Goals Understand the differences between Hodgkin Lymphoma and

Goals • Understand the differences between Hodgkin Lymphoma and non-Hodgkin Lymphoma – Clinically and biologically • Understand the differences between aggressive NHL and indolent NHL – Clinically and biologically

C Definition of Lymphoma • Heterogeneous group of lymphoproliferative malignancies – Results from clonal expansion of tumor cells derived from B, T, or NK cells – 85%-90% in the US are derived from B cells • Variable clinical presentations – Range from asymptomatic pick up on routine blood work to painless adenopathy to an emergent medical problem • Pain, failure to thrive, organ failure • Characterized by variable natural histories and therapeutic responses

Age at Diagnosis for Hodgkin’s and Non-Hodgkin’s Lymphoma ~56, 390 NHL cases/y ~7, 350 HD cases/y Cases/100, 000 NHL Hodgkin’s Age at diagnosis (y) Data for diagnoses from 1997 to 2001. At: http: //seer. cancer. gov. Accessed March 23, 2005.

Estimated annual incidence Non-Hodgkin’s Lymphoma: Epidemiology ~4% compound annual increase in incidence Year Adapted from Greenlee et al. CA Cancer J Clin. 2001; 51: 15. Adapted from Jemal et al. CA Cancer J Clin. 2005; 55: 10.

Hodgkin’s Disease

Hodgkin Biology • RS is a “crippled” germinal center B cell – does not have normal B cell surface antigens – micromanipulation of single RS followed by PCR demonstrates clonally rearranged, but non functional immunoglobulin genes • somatic mutations result in stop codon (no s. Ig) • no apoptotic death malignant transformation – unclear how this occurs; ? EBV – unclear how cells end up with RS phenotype

Hodgkin’s Disease • Clinical features – Often seen in young adults – Wide variety of presentations • • • B symptoms (fevers, night sweats, wt loss) Pruritis Cough/SOB Painless adenopathy

Hodgkin’s Disease • Approach to the Patient – staging evaluation • • • H&P CBC, diff, plts ESR, LDH, albumin, LFT’s, Cr CT scans chest/abd/pelvis bone marrow evaluation PET scan in selected cases

Ann Arbor Staging System for Hodgkin's Disease and Non. Hodgkin's Lymphoma Stage III Stage IV Reprinted with permission. Adapted from Skarin. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology. 1991.

Hodgkin’s Disease • Typical staging results – Most often disease is localized to above the diaphragm – Common to have extensive mediastinal disease • Tends to spread to contiguous nodal groups – Unlike NHL

Approach to the Patient • Hodgkin’s Disease – approach dictated mainly by where the disease is located rather (results of staging) than the exact histologic subtype • NHL – approach is often dictated more by the histologic subtype than the results of staging

Hodgkin Lymphoma: Treatment of limited stage disease

Hodgkin Lymphoma: Prognostic Factors

Hodgkins Disease Summary • B cell lymphoma - several histologic subtypes - Generally does not affect the approach to the patient – Reed-Sternberg Cells • • • Tends to occur in young adults Mediastinal disease common Spreads to contiguous nodes Common to have a “localized” presentation Highly curable with current treatments
, T cell, NK")
Non-Hodgkin’s Lymphoma • 30 ish histologic subtypes – B cell (85%), T cell, NK cell – Histologic subtype dictates the approach to the patient • Median age at diagnosis 60 • Often widespread disease at diagnosis • Wide variation in outcome – Some cases rapidly fatal – Some cases readily curable – Some cases incurable but patient can live for many years with good quality of life
 B-cell")
WHO Classification: B-Cell Malignancies Precursor B-cell neoplasm • Precursor B-lymphoblastic leukemia/lymphoma Mature (peripheral) B-cell neoplasms • B-cell chronic lymphocytic leukemia/ small lymphocytic lymphoma • Hairy cell leukemia • B-cell prolymphocytic leukemia • Plasma-cell myeloma/ plasmacytoma • Lymphoplasmacytic lymphoma • Follicular lymphoma • Splenic marginal-zone B-cell lymphoma • Mantle-cell lymphoma • Nodal marginal-zone lymphoma • Diffuse large B-cell lymphoma (DLBCL) • Extranodal marginal-zone B-cell lymphoma, mucosa-associated lymphoid tissue (MALT) type • Burkitt's lymphoma/Burkitt's cell leukemia • Blastic NK-cell leukemia Harris NL et al. J Clin Oncol. 1999; 17: 3835 -3849.
 T-cell")
WHO Classification: T-Cell Malignancies Precursor T-cell neoplasm • Precursor T-lymphoblastic leukemia/lymphoma Mature (peripheral) T-cell neoplasms • T-cell prolymphocytic leukemia • T-cell granular lymphocytic leukemia • Subcutaneous panniculitis-like T-cell lymphoma • Aggressive NK-cell leukemia • Mycosis fungoides/Sézary syndrome • Adult T-cell lymphoma/leukemia (HTLV 1+) • Primary cutaneous anaplastic large cell lymphoma, T/null cell • Extranodal NK/T-cell lymphoma, nasal type • Enteropathy-type T-cell lymphoma • Hepatosplenic gamma-delta T-cell lymphoma • Peripheral T-cell lymphoma, unspecified • Angioimmunoblastic T-cell lymphoma • Primary systemic anaplastic large cell lymphoma, T/null cell • Blastic NK lymphoma Harris NL et al. J Clin Oncol. 1999; 17: 3835 -3849.

B-Cell Development Stem cell Immature B cell s-Ig. M CD 79 a Td. T HLA-DR CD 79 a CD 22 CD 21 CD 20 CD 34 Follicle-center B cell s-Ig. M/G/A CD 22 CD 10 bcl 6 HLA-DR CD 21 CD 20 CD 19 Pre-pre–B cell s-Ig. M/G/A Td. T c-CD 22 c. CD 79 a HLA-DR Immunoblast CD 19 CD 10 Td. T c-CD 22 c. CD 79 a c-m CD 20 CD 79 a HLA-DR CD 19 HLA-DR MUM 1 CD 21 HLA-DR CD 19 CD 20 CD 19 CD 138± c-Ig s-Ig. M & Ig. D CD 22 Pre–B cell CD 22 CD 79 a Mature B cell CD 20 Plasma cell CD 79 a c-Ig Precursor cells Virgin (naïve) B cells Germinal-center and post–germinal-center B cells CD 138 PCA-1 MUM 1

Antigen Expression in BCell Lineage ALL Stem cell MCL, CLL Pre-B Early B Burkitts, FL, DLBCL Mature B Activated B WM Plasmacytoid B Germinal center Type of B cell lymphoma is a function of: 1) Where the cell was in development/maturation when it went “bad” 2) What molecular derangement occurred Jaffe. In: Non-Hodgkin’s Lymphoma. 1997: 84. MM Plasma

Models of Chromosomal Translocations in NHL REG CODING REG Protooncogene TRANSLOCATION REG CODING TRANSCRIPTIONAL DEREGULATION CODING Protooncogene TRANSLOCATION REG CODING FUSION PROTEIN REG = regulatory sequence. Harris NL et al. Hematology (Am Soc Hematol Educ Program). 2001: 194 -220.

Chromosomal Translocations Commonly Associated With Activation in B-Cell Malignancies Oncogene Protein Translocation Disease bcl-1 Cyclin D 1 t(11; 14) MCL bcl-2 BCL 2 (antiapoptosis) t(14; 18) FL myc Transcription factor t(8; 14) Burkitt’s NHL bcl-6 Zinc-finger transcription factor t(3; 14) DLBCL (some follicular NHL) National Comprehensive Cancer Network. Practice Guidelines in Oncology. v. 1. 2005.

Lymphoma Biology • Aggressive NHL – short natural history (patients die within months if untreated) – disease of rapid cellular proliferation – Potentially curable with chemotherapy • Indolent NHL – long natural history (patients can live for many years untreated) – disease of slow cellular accumulation – Generally incurable with chemotherapy

NHL: Presentation and Staging • Aggressive NHL – Patients likely to present with symptoms • Indolent NHL – Patients likely to present with painless adenopathy • Initial workup similar to Hodgkin Lymphoma

NHL: Approach to the Patient • Approach dictated mainly by histology – reliable hematopathology crucial • Aggressive NHL – Cure is often the goal • Indolent NHL – Cure is rarely the goal – Control is the goal
 Diffuse large B-cell 31 Follicular 22 Marginal-zone B-cell,")
Most Common NHLs Category Frequency (%) Diffuse large B-cell 31 Follicular 22 Marginal-zone B-cell, MALT 8 Peripheral T-cell 7 Small B-lymphocytic/CLL 7 Mantle-cell lymphoma 6 Primary mediastinal large B-cell 2 Anaplastic large T/null cell 2 High-grade B-cell, Burkitt-like 2 Marginal-zone B-cell, nodal 2 Precursor T-lymphoblastic lymphoma 2 Armitage JO, Weisenburger DD. J Clin Oncol. 1998; 16: 2780 -2795.

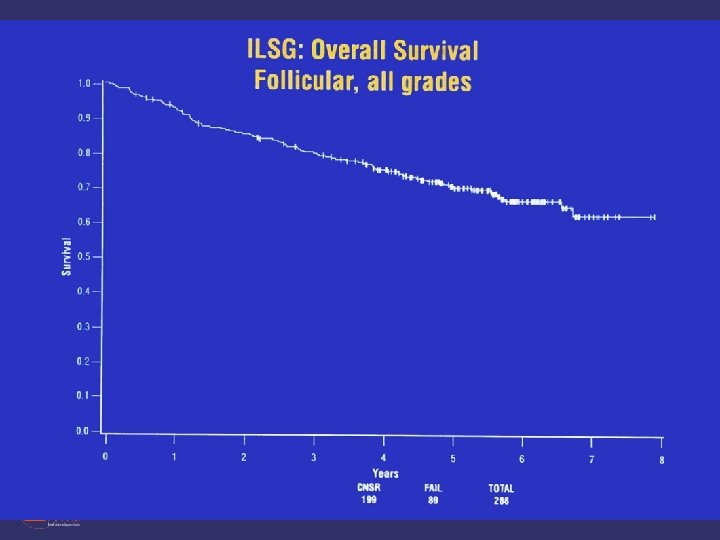
Follicular Lymphoma

Approach to Indolent NHL • Indolent NHL: guiding treatment principle • immediate treatment does not prolong overall survival for many patients – When to treat? • constitutional symptoms • compromise of a vital organ by compression or infiltration, particularly the bone marrow • bulky adenopathy • rapid progression • evidence of transformation • Will often begin with relatively non-toxic treatments and escalate the intensity of therapy

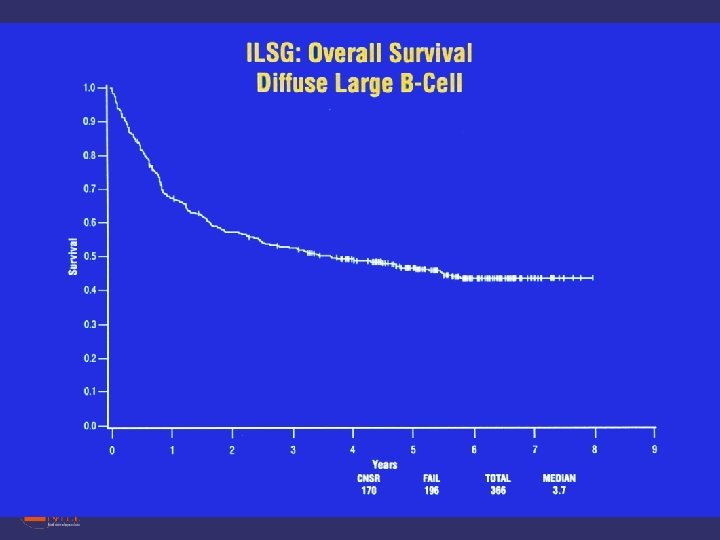
Diffuse Large B Cell Lymphoma

Approach to Aggressive NHL • Patients have the potential to be cured – Administer most effective therapy (no matter how harsh) at diagnosis – If not cured, patients typically die within a few years of diagnosis

International Prognostic Index for Age-Adjusted Factor Adverse PS LDH Stage ≥ 2 >Normal III-IV Number of Factors Present 5 -year DFS Age≤ 60 (%) 5 -year OS Age≤ 60 (%) Low 0 86 83 Low-Intermediate 1 66 69 High-Intermediate 2 53 46 High 3 58 32 Risk Group The International Non-Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med. 1993; 329: 987 -994.

DLBCL: Subtypes Revealed by Expression Array Probability 1. 0 Germinal-center B-cell–like 0. 8 0. 6 Activated B-cell–like 0. 4 0. 2 P = 7. 9 E-6 0. 0 0 Single histology with multiple molecular subtypes 2 4 6 8 Overall survival (years) 10 …with different outcomes Alizadeh AA et al. Nature. 2000; 403: 503 -511.

Summary • NHL incidence increasing • Hodgkin incidence stable or decreasing • Hodgkin Lymphoma – – – – Characterized by the Reed-Sternberg Cells Stage more important that histologic subtype Often limited stage (stage I or II) Spreads to contiguous nodes Often affects younger patients Very responsive to therapy Cure rate quite high

Summary • NHL cure rate mediocre – Many histologic subtypes • Often more important that the stage – indolent vs. aggressive • Function of underlying biology – indolent: • Often asymptomatic • Treatment: Less is more – aggressive: • Often symptomatic • require aggressive treatment ASAP to achieve cure
- Slides: 35