Hodgkins Disease and NonHodgkins Lymphoma Harold M Chung














 n n systemic symptoms")








 80 -90% RC n n")


 (Valagussa ’")




 # pts")




 Overall Survival")
 Total Patients = 547 (1. 5")
 Total Patients 204")



 A Younes et al, N Engl J Med 2010; 363: 1812")




 Diffuse Indolent Aggressive Small cell Large cell")

")




 Nodular lymphocyte Predominant (NLPHL) Multiple Myeloma")

 Peripheral T-cell (6%) Indolent (35%)")



 Bcl 2 Chromosome 18 C Chromosome")



 n n n Low-grade/Indolent lymphoma Radiation therapy sensitive")




 n CR")









J S E C Ig. H Chromosome")




 n n Triple-Hit")











- Slides: 99
Hodgkin’s Disease and Non-Hodgkin’s Lymphoma Harold M. Chung, MD Associate Professor of Medicine VCU Medical Center – MCV Hospitals Bone Marrow Transplantation Program November 8, 2011
Why Men Can’t Be Babysitters
Agenda n Discuss Hodgkin’s Disease n Discuss Non-Hodgkin’s Lymphoma n Classification Systems n Treatment Options
2008 Estimated US Cancer Cases* Men 720, 280 Women 679, 510 Prostate 33% 31% Breast Lung & bronchus 13% 12% Lung & bronchus Colon & rectum 10% 11% Colon & rectum Urinary bladder 6% 6% Uterine corpus Melanoma of skin 5% 4% Non-Hodgkin lymphoma 4% Melanoma of skin Kidney 3% 3% Thyroid Oral cavity 3% 3% Ovary Leukemia 3% 2% Urinary bladder Pancreas 2% 2% Pancreas All Other Sites 18% 22% All Other Sites *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2008.
2008 Estimated US Cancer Deaths* Men 291, 270 Women 273, 560 Lung & bronchus 31% 26% Lung & bronchus Colon & rectum 10% 15% Breast 10% Colon & rectum Prostate 9% Pancreas 6% 6% Pancreas Leukemia 4% 6% Ovary Liver & intrahepatic 4% bile duct 4% Leukemia 3% Non-Hodgkin lymphoma 3% Uterine corpus 2% Multiple myeloma Brain/ONS Esophagus 4% Non-Hodgkin lymphoma 3% Urinary bladder 3% 2% Kidney 3% 23% All other sites 23% ONS=Other nervous system. Source: American Cancer Society, 2008. All other sites
WHO/REAL Classification of Lymphoid Neoplasms B-Cell Neoplasms Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma (precursor B-acute lymphoblastic leukemia) Mature (peripheral) B-neoplasms B-cell chronic lymphocytic leukemia / small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma‡ Splenic marginal zone B-cell lymphoma (+ villous lymphocytes)* Hairy cell leukemia Plasma cell myeloma/plasmacytoma Extranodal marginal zone B-cell lymphoma of MALT type Nodal marginal zone B-cell lymphoma (+ monocytoid B cells)* Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Mediastinal large B-cell lymphoma Primary effusion lymphoma† Burkitt’s lymphoma/Burkitt cell leukemia§ T and NK-Cell Neoplasms Precursor T-cell neoplasm Precursor T-lymphoblastic leukemia/lymphoma (precursor T-acute lymphoblastic leukemia Mature (peripheral) T neoplasms T-cell chronic lymphocytic leukemia / small lymphocytic lymphoma T-cell prolymphocytic leukemia T-cell granular lymphocytic leukemia. II Aggressive NK leukemia Adult T-cell lymphoma/leukemia (HTLV-1+) Extranodal NK/T-cell lymphoma, nasal type# Enteropathy-like T-cell lymphoma** Hepatosplenic γδ T-cell lymphoma* Subcutaneous panniculitis-like T-cell lymphoma* Mycosis fungoides/Sézary syndrome Anaplastic large cell lymphoma, T/null cell, primary cutaneous type Peripheral T-cell lymphoma, not otherwise characterized Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma, T/null cell, primary systemic type Hodgkin’s Lymphoma (Hodgkin’s Disease) Nodular lymphocyte predominance Hodgkin’s lymphoma Classic Hodgkin’s lymphoma Nodular sclerosis Hodgkin’s lymphoma (grades 1 and 2) Lymphocyte-rich classic Hodgkin’s lymphoma Mixed cellularity Hodgkin’s lymphoma Lymphocyte depletion Hodgkin’s lymphoma ‡ Formerly known as lymphoplasmacytoid lymphoma or immunocytoma II Entities formally grouped under the heading large granular † Not described in REAL classification lymphocyte § Includes the so-called Burkitt-like lymphomas leukemia of T- and NK-cell types * Provisional entities in the REAL classification ** Formerly known as intestinal T-cell lymphoma # Formerly know as angiocentric lymphoma
Hematopoietic System
B cell malignancies Lymph node, lymph, blood, bone marrow Bone marrow Progressive B lymphocyte maturation Lymphoid stem cell Pre-B acute lymphoblastic leukemia Maturing B cell many stages B cell lymphoma Mature B cell Chronic lymphocytic leukemia Plasma cell Multiple myeloma
Boys Need Parents
Hodgkin’s Disease/Lymphoma In the Beginning First described in 1832 by Dr. Thomas Hodgkin Neoplasm of B lymphocytes – large pleomorphic prominent nucleolus in a halo - Hodgkin cells Reed-Sternberg cell – binucleate Hodgkin cell with owl eye appearance Classification: Classical Hodgkin’s Nodular sclerosis – low grade Mixed cellularity Lymphocyte rich classical Lymphocyte depleted. – high grade Nodular lymphocyte-rich Hodgkin’s 1798 -1866
Hodgkin’s Disease/Lymphoma In the Beginning n Bimodal age distribution n n first peak between 2 nd - 3 rd decade of life second peak between 5 th - 6 th decade of life n Male: Female 2: 1 in kids, adults almost equal M: F n Mixed cellularity (MC) Hodgkin’s Disease is more common at younger ages n More common in immune deficiency patients
Hodgkin’s Disease/Lymphoma In the Beginning n Accounts for ~ 30% of all malignant lymphomas n Composed of two different disease entities: Lymphocyte-predominant Hodgkin’s (LPHD), making up ~ 5% of cases Classical HD, representing ~ 95% of all HDs. A common factor of both HD types is that neoplastic cells constitute only a small minority of the cells in the affected tissue, often corresponding to < 2% of the total tumor
Hodgkin’s Disease/Lymphoma In the Beginning Fatal disease with 90% of untreated patients dying within 2 to 3 years With chemotherapy, >80% of patients suffering from HD are cured. Pathogenesis of HD is still largely unknown. HD nearly always arises and disseminates in lymph nodes
Hodgkin’s Disease/Lymphoma Interest tidbits n Pel-Ebstein Fevers n Pain with alcohol consumption
Hodgkin’s Disease/Lymphoma Clinical Presentation n Nontender lymph nodes enlargement (localized) n n systemic symptoms (B symptoms) n n neck and supraclavicular area mediastinal adenopathy other (abdominal, extranodal disease) fever night sweats unexplained weight loss (10% per 6 months) other symptoms n n fatigue, weakness, pruritus cough , chest pain, shortness of breath, vena cava syndrome abdominal pain, bowel disturbances, ascites bone pain
Hodgkin’s Disease/Lymphoma Clinical Presentation SIGNS & SYMPTOMS % OF PATIENTS Lymphadenopathy 90 Mediastinal mass 60 “B” symptoms 30 Fever, weight loss, night sweats Hepatosplenomegaly 25 n n Most commonly involved lymph nodes are the cervical and supraclavicular in 75% Bone marrow is involved in 5% of patients
Reed-Sternberg Cells
CD 30 Immunostain
Hodgkin’s Disease/Lymphoma Clinical Presentation Stage Definition I Involvement of a single lymph node region (I) or of a single extralymphatic organ or site (IE) II Involvement of two or more lymph node regions on the same side of the diaphragm (II) or localized involvement of an extralymphatic organ or site and one or more lymph node regions on the same side of the diaphragm (IIE) III IV be Involvement of lymph node regions on both sides of the diaphragm (III) which may accompanied by involvement of the spleen (IIIS) or by localized involvement of an extralymphatic organ or site (IIIE) or both (IIISE) Diffuse or disseminated involvement of one or more extra lymphatic organs or tissues with or without associated lymph node involvement B symptoms: fever > 38ºC for three consecutive days, drenching night sweats or unexplained loss 10% or more of weight the preceding 6 months
Hodgkin’s Disease/Lymphoma Treatment n Unfavorable prognostic factors: - Stage IIIB, IV - B symptoms - Bulky disease - High ESR >50
Hodgkin’s Disease/Lymphoma Treatment n Long term effects of treatment should be taken into consideration: - Treatment-related second neoplasms (i. e. AML, NHL and breast cancer) - Infertility - Growth consideration - Long-term organ dysfunction (i. e. , thyroid, heart, lung)
Hodgkin’s Disease/Lymphoma Treatment n Adolescent patients who have achieved maximum growth can be treated as adult patients n Chemotherapy alone protocols for localized disease has been used in developing countries with some success Lobo-Sanahuja F: Medical and Pediatric Oncology 22(6); 1994
Hodgkin’s Disease/Lymphoma Treatment With appropriate treatment about 85% of patients with Hodgkin’s disease are curable n I A, B II A n IIB; IIIA, B; IVA, B n Radiation Therapy Combination Chemo + Radiotherapy Combination Chemo (+/- radiotherapy)
Hodgkin’s Disease/Lymphoma Treatment n Radiation therapy (35 -40 Gy) 80 -90% RC n n Mantle field Paraaortic field Pelvic field Combination chemotherapy n n ABVD BEACOPP 80% RC 90% RC
Hodgkin’s Disease/Lymphoma Treatment Progress
ABVD vs MOPP/ABVD Failure-free survival Canellos et al, NEJM, 2002 Overall survival
Hodgkin’s Disease/Lymphoma Treatment n Almost no MDS/AML (at 15 years 1. 0%) (Valagussa ’ 86) n Oligospermia – 50% complete recovery n Median FSH in normal range (Viviani ’ 85) n Bleomycin-related pulmonary toxicity ~1/3 have reduced PFT but recover in 3 months; ~20% omit Bleomycin.
Cancer and Leukemia Group B 8251 and 8952: Recurrent Hodgkin's Disease by Treatment Canellos, G. P. et al. J Clin Oncol; 22: 1532 -1533 2004
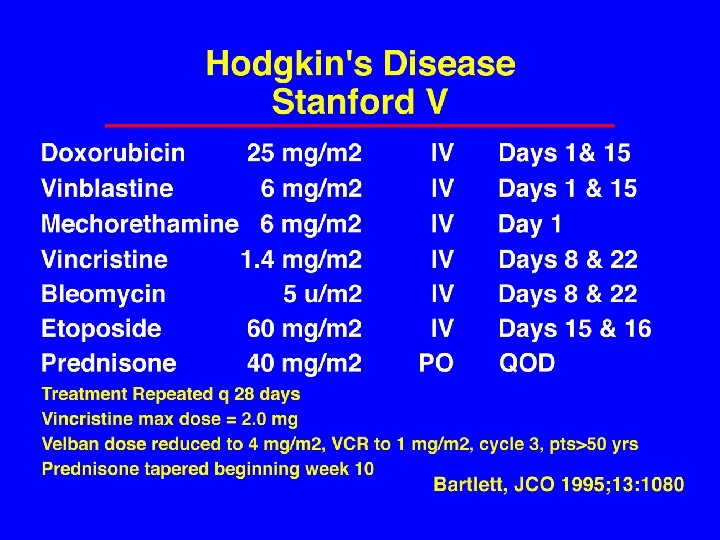
Hodgkin’s Disease/Lymphoma – Advanced Stage ABVD vs MEC vs Stanford V
Hodgkin’s Disease/Lymphoma Actual Treatment Progress Stanford, Hoppe et al
Causes of Death among 2733 Patients with Hodgkin’s Disease/Lymphoma Hodgkin lymphoma 383 41. 2% Secondary cancers 200 21. 5% Cardiovascular 148 15. 9% Pulmonary 41 4. 4% Infection 35 3. 8% Trauma/Suicide 16 1. 7% MDS 11 1. 2% Other/Unknown 96 10. 3% 930 100. 0% Total Stanford, Hoppe et al
SECOND TUMORS LONG-TERM SURVIVORS OF HODGKIN’S DISEASE/LYMPHOMA (PRIMARY RT OR COMBINED MODALITY) # pts Actuarial Incidence Median Follow-up n Princess Margaret Hospital, Toronto 865 18% (20 years) 20 years n US Pediatric Series (JCO 21: 4386, 2003) 1380 26. 3% (30 years) 17 years n Harvard/Joint Center (Blood 100: 1989, 2002) 1319 35% (25 years) 12 years n Netherlands (JCO 18: 481, 2000) 1253 27. 7% (25 years) 14. 1 years n NIH Survey of Registries and Seer (JCO 20: 3474, 2002) 32, 591 21. 9% (25 years) 10 years
HODGKIN’S DISEASE/LYMPHOMA SALVAGE REGIMENS Regimen DHAP Patients 102 CR/PR to ASCT 87% 60% (dexamethasone, ara-C, cisplatin) Mini-BEAM 89 77% 82% 75% 62% 88% 84% 86% 64% -- (BCNU, etoposide, ara-C, melphalan; 2 series) Dexa-BEAM 225 (above plus dexamethasone; 3 series) GDP 34 (gemcitabine, dexamethasone, oxaloplatin) ICE 65 (ifosfamide, carboplatin, etoposide) GND 38 (gemcitabine, vinorelbine, liposomal doxorubicin)
CALGB 50203 Treatment Plan AVG: n Doxorubicin 25 mg/m 2 IV d 1, D 15 n Vinblastine 6 mg/m 2 IV d 1, d 15 n Gemcitabine 1, 000 mg/m 2 IV d 1, d 15 n 800 mg/m 2 if gr. 4 ANC/plt ct in 2. 6 pts Repeat every 28 days x 6 cycles
HODGKIN’S DISEASE/LYMPHOMA Autologous Transplants as Primary Therapy n 1996 - 2002: 7 uncontrolled trials Event-free survival 242/337 patients 72% Median follow-up 42 -46 months (30 -86 months) n 2003: Prospective Randomized Trial (JCO 21: 2320, 2003) 163 83 ASCT CR 89% RFS (5 years) 88% OS (5 years) 88% 80 (4 more cycles ABVD) 92% 94% 88% [no difference]
PROBABILITY OF SURVIVAL AFTER AUTOTRANSPLANTS FOR RELAPSED HODGKIN’S DISEASE/LYMPHOMA, 1996 -2001 100 CR 1 (N = 226) PROBABILITY, % 80 CR 2+ (N = 733) 60 Never in remission (N = 823) 40 Relapse (N = 1, 744) 20 P = 0. 0001 0 0 1 2 3 YEARS 4 5 6
ALLOTRANSPLANTATION HODGKIN’S DISEASE/LYMPHOMA Patients Median age Event-free Survival Median F/U (mos. ) Overall Survival Treatment Mortality GVH Acute Chronic EBMTR 45 29 IBMTR 100 28 JOHNS HOPKINS 53 28 15% 31 25% 48% 15% 36 21% 61% 26% 60 30% 43% 63% 55% 35% 45% 17%
HODGKIN’S DISEASE/LYMPHOMA Non-Myeloablative Allotransplants 7 series (2004 -2008) Total Patients = 547 (1. 5 – 5 -year follow-up) Relapse PFS OS Treatment-Related Mortality 43 -64% 18 -32% 28 -61% 5 -24% (The majority failed autotransplantation)
HODGKIN’S DISEASE/LYMPHOMA Residual Masses By PET scan 5 series (2001 -present) Total Patients 204 Relapses PET negative after therapy 144 18 (12. 5%) PET positive (58. 3%) after therapy 60 ? 40% false positive rate 35
CTN 0701 n Tandem Transplant Modeled after myeloma data n High-risk Hodgkin’s Disease n University of Nebraska – Julie Vose, MD n
Monoclonal Antibodies
MDX-060 - Anti-CD 30 target Anti-CD 30 antibody Medarex 2004 – Orphan Drug Status Hodgkin’s Disease/Lymphoma Anaplastic Large Cell NHL
SGN-35 (Seattle Genetics) A Younes et al, N Engl J Med 2010; 363: 1812 -21.
Good Ideas n Cadence Pharmaceuticals Ofirmev n November 2, 2010 – FDA Approval n IV acetaminophen n $800/IV dose n
Boys Need Parents
Non-Hodgkin’s Lymphoma Deep Breath… Stand up… Stretch…
Histologic Classification of Non-Hodgkin’s Lymphomas 1. Rappaport 2. Lukes and Collins 3. Kiel 3. Dorfman 4. Bennet et al. , 5. Lennert 6. WHO 7. Working Formulation 8. REAL 9. WHO - 1966 1974 1974 1976 1982 1994 1999
Non-Hodgkin’s Lymphoma Rappaport Classification Nodular (follicular) Diffuse Indolent Aggressive Small cell Large cell
Non-Hodgkin’s Lymphoma Rappaport Classification n n Small cell, follicular Small cell, diffuse Large cell, follicular Large cell, diffuse
Non-Hodgkin’s Lymphoma Immunophenotyping n Immunohistochemistry Immunofluorescence Flow cytometry n Identification of CD’s (cluster determinants) n n CD 5 = T cell type n CD 20 = B cell type n
Non-Hodgkin’s Lymphoma Cluster Determinants
Non-Hodgkin’s Lymphoma Lukes-Collins & Kiel Classifications n Lukes-Collins System – US Kiel System – Europe n Differentiation of B-cell and T-cell lymphomas n
Non-Hodgkin’s Lymphoma Working Classification n n n Developed in 1980’s NCI Investigators reviewed Rappaport, Lukes. Collins, and Kiel systems n=1175 Goal was to clarify… now a new system! No consideration to B-cell or T-cell typing Goal was to group lymphomas according to aggressiveness (low, intermediate, high)
Non-Hodgkin’s Lymphoma Working Classification n Low Grade n n Intermediate Grade n n n Small Lymphocytic Follicular small-cleaved cell Follicular mixed small-cleaved and large cell Follicular large cell Diffuse small cleaved cell Diffuse mixed small and large cell Diffuse large cell High Grade n n n Large cell immunoblastic Lymphoblastic Small non-cleaved cell (Burkitt's and non-Burkitt's type)
Hodgkin Lymphoma Classical HL (NS, MC, LR, LD) Nodular lymphocyte Predominant (NLPHL) Multiple Myeloma Non Hodgkin Lymphoma Indolent Aggressive Highly Aggressive B cell Follicular SLL/CLL Marginal zone LP (WM) B cell DLBCL FLg 3 and t. FL Mantle cell Primary effusion B cell Pre-B lymphoblastic Burkitt T/NK cell Mycosis fungoides Sezary syndrome Primary cut ALCL T/NK cell ALCL Angioimmunoblastic Subq panniculitis-like Blastic NK Extnanodal NK/T nasal Enteropathy-type Hepatosplenic PTCL nos T/NK cell Pre-T lymphoblastic
Non-Hodgkin’s Lymphoma REAL Classification n n Revised European-American Lymphoma Mid 1990’s – International Lymphoma Study Group (informal group of hematopathologists) Using immunophenotype, cytogenetics, molecular diagnostics Reclassified lymphomas by diagnostic criteria and not by risk categories
Frequency of NHL Subtypes in Adults Mantle cell (6%) Peripheral T-cell (6%) Indolent (35%) Other subtypes with a frequency 2% (9%) Composite lymphomas (13%) Armitage et al. J Clin Oncol. 1998; 16: 2780– 2795 Diffuse large B-cell (31%)
Non-Hodgkin’s Lymphoma WHO Classification n n Bruce Cheson, MD and the NCI International Working Group reported in January 1999 Adopted in 2001, Revised in 2008 Discredited the Working (non-REAL) Classification Based on REAL (Non-working) Classification Cheson et al. J Clin Oncol. 1999 Apr; 17(4): 1244
WHO/REAL Classification of Lymphoid Neoplasms B-Cell Neoplasms Precursor B-cell neoplasm Precursor B-lymphoblastic leukemia/lymphoma (precursor B-acute lymphoblastic leukemia) Mature (peripheral) B-neoplasms B-cell chronic lymphocytic leukemia / small lymphocytic lymphoma B-cell prolymphocytic leukemia Lymphoplasmacytic lymphoma‡ Splenic marginal zone B-cell lymphoma (+ villous lymphocytes)* Hairy cell leukemia Plasma cell myeloma/plasmacytoma Extranodal marginal zone B-cell lymphoma of MALT type Nodal marginal zone B-cell lymphoma (+ monocytoid B cells)* Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Mediastinal large B-cell lymphoma Primary effusion lymphoma† Burkitt’s lymphoma/Burkitt cell leukemia§ T and NK-Cell Neoplasms Precursor T-cell neoplasm Precursor T-lymphoblastic leukemia/lymphoma (precursor T-acute lymphoblastic leukemia Mature (peripheral) T neoplasms T-cell chronic lymphocytic leukemia / small lymphocytic lymphoma T-cell prolymphocytic leukemia T-cell granular lymphocytic leukemia. II Aggressive NK leukemia Adult T-cell lymphoma/leukemia (HTLV-1+) Extranodal NK/T-cell lymphoma, nasal type# Enteropathy-like T-cell lymphoma** Hepatosplenic γδ T-cell lymphoma* Subcutaneous panniculitis-like T-cell lymphoma* Mycosis fungoides/Sézary syndrome Anaplastic large cell lymphoma, T/null cell, primary cutaneous type Peripheral T-cell lymphoma, not otherwise characterized Angioimmunoblastic T-cell lymphoma Anaplastic large cell lymphoma, T/null cell, primary systemic type Hodgkin’s Lymphoma (Hodgkin’s Disease) Nodular lymphocyte predominance Hodgkin’s lymphoma Classic Hodgkin’s lymphoma Nodular sclerosis Hodgkin’s lymphoma (grades 1 and 2) Lymphocyte-rich classic Hodgkin’s lymphoma Mixed cellularity Hodgkin’s lymphoma Lymphocyte depletion Hodgkin’s lymphoma ‡ Formerly known as lymphoplasmacytoid lymphoma or immunocytoma II Entities formally grouped under the heading large granular † Not described in REAL classification lymphocyte § Includes the so-called Burkitt-like lymphomas leukemia of T- and NK-cell types * Provisional entities in the REAL classification ** Formerly known as intestinal T-cell lymphoma # Formerly know as angiocentric lymphoma
Non-Hodgkin’s Lymphoma Specific Types Time For A Deep Breath… or an Excedrin
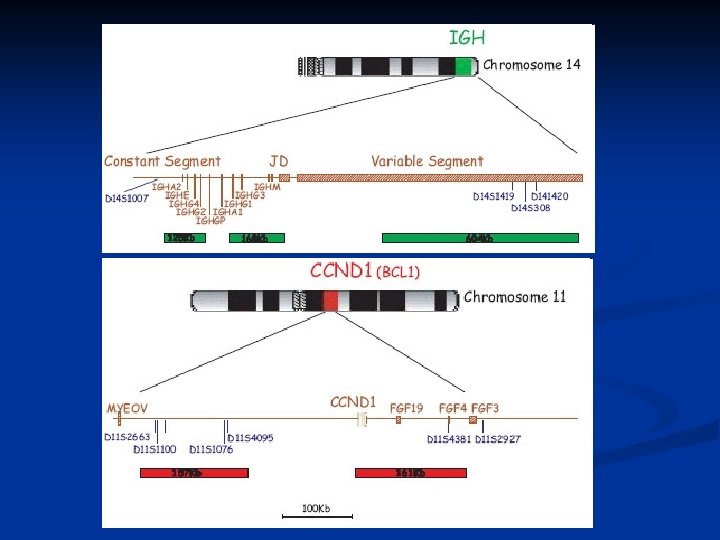
Follicular Lymphoma Mbr (major breakpoint region, 150 bp) Bcl 2 Chromosome 18 C Chromosome 14 JH Double strand DNA break by RAG 1/2 Translocation takes place in B cell precursors. Bcl 2 t(14; 18) translocation C Transformation takes place during B cell activation in GC. bcl 2 E C Unregulation of Bcl 2 expression by Ig. H enhancers C 3’E
Bcl 2 inhibits apoptosis Pro-survival oncogene mitochondrion Bax, Bad Pro-caspase-9 cytochrome c Bcl-2, Bcl-XL Apaf-1 d. ATP or ATP Caspase-9 Apaf-1 Pro-caspase-3 Caspase-3 Apoptosis
Over-expression of Bcl-2 may prevent the apoptosis of germinal center B cells Plasma cells Germinal center activation apoptosis Memory cells Germinal center Ig. H-Bcl 2 activation Most follicular lymphoma Ig V regions contain somatic hypermutation. follicular lymphoma Apoptosis inhibited
Non-Hodgkin’s Lymphoma Follicular Lymphoma n Low-grade lymphoma Grade 1 – Small cell n Grade 2 – Mixed cell n Grade 3 – Large cell n n Indolent in growth Chemotherapy sensitive Incurable
Non-Hodgkin’s Lymphoma Cutaneous T-Cell (Mycosis Fungoides) n n n Low-grade/Indolent lymphoma Radiation therapy sensitive Total Skin Electron Beam Therapy Control disease for years Peripheralization of lymphoma cells = Sezary Cell Sezary Syndrome
Non-Hodgkin’s Lymphoma Diffuse Large Cell n n Very Aggressive Curable if chemo-sensitive upfront, not so if chemo-refractory or relapses within 6 months Most common of all lymphomas Accounts for ~ 31% of all lymphomas
Non-Hodgkin’s Lymphoma Mantle Cell n n Aggressive Accounts for ~ 6% of all lymphomas Incurable with standard-dose therapy Stem cell transplant is offered often as front-line consolidation treatment in “younger” patients
Mantle Cell Lymphoma
Morphology Classical Mantle Cell Nodular pattern Diffuse pattern Blastoid Variant
Mantle Cell - Treatment n CHOP + Rituxan 40 patients (new diagnosis) n CR 48%, PR 48% n Molecular CR seen in 36% of patients with PCR detectable cyclin D 1/Ig. H translocation n Median PFS 16. 6 months, all patients relapsed by 36 months No significant difference in PFS for patients having a clinical or molecular CR n n Howard, O et al. , JCO, 20 (5): 1288
Non-Hodgkin’s Lymphoma Marginal Zone n n n Indolent Accounts for ~10% of all lymphomas Subcategories n n MALT (H. pylori) Nodal Extra-Nodal Splenic
Non-Hodgkin’s Lymphoma Splenic Lymphoma
Non-Hodgkin’s Lymphoma Primary CNS Lymphoma n n Aggressive with poor outcome Accounts for ~ 1 -2% of all lymphomas Different chemotherapy treatments Often requires radiation to the brain: n n Brain dysfunction in younger patients Dementia in older patients
Non-Hodgkin’s Lymphoma Anaplastic Large Cell Lymphoma n n Aggressive Accounts for ~ 2% of all lymphomas n ALCL ALK-1+ better prognosis, more common in younger patients and children n ALCL ALK-1 -negative : as bad as any other Tcell lymphoma
Treatment results of aggressive advanced non-Hodgkin’s lymphomas using different chemotherapy programs 1. First-generation: CHOP - CR: 50 -55%. Long-term survival: 35 -50 %. 2. Second-generation: m. BACOD, Pro. MACE-Cyta. BOM - CR: 70 -80%. Long-term survival: 50 -60%. 3. Third-generation: MACOP-B - CR: 84%. Long-term survival: 75%
Non-Hodgkin’s Lymphoma Intergroup 0067 Study 3 -year survival Mortality ___%________%___ CHOP m. BACOD Pro. MACE-Cyto. BOM 3 MACOP-B 6 41 46 46 41 1 5 Southwest Oncology Group
Non-Hodgkin’s Lymphoma Treatment of Patients Age over 60 Program________5 -year survival % CHOP m. BACOD Pro. MACE-Cyto. BOM MACOP-B 45 39 41 23
t
Non-Hodgkin’s Lymphoma Peripheral T-cell Lymphoma n n Aggressive Accounts for ~ 7% of all lymphomas Very poor prognosis, often associated with extra-nodal presentation Often requiring salvage treatment and transplant
Burkitt’s Lymphoma breakpoints Chromosome 8 myc *** V(D)J S E C Ig. H Chromosome 14, 80% Ig Chromosome 2 Ig chromosome 22 Class switch recombination Somatic hypermutation myc S E C C 3’E t(8: 14) C S C 3’E
Non-Hodgkin’s Lymphoma Burkitt’s NHL n n Very Aggressive Curable with standard-dose therapy but requires very extensive chemotherapy protocol Translocation t(8, 14) Specific Hematopathology Finding n Starry, Starry Night
Burkitt’s Lymhoma Starry, Starry Night
Non-Hodgkin’s Lymphoma Lymphoblastic NHL n n n Very aggressive Treatment is with acute lymphocytic leukemia regimen Often requires high-dose therapy and allogeneic transplantation for relapsed/refractory disease
Gamma Delta-T-cell NHL n n Very, very aggressive Very poor outcome with standard-dose therapy High-dose therapy and allogeneic transplantation is standard-of-care in first remission CD 57 protein positivity
Double-Hit Lymphomas n Multiple gene expressions MYC gene n t(14, 18) n n Triple-Hit MYC gene n t(14, 18) n BCL-6 gene n
Non-Hodgkin’s Lymphoma Aggressive chemotherapy regimens n n n Dose-dense CHOP-Bleo CEOP-Bleo Dexa. BEAM Hyper. CVAD
BMT for Non-Hodgkin’s Lymphoma Indications 1. Refractory disease 2. Relapse 3. High risk in CR 4. Lymphoblastic, Burkitt’s, and gamma delta-t-cell lymphomas
PROBABILITY OF SURVIVAL AFTER AUTOTRANSPLANTS FOR FOLLICULAR NON-HODGKIN LYMPHOMA 100 PROBABILITY, % 80 CR 1 (N = 174) CR 2+ (N = 322) 60 Never in remission (N = 418) Relapse (N = 791) 40 20 P = 0. 0009 0 0 1 2 3 YEARS 4 5 6
PROBABILITY OF SURVIVAL AFTER HLAIDENTICAL SIBLING MYELOABLATIVE TRANSPLANTS FOR FOLLICULAR NON-HODGKIN LYMPHOMA 100 Never in remission (N = 138) PROBABILITY, % 80 CR 1 -3 (N = 79) 60 Relapse (N = 193) 40 20 P = NS 0 0 1 2 3 YEARS 4 5 6
PROBABILITY OF SURVIVAL AFTER AUTOTRANSPLANTS FOR DIFFUSE LARGE CELL LYMPHOMA 100 PROBABILITY, % 80 CR 1 (N = 438) 60 CR 2+ (N = 651) 40 Relapse (N = 1, 443) 20 Never in remission (N = 986) P = 0. 0001 0 0 1 2 3 YEARS 4 5 6
PROBABILITY OF SURVIVAL AFTER HLAIDENTICAL SIBLING MYELOABLATIVE TRANSPLANTS FOR DIFFUSE LARGE CELL LYMPHOMA 100 PROBABILITY, % 80 60 40 Relapse (N = 144) CR 1 -3 (N = 56) Never in remission (N = 133) 20 P = NS 0 0 1 2 3 YEARS 4 5 6
Monoclonal Abs - Rituxan
Radioimmunotherapy with Y-90 Zevalin Monoclonal antibody n Ibritumomab n Murine monoclonal antibody parent of Rituximab n Tiuxetan n n Chelator Y-90 radionuclide Conjugated to antibody, forming strong urea-type bond Stable retention of Y-90 Beta radiation
New Treatment Options n n Velcade + Flavoperidol – MCC Trial Velcade + Darinaparsin
Conclusion n Discussed Hodgkin’s Disease n Discussed Non-Hodgkin’s Lymphoma n Discussed Classification Systems n Discussed Treatment Options