General algorithm for PSG Interpretation What symptoms or






 = From “ light out” to “light")

 = TRT Light Off Light On W W N")
 • Low TRT - Short sleeper Disturbed")
 • Low TST - Short sleeper")
 • Low SE - Short sleeper -")

 • short SL - Normal sleeper -")



")

 Apnea event + Hypopnea event + RERA")

 ( Apnea-Hypopnea Index) (Respiratory Disturbance")

 1) A clear")
 event AASM task work 1999 Pattern of progressively more negative")




















 : Mild OSA Occurred almost exclusively during")










 Mod.")
- Slides: 63
General algorithm for PSG Interpretation What symptoms or complaints Review raw data Determine range of normal values Review the sleep log sleep recording, technologist note, patients questionnaires age- , sex- related range TIB, TST, No. of awakening, Usual bed time and wake time Compare the values in the PSG Explain any discrepancies What values in the PSG summary are artifact What values are representative of the patient’s usual sleep Make a final statement and diagnosis 서울수면센타
Full Polysomnography n. PSG - EEG, EOG, EMG, Airflow, EKG, Pulse, Sp. O 2, Snoring, Position, respiratory effort (chest and abdominal movement), etc. . 서울수면센타
Diagnosis of OSA RDI Increased respiratory effort Increased autonomic nerve activity Decreased Oxygen desaturation Cardiovascular complication Arousal PSG EEG Arousal EKG Oxymeter 서울수면센타
Increased inspiratory effort Critical points of PSG Hypoxemia Sleep fragmentation 서울수면센타
What is the value of PSG? 1. 2. 3. 4. 5. 6. To To To ensure slept ensure REM sleep avoid scoring events in wakefulness diagnose other sleep disorders detect EEG arousals provide denominator for AHI 서울수면센타
Evaluation of Sleep states • • • Total Recording Time Total Sleep Time Sleep Efficiency Total Wake Time Wake After Sleep Onset( WASO) • Sleep Latency • REM Latency 서울수면센타
Sleep architecture definitions • Total Recording Time(TRT) = From “ light out” to “light on” • Total Sleep Time(TST) = minutes of stage 1 -4 + REM • Sleep efficiency (SE) = TST/ TRT or TIB • Wake after sleep onset (WASO) = minutes of wake after sleep onset but before the final awakening • Sleep Period Time (SPT)= WASO+TST 서울수면센타
• Sleep latency = lights out until first epoch of sleep • REM latency = time from the first sleep until start of REM sleep (normal 70 -120 minutes) • SO-REM latency: narcolepsy, depression, sleep apnea, withdrawal of drugs suppressing REM 서울수면센타
Sleep architecture definitions TST SE(%) = TRT Light Off Light On W W N 1 N 2 N 3 R W N 2 W R W WASO SL REM Latency TST SPT TRT 서울수면센타
Possible explanations for atypical Total Recording Time(TRT) • Low TRT - Short sleeper Disturbed by lab. environment First night effect (FNF) Depression/anxiety Sleep/wake schedule disorder Alerting medication Recent nap • High TRT - Long sleeper - Rebound sleep. Prior restriction of TIB. Elimination of sleep fragmentation(CPAP) - Anticipatory anxiety about not sleeping - Better mattress, pillow, service - Sedating medication 서울수면센타
Possible explanations for atypical total Sleep Time (TST) • Low TST - Short sleeper - Sleep disorders. Frequent arousal. difficulty falling asleep. early morning awakening. difficulty Returning to sleep after awakening - Disturbed by lab. environment - First night effect (FNF) - Depression/anxiety - Sleep/wake schedule disorder - Alerting medication - Recent nap • High TST - Long sleeper - Rebound sleep. Prior restriction of TIB. Elimination of sleep fragmentation(CPAP) - Lack of usual time pressures - Work, family, or marital related stresses not present - Better mattress, pillow, service - Felt more secure - Sedating medication 서울수면센타
Possible explanations for atypical Sleep efficiency (SE) • Low SE - Short sleeper - Sleep disorders - First night effect (FNF). Long sleep latency. Frequent arousal - Depression/anxiety - Excessive napping - Alerting medication - Disturbed by lab. Environment. Noise/Light/temperature. Uncomfortable bed. Technician into sleep room • High SE - Normal sleeper - Rebound sleep. Prior restriction of TIB. Elimination of sleep fragmentation(CPAP) - Periods of wakefulness too short( R & K rule) 서울수면센타
Possible explanations for WASO • High WASO - Environmental disturbance. Noise/Light/temperature/uncomfortable bed . Technician into sleep room - Sleep disorders. Sleep apnea/PLMS/RBD/Parasomnia/Seizures - FNE - Activating medication/alcohol/caffeine/nicotine effects - Anxiety/depression 서울수면센타
Possible explanations for atypical Sleep latency (SL) • short SL - Normal sleeper - Rebound sleep - Medication. Hypnotics/sedatives. Alcohol effects - Successful Tx. of sleep disorders - Good lab. Environment • long SL - Insomnia RLS Anxiety/depression FNE Sleep/wake schedule disturbance. Shift work/Jet leg/DSPS. On call/Hospitalization - Age effects - Caffeine, nicotine, alerting med. - Environment. Noise/Light/temperature. Uncomfortable bed. Technician into sleep room 서울수면센타
Possible explanations for atypical REM latency • Short REM latency - Narcolepsy - Sleep apnea - Sleep/wake schedule disturbance - Medication (Withdrawal from REM-suppression). TCA/MAO inhibitors/amphetamine. Barbiturates/alcohol - Depression - Rebound sleep - bed time later than usual bedtime • Long REM latency - Fragmented NREM sleep. Sleep apnea. PLMS - FNE - REM-suppression medication - Sleep/wake schedule disturbance - Bed time earlier than usual bedtime 서울수면센타
Evaluation of EEG Parameters Sleep stage • Stage 1, 2, 3, 4. • REM • Wake 서울수면센타
Normal Sleep stage – age. sex 서울수면센타
Evaluation of EEG Parameters Arousal • Spontaneous arousal • Respiratory Effort Related Arousal (RERA) • Leg movement arousal 서울수면센타
Arousal • Definition An abrupt shift in EEG frequency, which may include theta, alpha and/or frequencies greater than 16 Hz but not spindle. • Scoring rules 1. Subject must be asleep, defined as 10 or more continuous seconds or more, before an EEG arousal. 2. A minimum of 10 continuous seconds of intervening sleep is necessary to score a second arousal. 3. The EEG frequency shift must be 3 seconds or greater in duration 4. Arousal are scored in REM sleep only when accompanied by concurrent increase in submental EMG amplitude 5 etc. 서울수면센타
Respiratory event • RDI( Respiratory disturbance index) Apnea event + Hypopnea event + RERA 서울수면센타
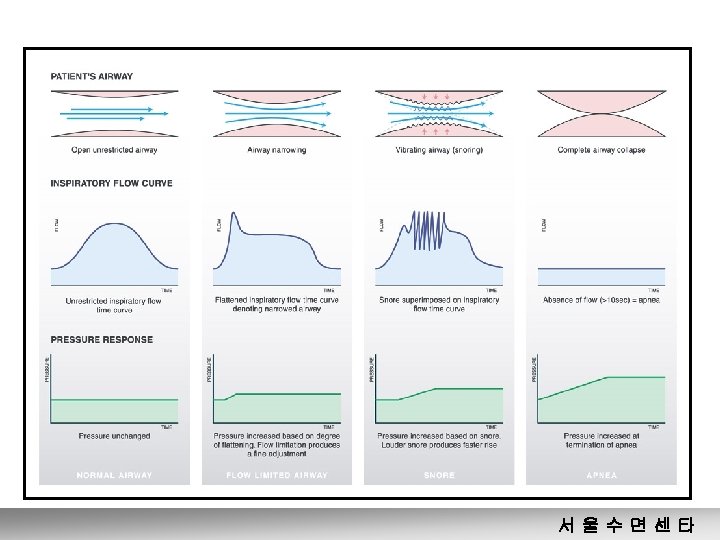
Snoring Thermister Flow limitation Respiratory effort Abd. and rib cage movements Intrathoracic effects on BP 서울수면센타
Evaluation of Respiratory Parameters AI AHI RDI (Apnea Index) ( Apnea-Hypopnea Index) (Respiratory Disturbance Index) 서울수면센타
Respiratory event - Apnea • Definition ; Cessation of airflow for at least 10 seconds documented on a PSG - Obstructive - Mixed - Central 서울수면센타
Respiratory event - Hypopnea • Chicago criteria (AASM Task Force, 1999) 1) A clear decrease(>50%) from baseline in the amplitude of a valid measure of breathing. 2) A clear amplitude reduction of a validated measure of breathing during sleep that dose not reach the above criterion but is associated with either an oxygen desaturation of >3% or arousal. 3) The event lasts 10 seconds or longer • Medicare Criteria an abnormal respiratory event lasting at least 10 seconds associated with at least a 30% reduction in thoracoabdominal movement or airflow as compared to baseline, and with at least a 4% decrease in oxygen saturation 서울수면센타
Respiratory effort-related arousal (RERA) event AASM task work 1999 Pattern of progressively more negative esophageal pressure, terminated by a sudden change in pressure to a less negative level and an arousal. 2. The event lasts 10 seconds or longer. 3. It is not long enough or of sufficient magnitude to be classified as a hypopnea. 4. Esophageal monitoring is still the gold standard for detecting RERAs. (sleep 1997; 20: 654 -675) 1. 서울수면센타
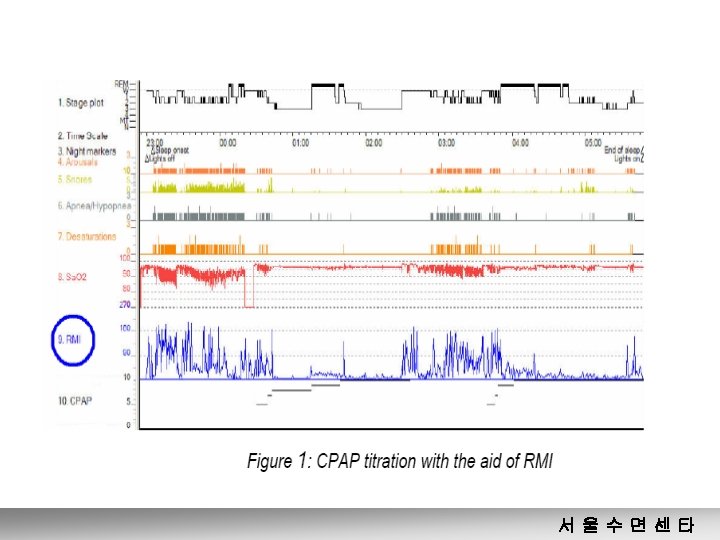
RMI is Model based Variance in phase between the 2 effort signals = Respiratory Mechanics Instability (RMI) %Time in RMI state: RMI-index 서울수면센타
RMI and CPAP titration • Upper airway mechanics is unstable under too low CPAP pressure as well as • Under too high CPAP pressure 서울수면센타
Evaluation of Respiratory Parameters • Position and apnea 서울수면센타
Body position • Sleep in the laboratory vs. at home - Patients could not sleep in their usual position due to the electrodes sensors, or CPAP mask. - Spending more time in a supine position in the sleep laboratory than at home. • Effect of body position on the sleep apnea - Body position, esp. supine, are potentially critical because of the effects on the sleep apnea. - OSA may occur only with the patient in the supine position and maybe exacerbated by change to the supine position 서울수면센타
Body position • Diagnostic Problems with Body Position - the laboratory technical staff can request that the patient assume certain body position during the sleep study for certain period of time. - It may be necessary during CPAP titrations or split night protocol - sleep apnea is likely to be most severe when the patient is sleeping in the supine position during REM sleep. - the highest RDI is not present during REM sleep because REM sleep-related apnea and hypopnea have longer duration and so a lower RDI 서울수면센타
Evaluation of Respiratory Parameters • REM/NREM and apnea 서울수면센타
Evaluation of cardiorespiratory Parameters • Nadir Sa. O 2 • Average Desaturation • % of hypoxemia (< 90%) 서울수면센타
Oxygen desaturation • Hypoxemia normal range of oxygen saturation is 90~100%, with values below this level labeled as hypoxemia. • Transient vs. Chronic decline in Sa. O 2 (4 pattern) - Normal Sa. O 2. ; no state or body position shift. - Short-term drop in Sa. O 2 <90%. - Chronic or long term hypoxemia(Sa. O 2<90%) - Repetitive O 2 desaturation. (M/C OSA) ; drop >2 -4% usually <60 sec. 서울수면센타
Desaturation vs. other PSG variables • Correlation of OSAS consequences with AHI and arousals poor, • Sa. O 2 better for both sleepiness Kingshott. ERJ 1998; 12: 1264 -70 Bennett. AJRCCM 1998; 158: 778 -86 + Hypertension Faccenda. AJRCCM 2001; 163: 344 -8 Pepperell. Lancet 2002; 359: 204 -10 서울수면센타
Pattern of Sa. O 2 in OSAS 서울수면센타
ODI 4: 4% oxygen desaturation dip rate AHI vs ODI 4 서울수면센타
4% Sa. O 2 Dip rate vs AHI Vazquez et al Thorax 2000; 55: 302 -307 • 4% Sa. O 2 dip rate : r=0. 97 • 4% Sa. O 2 dip rate or an arousal r=0. 98 • Criteria of 15/h for AHI and RDI sensitivity 98% specificity 88% 서울수면센타
Effect of hypoxia • Effect of Hypoxia on Functioning of the human Brain Sa. O 2(%) Pa. O 2 (mm. Hg) 97 91~81 95 60~45 81~67 45~35 67 35 Clinical status Normal Impaired concentration, short-term memory, Lethargy, euphoria, irritability, hallucination, muscular incoordination Loss of consciousness Gibson et al. Am J Med 1981 서울수면센타
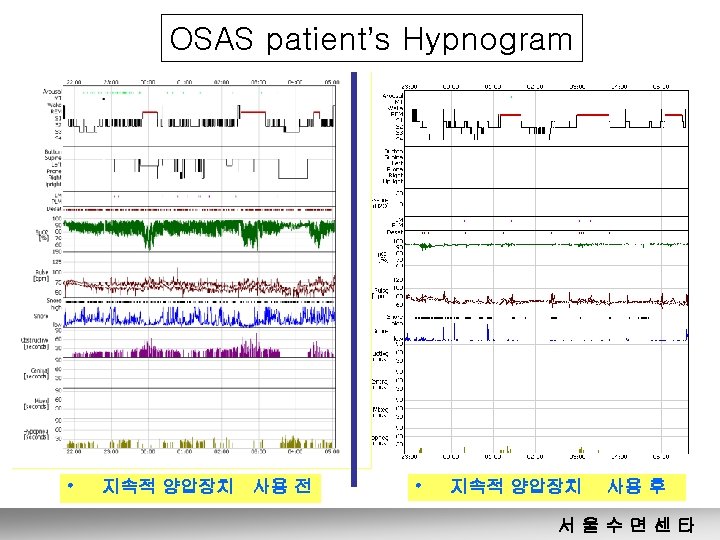
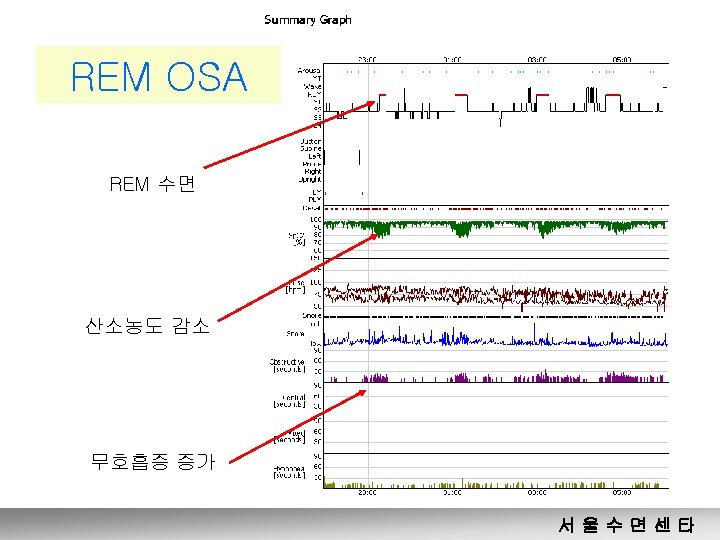
Clinical Hypnogram • Hypnogram 이란? • Example of OSAS patient’s Hypnogram 서울수면센타
Hypnogram 이란? Sleep stage Sleep position Sa. O 2 Pulse rate snoring Apnea event Hypopnea event 서울수면센타
Diagnosis • • • Classification of SDB Determination of severity Type of OSAS Cardiac arrhythmia Mouth breathing 서울수면센타
Spectrum of Sleep Disordered Breathing • • Intermittent snoring Chronic heavy snoring UARS Mild OSA Moderate OSA Severe OSA Obesity hypoventilation syndrome 서울수면센타
Determination of severity rating of sleep disordered breathing - According to RDI • Mild : 5 -15 events/hr • Moderate : 15 -30 events/hr • Severe : >30 events/hr # RDI of 15/hr of sleep was based on a consensus of task force members’ opinion # increased risk hypertension when RDI is >30 American Academy of Sleep Medicine Task Force on SRBD in adult 서울수면센타
RDI Which one is more severe OSA? • A case RDI, 40 Res. events Sp. O 2 • B case 91% 89% 90% 91% RDI, 20 Res. events Sp. O 2 78% 76% 서울수면센타
Mild OSA day time dysfunction RDI Arousal Sp. O 2 Severe OSA cardiovascular complication 서울수면센타
Type of OSA • REM OSA (ROSA) : Mild OSA Occurred almost exclusively during REM sleep defined by AHI(TST) : 10 ~25 AHI(REM)/AHI(Non. REM)>2 AHI(Non. REM) <10 • Supine OSA (SOSA) : OSA occurring almost exclusively in the supine position • OSA independent of sleep stage or sleep position (IOSA) O’Connors et al. Am J Respir Crit Care Med , 2000 서울수면센타
I OSA independent of sleep stage and position 서울수면센타
Potential effects of prior limitations of Sleep Quality or Quantity • • Partial acute or partial cumulative sleep deprivation Sleep fragmentation or poor sleep quality Sleep lab effect: The First Night Effect Rebound sleep : when sleep is better than expected • Effect of medication or withdrawal from medication • Timing of sleep : circadian modulation of sleep/wake system 서울수면센타
RDI가 낮게 나타나는 경우 • REM OSA • Sleep position ( SOSA 에서 Decubitus로 자는 경우) • First Night Effect • Circadian rhythm을 맞추지 못해 REM이 적게 나 타난 경우 • Medication 효과 등 서울수면센타
RDI가 높게 나타나는 경우 • Cumulative sleep deprivation • Rebound sleep • Medication 서울수면센타
First Night Effect ; Sleep lab effect • The poorer sleep of the first night usually consisted of - lower sleep efficiency - more stage 1 sleep - more awakenings - lower quantities of deep sleep 서울수면센타
Medication Effects on sleep Decrease sleep Quality Caffeine Nicotine Theophyline Amphetamines Decrease Deep Sleep Benzodiazepines CNS depressants Decrease REM sleep MAO inhibitors TCAs Amphetamines Barbiturates Alcohol Anticholinergics 서울수면센타
If the patient had not slept in the supine position and little or no REM sleep had occurred, • Interpretation No option other than to say mild OSA, if REM sleep or a supine position had been noted, more severe apnea might have been diagnosed. 서울수면센타
Why do PSG? • Establish diagnosis - History alone is in adequate - Most screening tests sensitive but no specific • • Differential diagnosis Sleep architecture Assess severity & operative risk Provide baseline for F/U 서울수면센타
PSG - Recommendation The presence and severity of obstructive sleep apnea in patients must be determined before initiating surgical therapy Rationale - identifies patients at risk due to complications of sleep apnea - provides a baseline to establish the effectiveness of therapy An American Sleep Disorders Association Practice Parameters for the Treatment of OSA in adult 서울수면센타
Hx, P/E, Cephalometry, Endoscopic Exam Polysomnogram Primary snoring UARS, Mild OSA 해부학적 폐쇄(-) Mod. OSA 해부학적 폐쇄(+) BMI>30 Radiofrequency , implant EDS(+) Yes No 건강상태 Severe OSA CPAP 심혈관계합병증(+) 양호 Oral Appliance No 수술 선호 일정기간사용 후 CPAP에서 벗어나기 원함 실패 시 Yes 실패 시 OPERATION Bi. PAP 서울수면센타