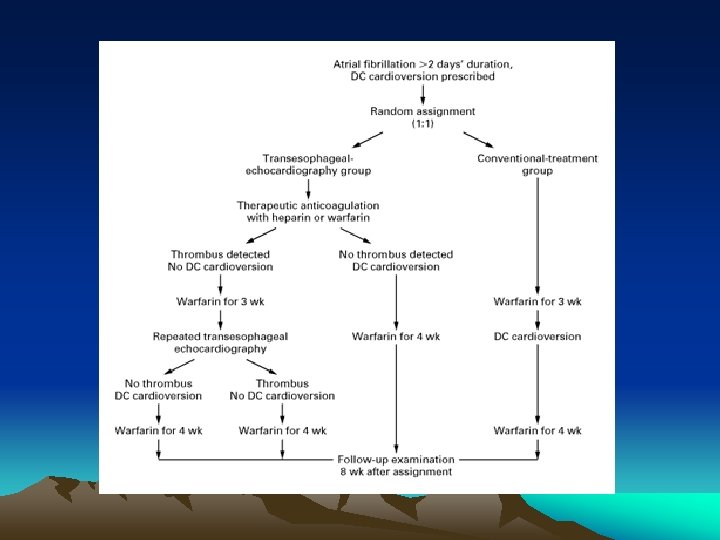
TEE and a fib • Klein et al. Use of Transesophageal Echocardiography to Guide Cardioversion in Patients with Atrial Fibrillation, New England Journal of Medicine. Vol 344 (19) 1411 -1420, May 10, 2001. (ACUTE trial) • Multicentered randomized prospective trial comparing standard tx (3 wks anticoagulation/cardioversion/4 wks anticoagulation) vs TEE guided cardioversion in a fib/flutter > 48 hrs. 1222 pts. • Primary outcome = composite of CVA, TIA, and peripheral embolism at 8 wks

ACUTE trial cont. • Patients assigned to TEE were divided into two groups • -inpatients: given heparin and scheduled TEE + cardioversion within 24 hrs. -outpatients: warfarin and scheduled TEE + cardioversion in 5 days

ACUTE trial cont. • Estimated sample size was 3000 patients based on an estimated rates of embolism of 1. 2% in TEE grp and 2. 9% in conventional grp. • First interim analysis after 1000 pts led to termination of the study

Results: • 5/619 in TEE group had an embolic event • 3/603 in conventional group had an event • No significant difference in primary outcome between the two groups (p=. 50) • Also, at 8 weeks there were no significant differences between the two groups in the rates of death or maintenance of sinus rhythm or in functional status.
 in TEE group had")
ACUTE trial cont. • Of note, 76/619 pts (13. 8%) in TEE group had a thrombus noted. 67/76 (88. 2%) were in the left atrial appendage. • Of note, there was a trend toward a higher rate of death from all causes in the TEE group (15 vs 6; p=0. 06)

What if TEE is used after 3 weeks of anticoagulation? * • Seidl et al. Embolic Events in Patients with Atrial Fibrillation and Effective Anticoagulation: Value of Transesophageal Echocardiography to Guide Direct-Current Cardioversion. Journal of the American College of Cardiology. V 39 (9), May 1, 2002. • No difference in outcome at the 4 week follow-up period

TEE Summary: • A TEE guided strategy for elective cardioversion in patients with AF > 48 hours has comparable outcomes for thromboembolism and death when compared with current traditional treatments. • Thus, it is an “alternative” Class I recommendation in the ACA/AHA/ESC guidelines to traditional treatments. • Consider this approach if the patient is at high risk of LA thrombus (rheumatic valve disease, recent thromboembolism, severe LV dysfunction) or if they cannot tolerate prolonged anticoagulation

What about “Lone” Atrial Fibrillation?

“Lone” Atrial Fibrillation? – Best Evidence* • Kopecky et al. The Natural History of Lone Atrial Fibrillation. A Population Based Study Over Three Decades. New England Journal of Medicine. 317(11): 669 -74, Sept 10, 1987. • 3623 pts with AF from Minnesota. 97 (2. 7%) were < 60 y and had lone AF. • 20 = 1 isolated episode, 56 = recurrent AF, 21 = chronic AF • F/U varied (mean = 15 years) • 4 pts had CVAs ie. Very low risk (. 28%/yr) *

Lone AF • Framingham study had 43/5209 participants given the diagnosis of lone AF with an age adjusted stroke rate over 11 yrs of 28. 2% compared with 6. 8% in matched controls. • BUT = lone AF included hypertensives, diabetics and patients with cardiomegally on CXR and they did not use echocardiography • THUS = these patients really were not “lone” AF

Lone AF cont. • Scardi et al. Lone Atrial Fibrillation: Prognostic Differences Between Paroxysmal and Chronic Forms After 10 years of Follow-up. American Heart Journal. 137(4 pt 1): 686 -91, April 1999. • N=145 age < 50 (paroxysmal = 96, chronic = 49) followed for 10 yrs with recording of thromboembolic phenomenon) • Results – Paroxysmal AF 1 embolic phen. (1%), 2 TIAs – Chronic AF 7 embolic phen. (16. 3%), 1 TIA • Conclusion: patients < 50 with paroxysmal lone AF have an excellent prognosis while those with chronic lone AF may be at increased risk of thromboembolic events

Lone AF > 60 y • Kopecky et al. Lone Atrial Fibrillation in Elderly Persons – A Marker For Cardiovascular Risk. Archives of Internal Medicine. V 159, May 24, 1999. • Patients > 60 y with lone AF compared with matched controls. Mean f/u=9. 6 y • Lone AF had a total CV event rate of 5. 0% person-year. Matched controls had 1. 3% rate • Although small numbers (n=55), this study forms the basis for antithrombotics in AF patients >60.

Lone AF Summary: • Still controversial but – Appears to be fairly benign in patients < 60 with paroxysmal lone AF (definitely if <50). – Increased risk of thromboembolic disease if chronic AF – Increased risk of thromboembolic disease if > 60 y

What about LMWH in Atrial Fibrillation?

LMWH in atrial fibrillation: • Current ACC/AHA/ESC guidelines give little mention of LMWH usage • State it is a Class IIb recommendation in specific circumstances (eg in high risk patients who must be off po anticoagulants for a whatever reason) and an optional Class I recommendation in AF patient’s undergoing cardioversion (level C evidence = expert consensus) • Based largely on extrapolation of venous thromboembolic disease states

LMWH in AF • The sixth ACCP Consensus Conference on Antithrombotic Therapy, Antithrombotic Therapy in Atrial Fibrillation, Chest, 2001; 119: 194 S-206 S – No mention of LMWH!

LMWH and AF • Harenberg et al. Prophylaxis of Embolic Events in Patients with Atrial Fibrillation Using Low Molecular Weight Heparin. Seminars in Thrombosis & Hemostasis. 19 Suppl 1: 116 -21, 1993. – Compared LMWH CY 216 with no specific treatment (observation only) in 75 consecutive patients with chronic non-rheumatic AF* – In LMWH 3/35 had thromboembolism while 8/40 controls had thromboembolism. ** – Still poor evidence

LMWH and AF • Very little in the literature • Kim et al. A Prospective, randomized, controlled Trial of an Emergency Department. Based Atrial Fibrillation Treatment Strategy With Low-Molecular-Weight Heparin, Annals of Emergency Medicine, 40(2), August 2002, p 187 -192 – A pilot study that compared traditional approaches involving hospitalization to an ED based LMWH approach in the treatment of newly diagnosed/recent AF. – Showed much lower hospitalization stays and costs (1 d vs. 2 d; $879 vs. $1706) in the LMWH group although no conclusions made because of small numbers. (n=18)

LMWH and AF • Labeque et al. Treatment of left atrial thrombosis by lowmolecular-weight heparin. A preliminary study of 6 cases. Archives des Maladies du Coeur et des Vaisseaux. 93(12): 152833, 2000 Dec. • 6 patients with atrial thrombi on TEE were treated with enoxaparin x 3 weeks. • 5/6 had resolution of thrombi at 3 wks on rpt TEE

LMWH and AF • Murray et al. Potential clinical efficacy and cost benefit of a transesophageal echocardiography-guided low molecular-weight heparin (enoxaparin) approach to antithrombotic therapy in patients undergoing immediate cardioversion from atrial fibrillation. Journal of the American Society of Echocardiography. 14(3): 200 -8, 2001 Mar. • Showed that there are substantial monetary savings when LMWH is used instead of IV heparin as a bridge post TEE guided cardioversion to therapeutic anticoagulation with heparin ($1353 less)
 that")
LMWH and AF • So far there are no trials (good or bad) that have looked directly at outcomes comparing LMWH with standard antithrombotic treatments in atrial fibrillation

LMWH in AF • Thankfully there is the ACE study underway. (Anticoagulation in Cardioversion using Enoxaparin) • Randomized, prospective, open label multicentre trial • Stellbrink et al. Anticoagulation in Cardioversion using Enoxaparin Study Group. Low Molecular Weight Heparin for Prevention of Thromboembolic Complications in Cardioversion –Rationale and Design of the ACE study, Zeitschrift fur Kardiologie. 91(3): 249 -54, Mar. 2002.

What about antithrombotic therapy?

HUGE TOPIC! • Awesome resource is the summary overview “Antithrombotic Therapy in Atrial Fibrillation” by the Sixth ACCP Consensus Conference on Antithrombotic Therapy published in Chest V 119(1) Supp, Jan 2001.
 that in many")
Summary #1: • There is good new evidence (AFFIRM, RACE, PIAF) that in many AF patients rate control with anticoagulation is just as good (if not better than) as rhythm control. • However, this evidence should be used in a “patient by patient basis” and likely does not apply to “lone” AF patients, 1 st time AF presenters, or those with symptomatic paroxysms.

Summary #2: • There is reasonable evidence that cardioversion for AF<48 hrs is safe (note: should use periconversion anticoagulation) • There is good evidence that a TEE guided approach to AF pts>48 hrs provides equal, but not superior outcomes to the traditional approach of 3 -4 wks pre-cardioversion anticoagulation. (ACUTE trial)

Summary #3 • “Lone” AF has a very low risk of stroke especially if it is of the paroxysmal type and age < 60. • There is a huge need for ED based research involving LMWH in AF. (the ACE trial should help)

CASE: • 66 y male retired GP presents with mild palpitations. ECG shows AF with a rate of 106. • Patient sure of the onset (9 hours ago) • PMHx: HTN, had similar sensation 2 years ago/4 mo ago but resolved after 2 -4 hours. • HR decreases to 76 with diltiazem and patient becomes asymptomatic but is still in AF • What would you do?

QUESTIONS?
- Slides: 80