Non Hodgkins lymphoma Rakesh Biswas MD Professor Department

Non Hodgkin’s lymphoma Rakesh Biswas MD, Professor, Department of Medicine, People's College of Medical Sciences, Bhanpur, Bhopal, India

 or extra")
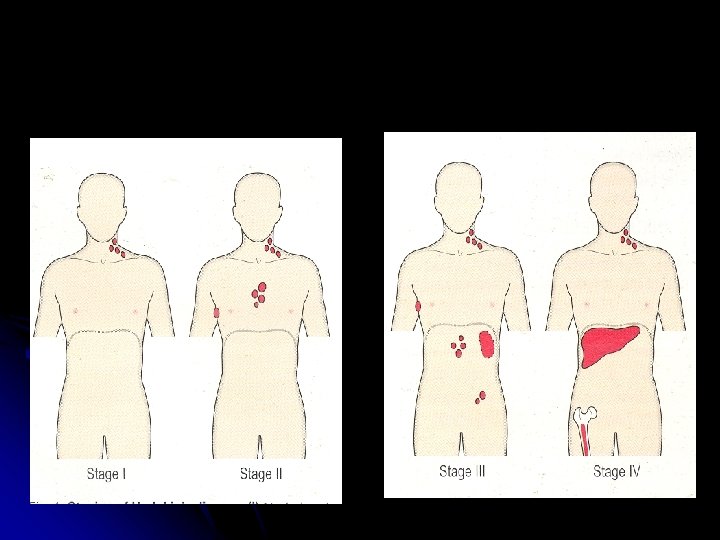
Staging l l Stage I : Involvement of single LN region (I) or extra lymphatic site (IAE ) Stage II : Two or more LN regions involved (II) or an extra lymphatic site and lymph node regions on the same side of diaphragm Stage III : Involvement of lymph node regions on both sides of diaphragm, with (IIIE) or without (III) localized extra lymphatic involvement or involvement of the spleen (IIS) or both (IISE) Stage IV : Involvement outside LN areas (Liver, bone marrow) A : Absence of ‘B’ symptoms B : B symptoms present

Non Hodgkin’s lymphoma Incidence is increasing l NHL>HD l Median age of presentation is 65 -70 yrs l M>F l More often clinically disseminated at diagnosis l B-cell-70% ; T-cell-30% l

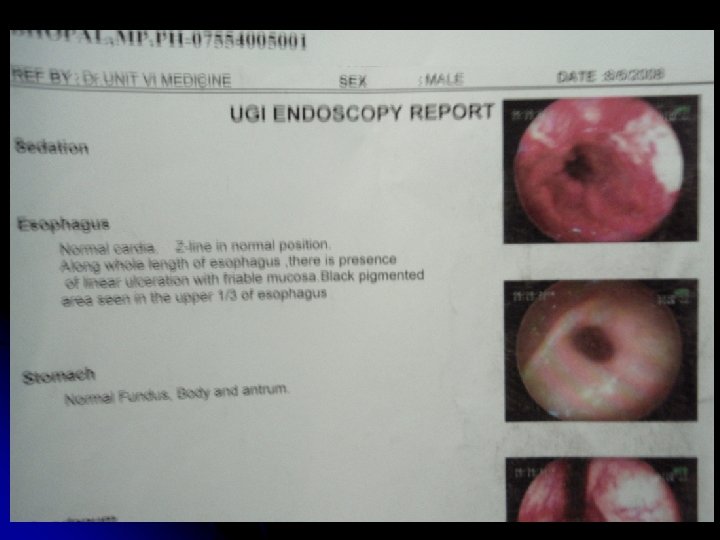
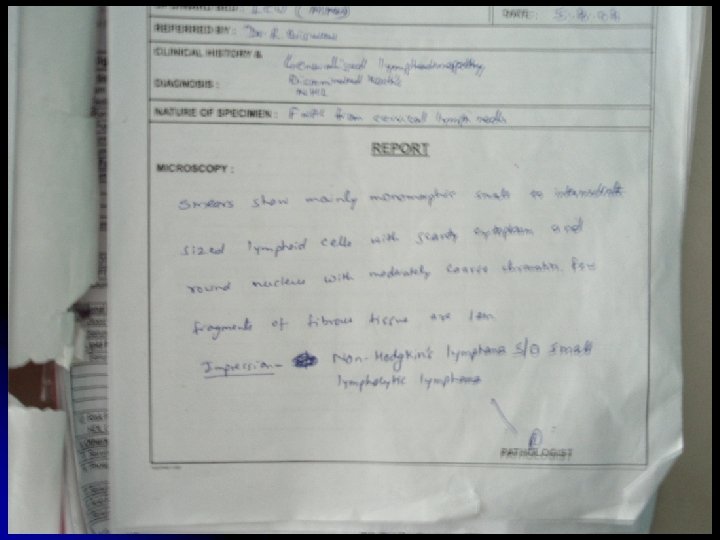
Clinical features l l Widely disseminated at presentation Nodal involvement: Painless lymphadenopathy, often cervical region is the most common presentation Hepatospleenomegaly Extranodal : Intestinal lymphoma ( abdominal pain, anemia, dysphagia); CNS ( headache, cranial nerve palsies, spinal cord compression) ; Skin, Testis; Thyroid; Lung Bone marrow (low grade): Pancytopenia

Clinical features contd § Systemic symptoms l l l Sweating, weight loss, itching Metabolic complications: hyperuricemia, hypercalcemia, renal failure Compression syndrome: l l Gut obstruction Ascites SVC obstruction S/C Compression

Classification REAL l Clinical / Working Formulation l l Low grade l Intermediate grade l High grade

Classification Proliferation: Course: Symptoms: Treatment: Low grade High grade Low Indolent -ve Not curable High Rapid, fatal(un-Rx) +ve Potentially Curable
 l Infection:")
Etiology l Cannot be attributed a single cause Chromosomal translocations: (14, 18) l Infection: l l Virus: EBV, HTLV, HHV-8, HIV Bacteria: H. Pylori - Gastric lymphoma Immunology: l l Congenital immunodeficiency, Immunocompromised patients - HIV, organ transplantation t

Management l l l Low grade: Asymptomatic : No treatment ; Radiotherapy for localised disease (Stage 1); Chemotherapy: mainstay is Chlorambucil; Initial response good , but repeated relapses, median survival 6 -10 yrs; l l l Newer: Fludarabine, 2 -Cd. A (Chlorodeoxyadenosine) Monoclonal antibody: Rituximab SCT/BMT
: l Chemotherapy: mainstay CHOP -every 3 weeks, at")
Aggressive ( high / intermediate grade): l Chemotherapy: mainstay CHOP -every 3 weeks, at least 6 cycles Cyclophosphamide, Doxorubicin Hydrochloride, Vincristine, Prednisolone

l High risk cases with poor prognostic factors or relapse : High dose chemotherapy combined with autologous BMT / SCT l Monoclonal antibody l With CNS involvement / leukemic relapse : Similar to ALL

Prognosis Low grade : Median survival – 10 yrs l High Grade: l l Increasing age, advanced stage, concomitant disease, raised LDH, T- cell phenotype : Poor prognosis
- Slides: 16