Clinical neurological syndroms Kateina Zrubov Syndrom n association

Clinical neurological syndroms Kateřina Zárubová
 and symptoms")
Syndrom n association of several clinical features, signs (observed by a physician) and symptoms (reported by the patient) that occur together in characteristic combination n important for topic diagnosis

Physical examination in neurology A. Medical history B. Neurological examination - verification of normal function - looking for patologic signs C. Basic steps in making neurological dg. : - 1. syndromologic diagnosis (list of patotologic signs) - 2. topical diagnosis (localization of the lesion) - 3. etiologic diagnosis

Central and peripheral nervous system

Central and peripheral nervous system n n Brain Spinal cord Cranial nerves Peripheral nerves

Central nervous system Brain Supratentorial area n cortex n white matter of hemispheres n thalamus n bazal ganglia Infratentorial area n brainstem n cebellum

Brain lobes Cortical functions n n Frontal lobe - reasoning, planning, parts of speech, movement Parietal lobeorientation, recognition, perception of somatosensory stimuli Occipital lobe- visual processing Temporal lobeperception and recognition of auditory stimuli, memory, speech

Frontal lobe - frontal part n n A 4: Primary motor cortex - controls voluntary movements of specific body parts A 6: Premotor cortex, SMA contributes to the control of movements, planning of complex movements

Frontal lobe - frontal part n n A 8: frontal eye field control of eye movements A 44: Broca´s area responsible for producing language

Homunculus: the "little person" n n n Somatotopic representation of the different body parts The face and hand motor area are the largest Neurons rise to the fibers of the corticospinal tract

Corticospinal tract the main pathway for control of voluntary movement
 and/or behavior diturbance q Primary motor cortex")
Frontal lobe syndromes Impairment of movement (paresis) and/or behavior diturbance q Primary motor cortex q Broca's area aphasia (mono)paresis q q q Contralateral nonfluent speach, agrammatism pt. can understand language but cannot properly form words or produce speech A 8 - frontal eye field deviation of the eyes towards the side of the injury

Frontal lobe - prefrontal part n n modifies the cognitive behavior, personality expression, decision making, social behavior controls emotions, problem solving, memory, judgment, and social and sexual behavior

Prefrontal lobe syndromes changes in personality, behavior diturbance n Disinhibition, emotional lability, sociopathy, sexual n disinhibition, impulsiveness, puerility, pseudopsychopathic disorder Apathy, personality changes, abulia, lack to ability to plan, poor working memory
 - connections from")
Parietal lobe A 1, 2, 3: primary somatosensory area (gyrus postcentralis) - connections from thalamus A 5, A 7: association areas integration of somatosensory, visual, auditory informations

Parietal lobe

Features of parietal lobe lesions n n Somatosensory area - contralateral hemisensory Somatosensory area - loss Association areas - n agnosia -loss of ability to recognize objects, persons, sounds, shapes (while the specific sense is not defective) (tactile, auditory, visual) n apraxia – inability to perform complex movements

Agnosia n n Astereognosia – inability to determine shapes by touch Agraphaesthesia – inability to read numbers or letters drawn on hand, with eyes shut
, the individual has difficulty")
Apraxia n n Apraxia (damage specifically the posterior parietal cortex), the individual has difficulty with the motor planning to perform tasks or movements

Parietal lobe syndromes n Damage to the right parietal lobe can result in Neglect syndrome - neglecting part of the body or space

Temporal lobe n n A 41, 42 primary auditory region A 22 Wernicke‘ s area – comprehension, naming, verbal memory Adjacent areas – involved in high-level auditory processing Hipokampus – essential for memory and learning function

Temporal lobe syndromes n Sensory aphasia- lesion involve the Wernicke s area in language-dominant hemisphere – (comprehensioon, naming, verbal memory) Impairment of memory – lesions affecting the hippokampus n n Possible disturbance of spatial orientation (non-dominant n Irritative phenomena – partial seizures (olfactory, gustatory hallucinations) hemis. )

Occipital lobe n n The occipital lobe - visual processing center The primary visual cortex - Brodmann area 17

Occipital lobe syndrome n n n Homonymous hemianopsia Bilateral lesions - can lead to cortical blindness Occipital lesions can cause visual hallucinations

Aphasia n Broca´s aphasia n n damage to Broca´s area can understand speach cannot produce speach Wernicke´s aphasia n n n damage to Wernicke´s area can produce speach cannot understand speach

n Motor system

Motor system

Basic terms Paresis: decrease in muscular strength, partial paralysis Plegia: loss of muscle strength, complete paralysis monoparesis: one limb affected diparesis: 2 limbs affected triparesis: 3 limbs affected quadriparesis: all limbs affected hemiparesis: limbs of one body side affected (left / right) paraparesis: both lower limbs affected

Central lesion Periferal lesion spastic paresis flaccid paresis Upper motor neuron Lower motor neuron

Upper motor neuron Pyramidal tract the main pathway for control of voluntary movement axons travel in: corticobulbar, corticospinal tract through capsula interna n terminate in: - the cranial nerve nuclei (brainstem) - anterior horn cells (spinal cord) n
 motor neuron, pyramidal tract cause: Central (spastic) paresis disturbance")
Lesion of the upper (central) motor neuron, pyramidal tract cause: Central (spastic) paresis disturbance of movement motor weakness Ø Ø increased reflexes Ø incresaed muscle tone Ø paretic pyramidal signs Ø spastic pyramidal signs

Central paresis power paretic pyramidal signs hyperreflexia irritative pyramidal signs

Typická lokalizace v capsula interna: hemoragie

Peripheral nervous system n n n anterior horn cells of the spinal cord spinal nervs, roots (ventral, dorsal) plexus periferal nerves neuromuscular junction muscle
 motor neuron n n n Peripheral (flaccid) paresis/paralysis weakness is")
Lesion of lower (peripheral) motor neuron n n n Peripheral (flaccid) paresis/paralysis weakness is limited to segmental or focal patterns Hypotonia Hyporefflexia/areflexia Muscle fasciculations Atrophy

Basic different between periferal and central involvement Parametr Periferal lesion Central lesion Myotatic reflexes Muscle tonus - + + - (late, from Fasciculations + - Muscle weakness +(area radic. , nerv. ) + (large areas) Pyramidal irritative signs Muscle atrophy inactivity)

Somatosensory system Sensitivity • anesthesia: loss of sensitivity • hypestesia: decrease of sensitivity • hyperesthesia: increase in sensitivity • paresthesia: sensation of burning, numbness, tingling

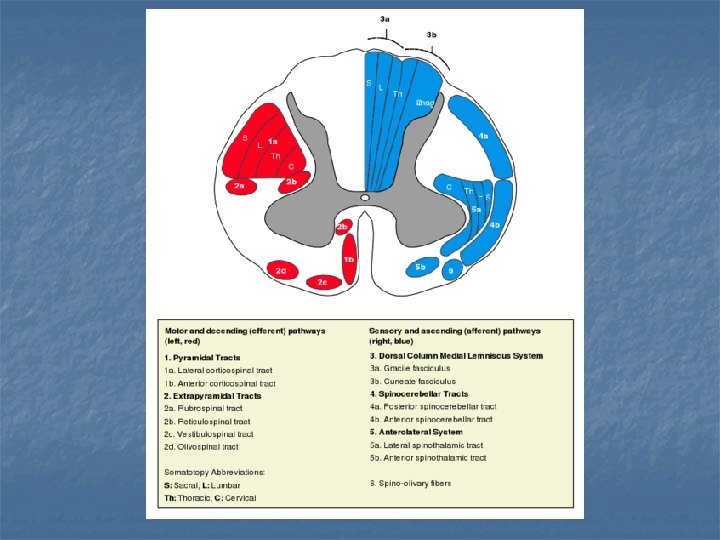
Somatosensitive tracts n Spinothalamic tract: n n pain temperature touch Posterior column n proprioreception (muscle spindles, Golgi tendon organ) pallestesia = vibration sense joint position sense

BG

Basal gangla – major functions Body posture Regulation of muscle tone Coordination of voluntary and automatic movements n n planning and control motor movements, learning/establishing new motor patterns

Extrapyramidal syndromes Damage to these nuclei can cause motor abnormalities Hypokinetic parkinsonism - hypokinesia - rigidity - rest tremor - postural disturbance q Indipendent lecture Hyperkinetic n tremor n chorea n dystonia n myoklonus n tic

Cerebellum regulation of muscle tone balance movement coordination Cerebellar injury results: - in movements that are slow and uncoordinated - patients tend to sway

MRI Imaging
 § q Paleocerebellum (vermis) § q vestibular afferentation -")
Cerebellum q Archicerebellum (pars flokulonodularis) § q Paleocerebellum (vermis) § q vestibular afferentation - balance afferentation from spine cord - posture, gait Neocerebellum (cerebellar hemispheres) § afferentation from cerebral cortex –coordination
 astasia – uncertain standing with wide basis, deviations,")
Paleocerebellar syndrome Axial ataxia (axial disequilibrium) astasia – uncertain standing with wide basis, deviations, falls without side preference abasia – uncertainty when walking, widen basis, deviations, falls without side preference large asynergy – dysfunction of axial muscles coordination titubation – swaying tremor of the head and upper trunk dysarthria

Neocerebellar syndrome Limb ataxia, ipsilateral to affected cerebellar hemisphere hypermetria dysdiadochokinesis intention tremor hypotonia – increased passiveness, excursion range of joints

Vestibular apparatus Balance Regulation of muscle tone Coordination of movements of the head and eyes

Vestibular syndromes Subjective symptoms: vertigo, nausea Objective signs: Nystagmus Balance disorder Tonic deviations of the trunk and limbs
 and fast (compensatory) component.")
Nystagmus Involuntary fast movements of both eyeballs with slow (pathological) and fast (compensatory) component. Nystagmus results from disruption of vestibular system and its neural connections Direction determined by fast component (horizontal, rotational, vertical, combined etc. ) Intensity I. grade: present only when looking in direction of the fast component II. grade: apparent in forward gaze as well III. grade: persisting even when looking on the opposite side

Differentiation between peripheral and central vestibular syndrome Intensity of vertigo Nystagmus Tonic deviation Peripheral Central (harmonic) (dysharmonic) high one direction mild, moderate changes direction Compensation one direction relatively fast Other symptoms auditory variable direction slow, difficult brainstem

Brain stem

Brainstem n A lot of important neural structures located within the brainstem and tracts passing through it. n n n All motor and somatosensory projections pass through brainstem Many nuclei (ncl. of cranial nerves, red nucleus, substantia nigra) Vital regulatory centers (controling cardiovascular, respiratory function) Nuclei of the reticular system Lesions: n n n wide variety of deficits can be produece by lesions The pattern of clinical manifestations depends on localization the level of the lesion - one of the three brainstem segments (midbrain, pons, medulla oblongata)

Crossed brainstem syndromes hemiplegia alternans characterized by the presence of an cranial nerve palsy and contralateral hemiparesis or hemiplegia n n n Mesencephalon (n. III): hemiplegia alternans superior (Weber) Pons (n. VI a VII): hemiplegia alternans media (Millard-Gubler) Oblongata (n. XII): hemiplegia alternans inferior (Déjerine)

hemiplegia alternans

Cranial nerves

Cranial nerves provide motor and sensory innervation for the head and neck damage of the motor neurons results in cranial nerve palsy

Optic nerve, tractus opticus 1. Optic nerve lesion - monocular blindness n 3. Optic chiasm section - bitemporal hemianopsia n 4. Optic tract lesion - contralateral homonymous hemianopsia n

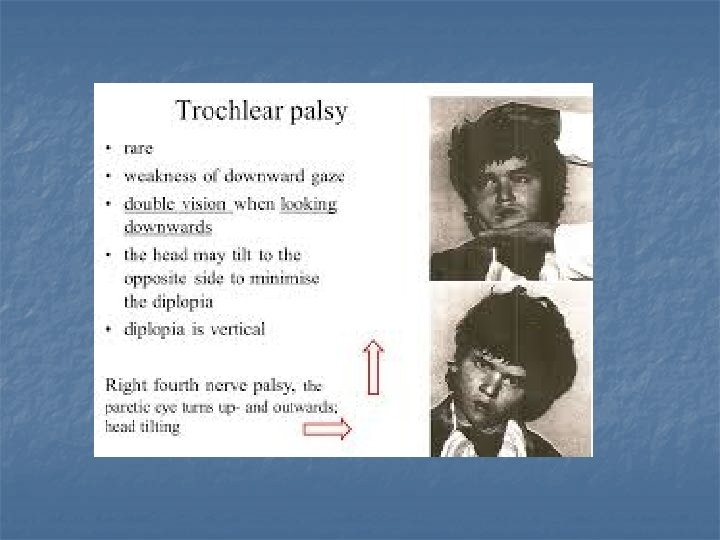
Impaired ocular movement n Lesion of the cranial nerves : n III. oculomotor IV. trochlear VI. abducens n strabismus, double vision (diplopia) n n

Oculomotor palsy

Paréza n. VI.

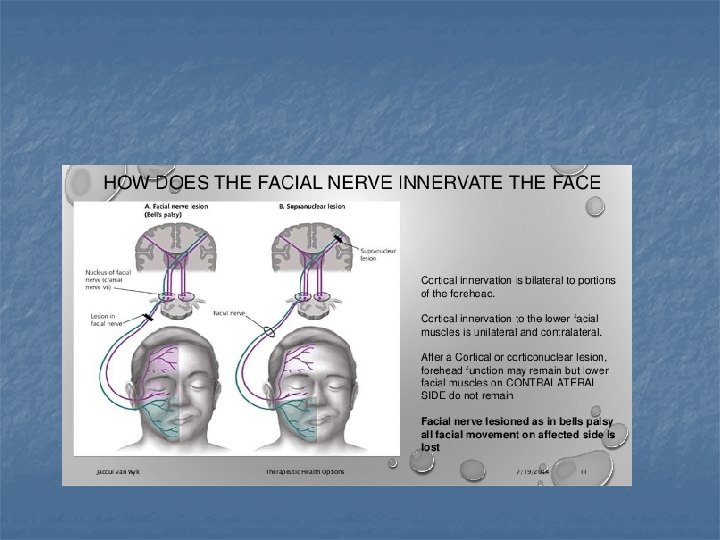
peripheral facial nerve palsy paralysis or weakness of the muscles on one side of the face.
 n motor, sensitive")
Glossopharyngeus, Vagus, Accessorius Hypoglossus nerves (IX, X, XII – bulbar nerves) n motor, sensitive and autonomic inervation
 Lesion of cranial nerves or nuclei of the IX. –")
Bulbar syndrom (bulbar palsy) Lesion of cranial nerves or nuclei of the IX. – XII. in medulla obl. bil. n n n manifests as: dysarthria, dysphagia, aspiration, paresis of soft palate, tongue atrohpy with fasciculations, emetic rfl. is missing Vascular causes: medullary infarction Degenerative diseases: motor neuron disease (amyotrophic lateral sclerosis)

Pseudobulbar syndrome Bilateral lesion of corticobulbar pathway (from cortex – nuclei of nn. IX. – XII. ) dysphagia, dysarthria, dysphonia tongue without atrophy present gag rfl.

Syndrome of pontocerebellar angle Hypacusis, tinnitus, vertigo Peripheral paresis of n. VII. Unilateral extinction of corneal r. Cerebellar syndrome Etiology: Neurinoma of n. VIII. , meningeom
 Neck")
Meningeal syndrome n n n n severe headache nausea and vomiting hypersensitivity (photophobia) Neck stiffness Lassegue sign Brudzinski sign Kernig sign Spine sign

Meningeal signs n Neck stiffness passive flexion of the neck is restricted and painful n Lassegue sign resistance to passive extension of the legs
 n blood (subarachnoid haemorrhage) n")
Meningeal irritation - causes n inflammatory processes (acute meningitis) n blood (subarachnoid haemorrhage) n intracranial hypertension syndrome

Brain herniation n n displacement of a portion of the brain from its normal position can be caused by a number of factors that cause a mass effect and increase intracranial pressure: (injury, stroke, tumor)
 Subfalcial (cingulate) herniation b) uncal herniation c) central, (transtentorial)")
Brain herniation n n a) Subfalcial (cingulate) herniation b) uncal herniation c) central, (transtentorial) herniation d) external herniation e) tonsillar herniation

Spinal cord and syndromes
 the total loss of: n voluntary movement")
Complete spinal lesion Acute stage (spinal shock) the total loss of: n voluntary movement = (paraplegia or quadruplegia) n sensation (of pain, temperature, pressure, proprioception) n autonomic function (bowel and bladder function) n

Complete spinal lesion Motor disorders Peripheral paresis in affected segment Central paresis under the affected segment

Incomplete lesion n n n Lesions affecting only a portion of the spinal cord - cause specific clinical syndromes according to their site some motor and sensory function remains Central Cord Syndrome Anterior Cord Syndrome Posterior Cord Syndrome Brown-Séquard syndrome

Central cord syndrome n n The most common causes: tumor or ischemia Basic characterization: disruption of algic, heat and cold sensitivity within affected segments, with continual spread in caudal direction, usually with sacral preservation. n Syringomyelic dissociation of sensitivity

Anterolateral syndrome n The most common cause: ischemia Basic characterization: n peripheral paresis on the level of affected segments n central paresis caudally from lesion level - results from lesion of descendent pathways n sensation of heat, cold and algic stimuli is affected. Preserved tactile and deep sensory functions.

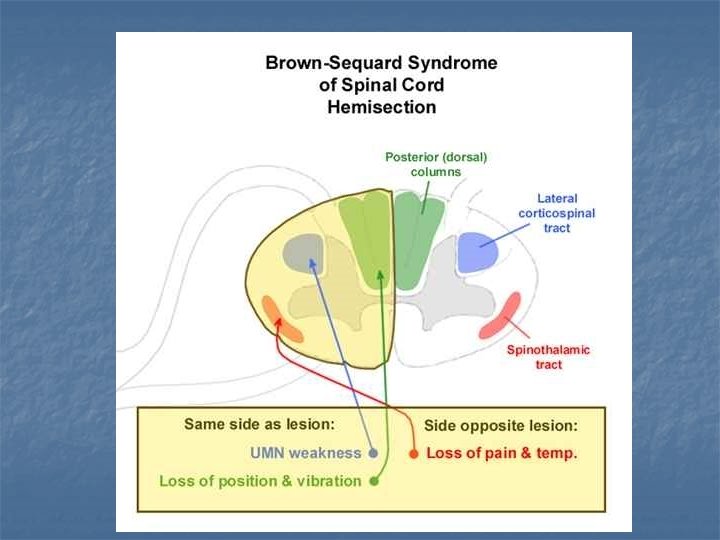
Brown-Sequard´s syndrome n The most common cause: traumatic injury. Basic characterization: n On the homolateral side: n n Peripheral paresis on the level of lesion central paresis below the lesion Sensory disturbance – deep and tactile On the contralateral side: n n No motor disorder Disrupted sensory f. – heat, cold, algic

Posterior column syndrome Lesion of the afferent somatosensory tracts in dorsal portion of the spinal cord (neurosyfilis, metabolic diseasediabetes mellitus) n n impaired proprioreception and position sense lost of balance, ataxia

Peripheral nervous system

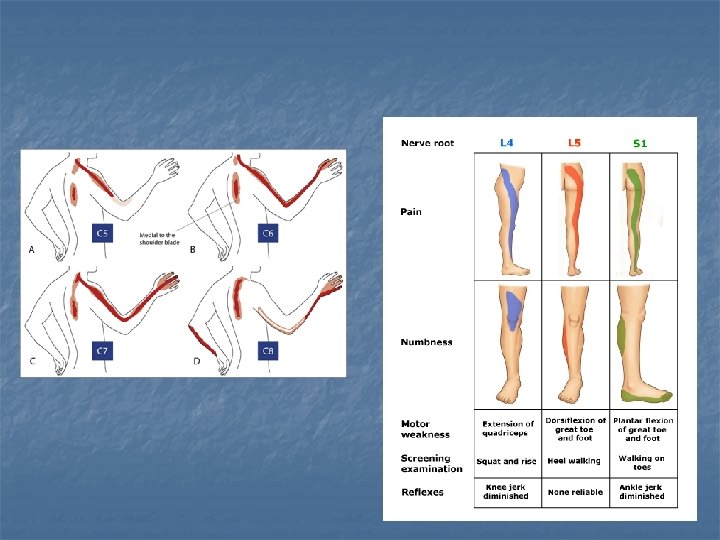
Radicular lesion n n sensory disorder pain in distribution of area radicularis muscle weakness in distribution of area radicularis fasciculation

Disc herniation

Disc herniation n n The majority of spinal disc herniation cases - in lumbar region (95% in L 4 -L 5 or L 5 -S 1) The second most common site - the cervical region (C 5 -C 6, C 6 -C 7)

Spinal disc herniation n n Back pain - into the regions served by affected nerve roots Other symptoms may include: n n n sensory changes (numbness, paresthesia) muscular weakness, paresis affection of reflexes

Cauda equina syndrome n n n compression of multiple lumbosacral nerve roots - usually large midline disc herniation (most often L 4/5 or L 5/S 1) can cause permanent nerve damage the nerve damage can result in loss of bowel and bladder control

Cauda equina syndrome presents: n n n low back pain, asymetry leg pain muscle weakness (hypo)areflexia L 5/S 2 sacral sensory lost dysfunction of urinary and rectal sphinceres

Cauda equina syndrome n n n emergency condition urgent spinal imaging and decompressive surgery is needed to restore neurological functions If the pressure isn't relieved, it can lead to permanent paralysis of the bowels and bladder

Lesion of peripheral nerve muscle weakness in „area nervina“ distribution disorder of sensation in „area nervina“ or „glove-like, sock-like“ distribution (not always present – depends whether the nerve with sensitive component is affected) Pain may be present

Areae nervorum

Areae nervorum

Léze n. radialis Léze n. ulnaris

Carpal tunnel syndrome Compression of the median nerve at the wrist in the carpal tunnel n The main symptoms intermittent numbness n paresthesia n pain of the thumb, index, long and radial half of the ring finger n
 muscular fatigue, weakness depending on preceding physical effort")
Disorders of neuromuscular junction (myasthenic pattern) muscular fatigue, weakness depending on preceding physical effort no sensory deficit no pain normal muscle tone normal reflexes normal muscle mass (-trophy)

Muscle lesion – clinical characterization Muscle weakness (localization depends on distribution of affected muscles, more often proximal) atrophy, hypotrophy, pseudohypertrophy hypotonia reduced (but may be also adequate) reflexes absent disorder of sensation but pain may be present (myositis, rhabdomyolysis) (myopatic climb)
- Slides: 99