Menieres Disease Dr azimi definition spontaneous episodic attacks




")




 • Viral (delayed endolyphativ hydrops after")













 ü Reduce")

 exact mechanism in unclear")













- Slides: 41
Meniere’s Disease Dr. azimi
definition spontaneous, episodic attacks of vertigo; sensorineural hearing loss which usually fluctuates; tinnitus; and often a sensation of aural fullnaess
Epidemiology • • • 17 /100, 000 Japan …… 513/100, 000 Finland More in Whites M=F Peak : 4 th -5 th decade 19 – 24% bilateral 10 -20 % familial (HLA B 8/DR 3)
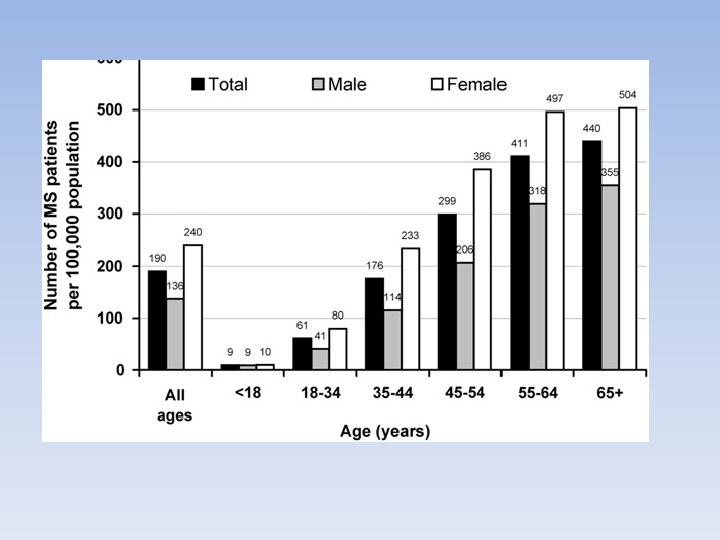
Current epidemiology of Meniere's syndrom 2010 USA • 3. 5 in 100, 000 to 513 in 100, 000 • F /m : 1. 89 /1 • Prevalence of meniere’s syndrome increase with age
Normal membranous labyrinth Dilated membranous labyrinth in Meniere's disease (Hydrops)
Endolymphatic hydrops • • • Meniere’s disease Trauma acute otitis media labyrinthitis, congenital inner ear deformity idiopathic processes
pathophisiology • Ruptures in the membranous labyrinth • leakage of the potassium-rich endolymph into the perilymph • bathing the eighth cranial nerve and lateral sides of the hair cells • depolarize the nerve cells, causing their acute inactivation • typical Meniere's attack • Healing of the membranes • chronic deterioration in inner ear function (repeated exposure to the effects of the potassium)
Pathophysiology
terminology • Triad : vertigo + HL + Tinitus • Triad + known etiology : meniere’s syndrome • Triad + unknown etiology : meniere’s Disease • Triad + known hydrops etiology : secondary meniere’s
Etiology • Immonologic (Abs, HLA, chronic and fluctuating) • Viral (delayed endolyphativ hydrops after deafness) • Ischemy of inner ear or endolymphatic sac (linkage of meniere’s & migrain) • Other related processes (trauma, acute otitis media, labyrinthitis, congenital inner ear deformity, idiopathic processes)
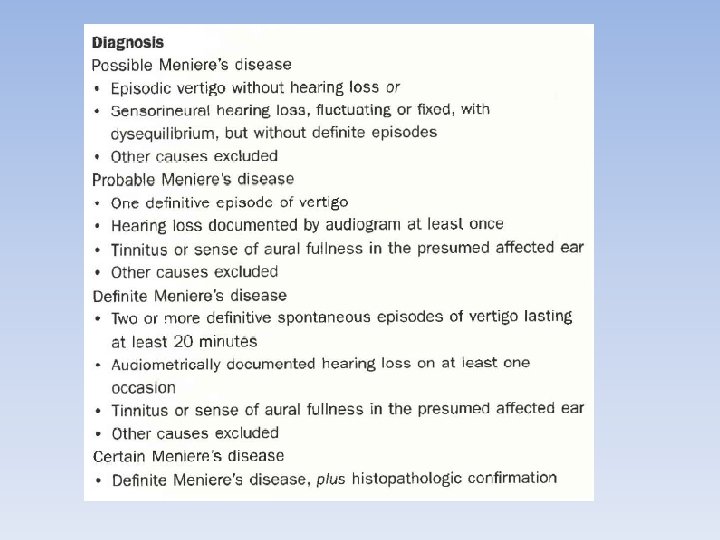
AA 0 -HNS criteria
Clinical presentation • • Vertigo : 96. 2% Tinitus : 91. 1 % Unilateral HL : 87. 7% Sometimes aura : (increased tinitus, HL, aural fullness) Ø Attacks longer than one day : no meiere!!? ?
Vertigo Most distressing complaint Spinning vertigo with horizontal axis Exacerbated with head motion nausea, vomiting. diarrhea, and sweating Between attacks: asymptomatic, periods of dysequilibrium , lightheadedness, and tilt • Horizontal nystagmus (not useful in determi ning the involved ear) • • •
otolithic crises of Tumarkin • Sudden unexplained falls without loss of consciousness or associated vertigo • 2% to 6% of persons with Meniere's disease • The spells are brief with little associated vertigo • tend ro occur in clusters and then spontaneously remit qabrupt change in otolithic input generates an erroneous vertical gravity reference
Hearing Loss • SNHL fluctuating and progressive • sensation of fullness or pressure in the ear • low-frequency fluctuating loss and a coincident nonchanging, high-frequency loss • "peaked" or "tent-like“ at 2 k. Hz • profound deafness in 1 -2 % • Diplacusis (43. 6%) • Recruitment (56%)
Hearing assessment in Menière's disease 2011 spain • 273 ps. • Follow up 1 -30 years. • If surgery was done, data of before the surgery was accessed • Unilateral : low frequency, even in very advanced stage. was accentuated at 5 and 15 years from onset • Bilateral : slightly more severe. a flatter audiometric curve than in unilateral cases v. The audiometric curve configuration may be an indicator of future bilateral disease.
tinitus • Nonpulsatile • Whistling or roaring • continuous or intermittent • Tinnitus often: ü begins, gets louder, or changes pitch as an attack approaches
Clinical characteristics of tinnitus in Ménière's diseas 2011 • 88 ps were analysed • Avarage time of the disease: 15. 4 • 46% of moderate intensity ( 5/10 analogue-visual scale) & low frequency • unfavourable prognostic factors for decrease in quality of life : history of depression & young age. v patients do not perceive tinnitus as a problem that produces serious impairment in their quality of life
Electronystagmography • recordings of eye movements after caloric and rotational stimulation • often can localize the involved ear. • significant caloric response reduction: 48 -73. 5% • Complete absence of caloric response : 6 -11%
Electrocochleography • SP : is larger and more negative • increase in SP/AP : reduce the intertest variability, a more linear response • Increase in SP/AP : 62% of meniere & 21% in normal controls
Dehydrating Agents • urea, glycerol, furosemide • Improvement has been measured with audiometrics, reduction in SP negativity (as recorded with electrocochleography), or a change in the gain of the vestibula-ocular response to rotational stimulation Ø Sensivity : variable. 60%
Vestibular Evoked Myopotentials • Click stapes movement saccule stimulation vestibular nocleus SCM relaxation • Saccule : 2 nd most common affected site in hydrops • Affected ear: elevated VEMP thresholds with flattened tuning
Treatment
Dietary Modification and Diuretics • Salt restriction + diuretics (best initial therapy) ü Reduce endolymph volume ü Not confirmed • Acetazolamide : ü localization of carbonic anhydrase to the dark cells and the stria vascularis ü Not proved
Diuretics in Meniere disease: A therapy or a potential cause of harm? 2011 italy • A common treatment ü to decrease volume and pressure in the endolymphatic partition of the labyrinth • possibility of an adverse effect: ü Abrupt lowerng of BP …exaggerated vasomotor response …. local ischemia…. permanent damage. ü terminal vascular supply…hemodynamic imblaenc: loss of perfusion
vasodilators • At the basis of sterial ischemia • (2010) exact mechanism in unclear • Betahistine: ü Oral histamine preparation ü Proved to be effective in vertigo ü (cochrane 2010) although individual trials had positive results, larg randomised trials is needed (2010) No effect on hearing loss
Symptomatic treatment • • • Anti vertigo Anti nausea Sedatives Antidepressants Psychiatric treatment
Local Overpressure Therapy • Increase in middle ear pressure: relief of meniere’s symptoms • Meniett device: ü FDA approved ü First; VT insertion ü Pressure : 20 cm H 2 O for 5 min periods ü Effective in first 3 months
Long-term effects of the Meniett device in Japanese patients with Meniere's disease and delayed endolymphatic hydrops reported by the Middle Ear Pressure Treatment Research Group of Japan. 2011 • 29 ears of 28 meniere ps & 5 ears of 5 ps with DEH • All , failed medical treatment • 57% of MD & 100% of DEH remained entirely free from vertigo spells • 32% of MD : significant decrease in the frequency of vertigo spells • 25 ears : stable hearing levels • 4 ears : significant hearing improvement. v. No complications
Intratympanic Injection • • • Gentamycin: Vestibulotoxicity more than cochleotoxicity Elimination of vertigo: 90% , 83% SNHL : 10%, 3% Single dose is better (booster dose if needed) The risk of hearing loss with gentamicin using many current protocols is similar to that with the natural history of Meniere's disease
Intratympanic gentamicin in Ménière's disease: our experience. 2011 spain • Longitudinal, prospective, descriptive • Complete vertigo control : 65. 6% • complete or substantial control : 84. 37% • 13 ps (18. 3%) suffered significant hearing loss. va good alternative to more aggressive techniques for the treatment of Ménière's disease which does not respond to medical treatment.
Intratympanic Injection • Dexametasone: • Control of vertigo without effect on HL or tinitus • Intarctable vertigo but functional hearing • Success : 83% • Repeated dose every 3 month • Dose : 2 -24 mg/ml
Intratympanic steroids for Ménière's disease or syndrome. 2011 UK • Clinical trial • A single trial containing 22 patients, with a low risk of bias was included. • daily injections of dexamethasone solution 4 mg/ml for five consecutive days • After 24 m. compared placebo with intratympanic dexamethasone • improvement in vertigo (90% vs 42%) • mean vertigo subjective improvement (90% vs 57%) v clinically significant. No complications. v statistically and clinically significant improvement of the frequency and severity of vertigo
Endolymphatic Sac Surgery • Simple decompression, • wide decompression that includes the sigmoid sinus, • cannulating the endolymphatic duct • endolymphatic drainage to the subarchnoid space, • drainage to the mastoid • removal of the extraosseous portion of the sac
Nerve Section • Approaches: retrosygmoid, suboccipital, middle fossa, retrolabyrinthine • 85 -95% relief of vertigo • 80 -90% hearing perservation v. HL less than gentamycin injection
10 -year review of endolymphatic sac surgery for intractable meniere disease 2011 London • 1998 – 2007 • 33 ears. • Mean age : 49 m/f : 63%-37% • Successful vertigo control : 64. 5% (class a-b) • Hearing : • improved 14. 8%, the same 51. 9%, worsend 33. 3% • 3 p. (10%) had profound SNHL • 80% of ps, had improved quality of life scales
Labyrinthectomy • No functional hearing with resistant vertigo • Best control of vertigo • But should be the last choice
Meniere's disease and the use of proton pump inhibitors 2010 italy • 2001 – 2006 • 42 ps • 18 patients had used PPI for various reasons for at least 12 consecutive months, whilst 24 patients had never been prescribed them • f/u 29 month • Most of MD patients (72%) using PPI suffered less than one episode of menieric crisis/year. On the other hand patients who had never used a PPI, experienced considerably more episodes only 16. 7% having less than one crisis per year. This difference was statistically significant (p<0, 001). v strongly suggest a possible role for proton pumps in the pathogenesis of MD