Thoracic Ultrasound for Pulmonologists Interventional Pulmonology Course The







 • Hands-on lab sessions (PM)")





 are visible, reminiscent of a rocket")





 − 18% PTx")
 – Feissel ICM 2004 •")
 • To image and access beyond the mucosa of the GI")











 • Radial probe (not real-time): for peripheral lesion • Linear probe")






 • Sputum cytology atypia but normal white")
 • For patients")


 transbronchial lung biopsy Wahidi, M. M.")



 • A high voltage spark is delivered at the tip")
")




 Trial Cox G et al. NEJM 2007; 356: 33")











 is a")





- Slides: 85
Thoracic Ultrasound for Pulmonologists Interventional Pulmonology Course - The 24 th Year Lahey Clinic, Burlington, Boston, USA Mar 27 – 31, 2007 Highlights by Dr Arthur CW Lau
Introduction • Didactic lectures (AM) • Hands-on lab sessions (PM)
Topics • • • Pleura and pleural space, vessels − Thoracic ultrasound in critical care: vessel, transthoracic − Pleuroscopy – rigid thorascopy and flexi-rigid pleuroscopy − Use of pleural catheter Brochoscopy (diagnostic and therapeutic) − Endobronchial USG (EBUS) − Improving TBNA yield − Autofluorescence bronchoscopy − Navigational bronchoscopy − Endobronchial electrosurgery and Argon Plasma Coagulation − Endobronchial cryotherapy − Laser bronchoscopy − Bronchial thermoplasty Airways − Percutaneous tracheostomy − Airway Stents: − Balloons and tubes for airways and pleura − Laryngo-tracheal stenosis − Tracheomalacia and dynamic airway collapse − Endobronchial valves Medical Grand Round – Lung transplantation Billing and coding for Interventional procedures
Harvard University
Pleura and pleural space Ultrasound
Thoracic ultrasound in critical care • Transthoracic −curvilinear • Vessel −linear
• Left: B-mode − horizontal artifacts, the pleural line, called for convenience “ultrasound A lines” (Fig. 1 left) − vertical comet-tail artifacts, well-defined, arising from the pleural line, synchronous with lung sliding, spreading out without fading to the edge of the screen • Right: M-mode − objectifies lung sliding − “seashore sign”
• Four or five comet-tail artifacts (“Lung-rockets”) are visible, reminiscent of a rocket at lift-off. • an ultrasound sign of interstitial syndrome: “Lung rockets” reveal structures which are not directly visible but which have an high acoustic impedance gradient, e. g. thickened interlobular septa.
• Pleural effusion • pleural line superficially, visceral pleura deeper. • The deep border must move sinusoidally from bottom to top, synchronized with respiration (“sinusoid sign”), specific to pleural effusion
• Left B-mode: Abolition of lung sliding (which cannot be visualized in this frozen image) associated with exclusive horizontal artifacts arising from the pleural line. Absence of sliding lung and absence of “comet-tail” artefacts = 96. 5% specific for PTx Right M-mode: Below the pleural line, the normal granulous pattern is replaced by a horizontal pattern, objectifying the absolute absence of lung sliding (“stratosphere sign”)- not specific to pneumothorax.
• The “lung point”: Association of absent lung sliding with “A lines” • M-mode: This sudden replacement of the physiologic granulous pattern by a horizontal pattern, at a precise location of the chest wall, is specific to pneumothorax.
• Alveolar consolidation: Hyperechoic punctiform opacities show the air bronchograms
Vascular Thrombus in RIJV Needle, guidewire, catheter visualized
Why US? • Review of 342 thoracentesis (Raplopoulos, AJR 156: 917) − 18% PTx rate without US − 3% PTx rate with • ICU/vented patients (Kohan ARRD 1986) − Significantly changes treatment in 41%
Vessels • IVC (distensibility index >12% predicted fluid responsiveness) – Feissel ICM 2004 • Echocardiography − Changes Mx in 34 – 64% • USG-guided central line placement − Position, thrombus
Endoscopic ultrasound (EUS) • To image and access beyond the mucosa of the GI tract for dx and staging • First described in Japan in 1988 • Use radial or linear probes • EUS with FNA for lung cancer staging: − Left lobe of liver − Left adrenal − Stations (2, 4), 5, 7, 8, 9
Use of pleural catheter The Pleurx® catheter: manage chronic pleural effusion in the home setting
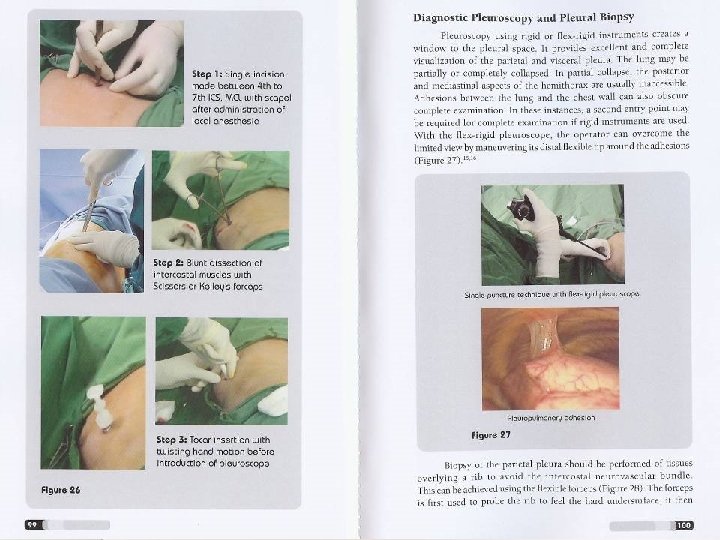
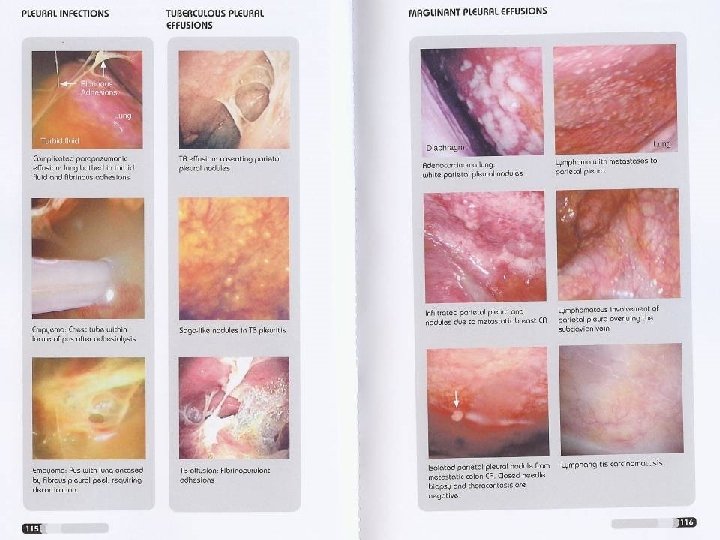
Pleuroscopy – rigid thorascopy and flexi-rigid pleuroscopy • Rigid thoracoscope: in OR • Flexi-rigid pleuroscopy: can be done in the bronchoscopy suite under conscious sedation
Nodules seen on the diaphragmatic pleura during medical pleuroscopy in a patient who presented with a right pleural effusion Wahidi, M. M. et al. Chest 2007; 131: 261 -274
Bronchoscopy Diagnostic and therapeutic
Regional Lymph Node Classification for Lung Cancer Staging Mountain and Dresler 1997
Areas accessible by technique 2 TBNA EUS/FNA Mediastin oscopy Thoracosc opy 4 5 6 7 ● ● ● 3 ● ● ● ● 8 9 ● ●
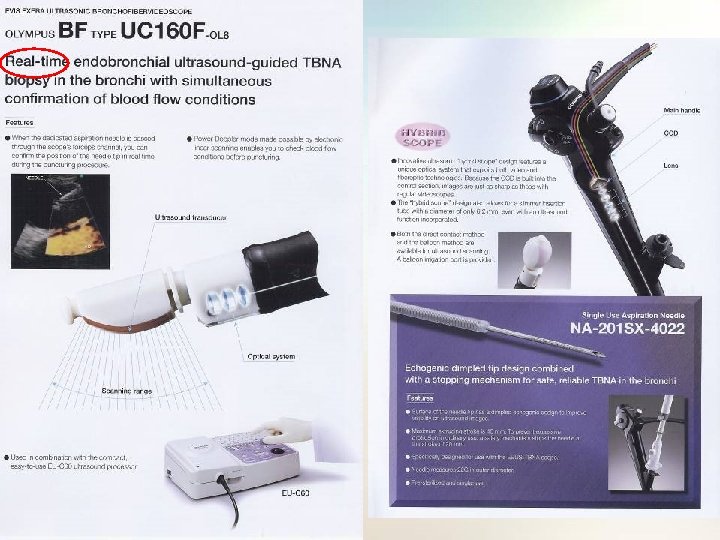
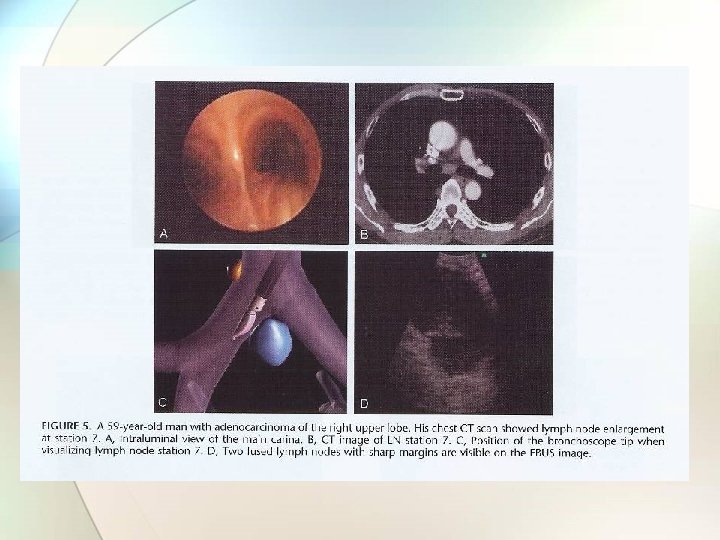
Endobronchial ultrasound (EBUS) • Radial probe (not real-time): for peripheral lesion • Linear probe (real-time): for central lesion − Stations 2, 4, 5, 6, 7 • + doppler function
Radial probe
Image of a transbronchial needle puncture of a small lymph node in the 10 R position Wahidi, M. M. et al. Chest 2007; 131: 261 -274
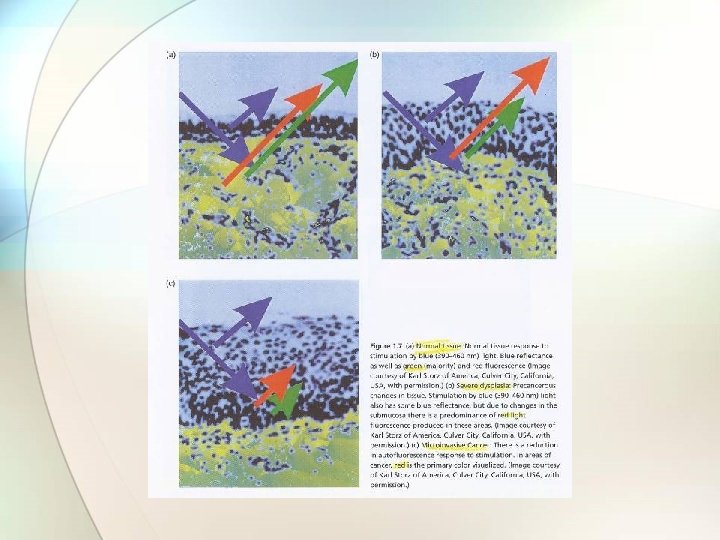
Autofluorescence systems
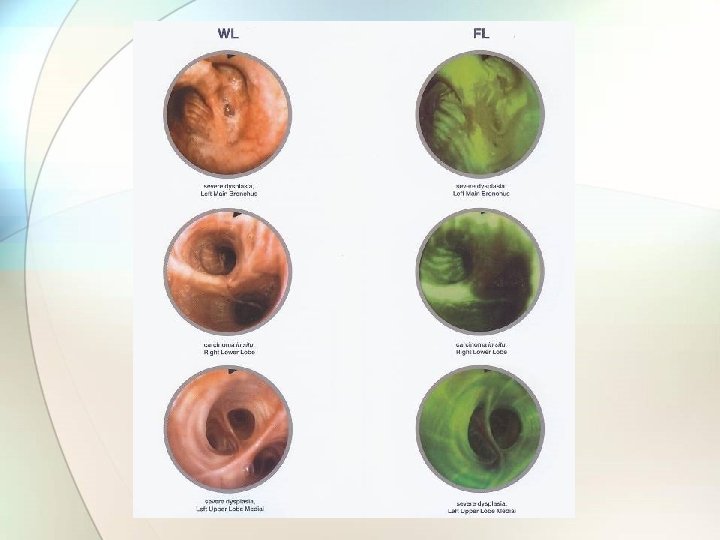
Autofluorescence bronchoscopy
A patient with a small endobronchial carcinoma in situ Wahidi, M. M. et al. Chest 2007; 131: 261 -274
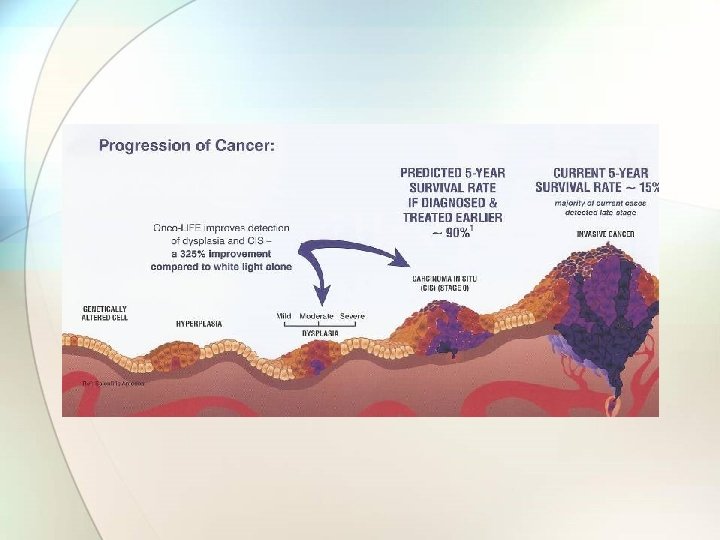
Local indications for autofluorescence bronchoscopy examination (QMH) • Sputum cytology atypia but normal white light bronchoscopy and non-localizing radiological examination i. e. normal CXR/CT • Operable lung cancer patients but synchronous lung cancer suspected. • Preoperative assessment of lung cancer to delineate endobronchial extension.
Follow up plan for patients who had autofluorescence bronchoscopy performed (QMH) • For patients confirmed to have invasive lung cancer, they will be staged and managed according to the current recommendations. • For patients with intraepithelial neoplasm, i. e. severe dysplasia or carcinoma in situ, local treatment will be offered (e. g. cryotherapy) unless refused by patients. • For patients with moderate dysplasia, they would be followed up with autofluorescence bronchoscopy at 6 monthly interval till histology reported as mild dysplasia or less • For remaining patients who had non-diagnostic autofluorescence bronchoscopy, they should have CT thorax if not done yet to look for peripheral lesions. If still non-diagnostic, these patients should be followed up regularly at referring unit and repeat sputum cytology at 6 monthly intervals. They should be referred for repeating autofluorescence bronchoscopy examination if sputum atypia persisted.
Harvard Museum of Natural History
Navigational bronchoscopy
Typical images of an electromagnetically guided (super. Dimension) transbronchial lung biopsy Wahidi, M. M. et al. Chest 2007; 131: 261 -274
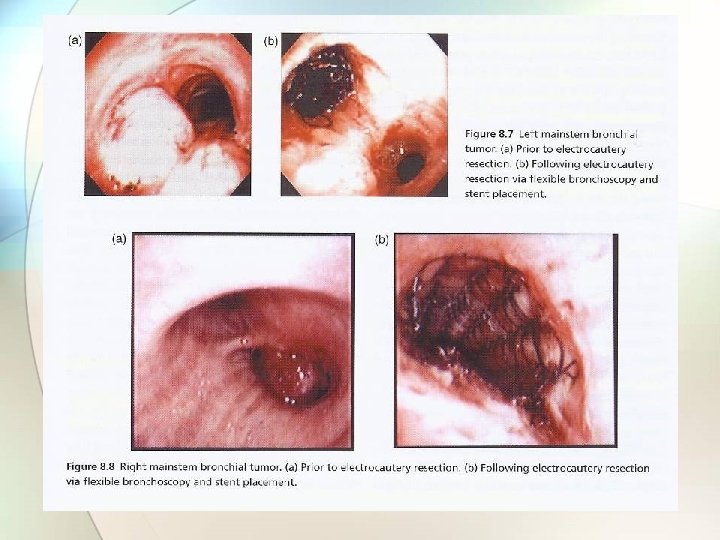
Electrosurgery • Electrocautery with • Argon Plasma Coagulation • Nd: YAG Laser • Cryotherapy
Electrocautery via the flexible or rigid bronchoscope Relies on direct tissue contact Can be done through rigid or flexible scopes.
Argon plasma coagulation (APC) • A high voltage spark is delivered at the tip of the probe, which ionizes the argon gas as it is sprayed from the probe tip in the direction of the target tissue. • via the flexible or rigid bronchoscope • Non-contact
Granulation tissue is visible at the proximal end of a tracheal stent (top left) Wahidi, M. M. et al. Chest 2007; 131: 261 -274
Nd: YAG laser • via the flexible or rigid bronchoscope • Non-tissue contact • Low tissue absorption • High coagulation • Low cutting effect • Perforation, airway fire, air embolism
Cryotherapay • via the flexible or rigid bronchoscope • Tissue contact • safe, with no danger of bronchial wall perforation • delayed results and the requirement for multiple endoscopies to remove debris or to retreat. (A) Cryotherapy can be applied to tissue using either the probe tip or side. (B) Reapplication to the same area after thawing allows a deeper freeze and tissue destruction.
Chest. 2007; 131: 261 -274
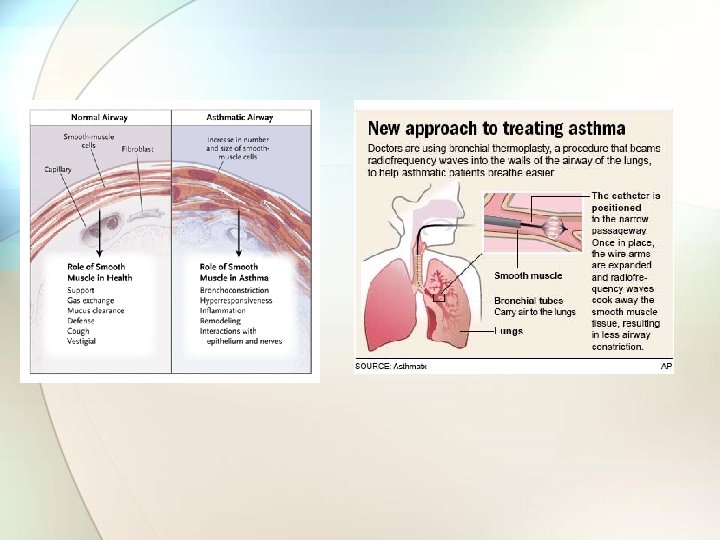
Bronchial thermoplasty The Alair® System - which is manufactured by Asthmatx, Inc. - consists of a single-use device and a controller that delivers thermal energy to the bronchial wall during an outpatient bronchoscopic procedure known as Bronchial Thermoplasty™.
The Asthma Intervention Research (AIR) Trial Cox G et al. NEJM 2007; 356: 33 - 43
Summary • • Bronchial thermoplasty to moderate to severe asthma 55 BT vs 54 control The mean rate of mild exacerbations, as compared with baseline, was reduced in the bronchial-thermoplasty group but was unchanged in the control group (change in frequency per subject per week, – 0. 16± 0. 37 vs. 0. 04± 0. 29; P=0. 005). At 12 months, there were significantly greater improvements in the bronchialthermoplasty group than in the control group in the − − − • morning peak expiratory flow (39. 3± 48. 7 vs. 8. 5± 44. 2 liters per minute) scores on the AQLQ (1. 3± 1. 0 vs. 0. 6± 1. 1) ACQ (reduction, 1. 2± 1. 0 vs. 0. 5± 1. 0) the percentage of symptom-free days (40. 6± 39. 7 vs. 17. 0± 37. 9), and symptom scores (reduction, 1. 9± 2. 1 vs. 0. 7± 2. 5) while fewer puffs of rescue medication were required. Adverse events immediately after treatment were more common in the bronchialthermoplasty group than in the control group but were similar during the period from 6 weeks to 12 months after treatment.
AIR 2 Trial • Subjects: severe asthma • Aims to recruit 280 patients by March 31 2007
Airways
Percutaneous tracheostomy • Human cadaver available for practice
Airway stents • Silicone stents − − Cheaper easily removed higher incidence of migration require rigid bronchoscopy for placement • Metallic stents − can be placed via flexible bronchoscopy or rigid bronchoscopy, with or without fluoroscopy. − Ultraflex® stent
Top, A: a proximal view of a silicone stent within the right mainstem bronchus Wahidi, M. M. et al. Chest 2007; 131: 261 -274
Top, A: squamous cell carcinoma with near complete occlusion of the left mainstem bronchus Wahidi, M. M. et al. Chest 2007; 131: 261 -274
Stent Type Manufacturer Construction Dumon Novatech Molded silicon rubber Hood Corp. Molded silicon rubber Wallstent Boston Scientific Woven cobalt/chrome alloy monofilament coated with silicone Polyflex Rush Inc. Ultraflex Boston Scientific Dynamic Rush Inc. Polyester mesh covered with silicone Single strand woven nitilol With/without silicone coating Silicone with anterolateal steel struts
Bronchoscopic lung volume reduction • Placement of one-way endobronchial valves in segmental and/or sub-segmental airways • General inclusion and exclusion criteria (extrapolated from NETT) • Inclusion: severe, UL emphysema • Exclusion: diffuse emphysema, FEV 1<20%, DLCO<20%
Endobronchial valves 1. Emphasys Med Inc: − Emphasys Zephyr™ Endobronchial Valve* (EBV) is a one-way, silicone valve supported by a Nitinol retainer − Endobronchial Valve for Emphysema Palliatio. N Trial (VENT) 2. Spiration Inc: − IBV valve − IBV Valve Trial An older model
Balloon bronchoplasty Ballon bronchoplasty can be performed with a flexible or a rigid bronchoscope ● Serial bougie dilatation can only be done by rigid Mayse, M. L. et al. Chest bronchoscope ● 2004; 126: 634 -637
Microdebrider
Other topics • Medical Grand Round: Lung transplantation • Billing and coding for Interventional procedures • Improving yield of TBNA • Laryngotracheal stenosis • Tracheomalacia and excessive dynamic collapse • Chest tube insertion and management
Boston downtown
Thank you.