THORACIC AND NECK TRAUMA Epidemiology Thoracic and neck





















 – Shotgun • Injury severity")


















































 • Neurologic deficit • Cranial nerve deficits •")






 • Jugular veins • Zone of injury •")













- Slides: 94
THORACIC AND NECK TRAUMA
Epidemiology • Thoracic and neck injuries are the 2 nd leading cause of death due to trauma • The mortality rate of neck injuries has declined • Increase in violence has had an impact on the pattern of injuries to the chest and neck
Mechanisms of Injury and Biomechanics • • Motor vehicle crashes Falls Crush Injuries Assaults Firearms Stabbings Motor vehicle versus pedestrian
Mechanisms of Injury and Biomechanics • Acceleration forces • Deceleration forces – Thoracic aorta – Relative fixed attachment – Ligamentum arteriosum • Motor vehicle crashes account for two-thirds of all chest traumarelated deaths
Concurrent Injuries • Head • Extremity • Abdomen 5
Introduction to Thoracic Injury • Vital Structures – Heart, Great Vessels, Esophagus, Tracheobronchial Tree, & Lungs • Abdominal injuries are common with chest trauma.
Pathophysiology • Ineffective ventilation may occur from the loss of integrity of anatomical structures as well as compromise to the normal physiologic process of respiration. 7 Coronal CT image—crush injury to chest with left pneumothorax, air and blood in pleural space, and subcutaneous emphysema (blue arrow) in left chest wall
Pathophysiology • Some causes of ineffective ventilation include: • Tears or lacerations to tracheobronchial tree • Rib or sternal fractures • Pain • Lung contusion or puncture • Penetrating injury of the chest wall
Pathophysiology • Ineffective circulation can occur from injury to the heart or thoracic great vessels causing internal and external hemorrhage which can lead to hypovolemia and shock. • Direct trauma to the heart may result in a reduced cardiac output from decreased myocardial contractility. 9
• Air or blood in the thoracic cavity will increase the intrapleural pressure causing obstruction of venous return. • Pericardial tamponade may result in decreased cardiac output.
Type of Impact and Associated Injury • Frontal impact: Anterior flail chest, blunt cardiac injury • Side impact: Lateral flail chest, pneumothorax • Motor vehicle versus pedestrian: Thoracic and abdominal injuries
Pathophysiology of Thoracic Trauma • Deceleration – Body in motion strikes a fixed object – Blunt trauma to chest wall – Internal structures continue in motion » Ligamentum Arteriosum shears aorta
Ruptured Aorta Blunt aortic Injury Widened Mediatinum
Types of Injuries • Blunt trauma: 70% – Most common cause is motor vehicle crashes • Penetrating trauma: 30% – Firearms – Stabbings
Pathophysiology of Thoracic Trauma Blunt Trauma – Results from kinetic energy forces – Subdivision Mechanisms • Blast – Pressure wave causes tissue disruption – Tear blood vessels & disrupt alveolar tissue – Disruption of tracheobronchial tree – Traumatic diaphragm rupture • Crush (Compression) – Body is compressed between an object and a hard surface – Direct injury of chest wall and internal structures
Blunt Cardiac Injury • Formerly called cardiac contusion or cardiac concussion • Suspect following an associated mechanism of injury (motor vehicle crash) or in those patients with poor cardiovascular response to injury 16
Blunt Cardiac Injury Signs and Symptoms • ECG abnormalities • Chest pain • Chest wall ecchymosis 17
Pathophysiology of Thoracic Trauma Chest Wall Injuries • Contusion – Most Common result of blunt injury – Signs & Symptoms • • • Erythema Ecchymosis DYSPNEA PAIN on breathing Limited breath sounds HYPOVENTILATION – BIGGEST CONCERN = “HURTS TO BREATHE” • Crepitus • Paradoxical chest wall motion
Pulmonary Contusion • Occurs as a result of direct impact • Blood leaks into lung • Respiratory insufficiency develops over time 19 Copyright © 2007 ENA
Pulmonary Contusion Signs and Symptoms • Dyspnea • Ineffective cough • Hemoptysis • Hypoxia • Chest pain • Chest wall contusion or abrasions 20 Copyright © 2007 ENA
Pathophysiology of Thoracic Trauma • Penetrating Trauma – Low Energy • Arrows, knives, handguns • Injury caused by direct contact and cavitation – High Energy • Military, hunting rifles & high powered hand guns • Extensive injury due to high pressure cavitation
Pathophysiology of Thoracic Trauma • Penetrating Injuries (cont. ) – Shotgun • Injury severity based upon the distance between the victim and shotgun & caliber of shot • Type I: >7 meters from the weapon – Soft tissue injury • Type II: 3 -7 meters from weapon – Penetration into deep fascia and some internal organs • Type III: <3 meters from weapon – Massive tissue destruction
Injuries Associated with Penetrating Thoracic Trauma • Closed pneumothorax • Open pneumothorax (including sucking chest wound) • Tension pneumothorax • Pneumomediastinum • Hemothorax • Hemopneumothorax • Laceration of vascular structures • • Tracheobronchial tree lacerations Esophageal lacerations Penetrating cardiac injuries Pericardial tamponade Spinal cord injuries Diaphragm trauma Intra-abdominal penetration with associated organ injury
Pathophysiology of Thoracic Trauma – Age Factors • Pediatric Thorax: More cartilage = Absorbs forces • Geriatric Thorax: Calcification & osteoporosis = More fractures
Rib and Sternal Fractures • Rib fractures – Most common blunt chest injury – Lung injury most significant • Most common sternal fracture site: Angle of Louis 25
Rib and Sternal Fractures Signs and Symptoms • Dyspnea • Localized pain • • Assumes position to splint chest wall Chest wall ecchymosis Sternal contusion Bony crepitus or deformity 26
Management of the Chest Injury Patient • Rib Fractures – Consider analgesics for pain and to improve chest excursion • Versed • Morphine Sulfate – CONTRAINDICATION • Nitrous Oxide – May migrate into pleural or mediastinal space and worsen condition
Flail Chest • Flail chest is defined as a fracture of two or more sites on two or more adjacent ribs or when rib fractures produce a free-floating sternum causing the unsupported chest wall or flail segment to move paradoxically from the rest of the chest wall during inspiration and expiration. • May not be clinically evident in first several hours 29
Pathophysiology of Thoracic Trauma Chest Wall Injuries • Flail Chest – Segment of the chest that becomes free to move with the pressure changes of respiration – Three or more adjacent rib fracture in two or more places – Serious chest wall injury with underlying pulmonary injury • Reduces volume of respiration • Adds to increased mortality – Paradoxical flail segment movement – Positive pressure ventilation can restore tidal volume
• A flail chest may be associated with the following: • Ineffective ventilation • Pulmonary contusion • Lacerated parenchyma • Flail chest may not be clinically evident in the first several hours because of muscle spasms that cause splinting.
Flail Chest Signs and Symptoms • Dyspnea • Chest wall pain • Paradoxical chest wall movement: The flail segment moves in during inspiration and out during expiration http: //www. youtube. com/watch? v=e 0 VNBDbr 67 U Flail Chest
Pneumothorax • Injury to the lung leads to accumulation of air in the pleural space with a subsequent loss of negative intrapleural pressure • Open pneumothorax: Wound in chest wall
Pneumothorax • Accumulation of air in pleural space with loss of negative intrapleural pressure • Open pneumothorax: Wound in chest wall 34 Copyright © 2007 ENA
Pathophysiology of Thoracic Trauma Pulmonary Injuries • Open Pneumothorax – Free passage of air between atmosphere and pleural space – Air replaces lung tissue – Mediastinum shifts to uninjured side – Air will be drawn through wound if wound is 2/3 diameter of the trachea or larger – Signs & Symptoms • • • Penetrating chest trauma Sucking chest wound Frothy blood at wound site Severe Dyspnea Hypovolemia
Pathophysiology of Thoracic Trauma Pulmonary Injuries • Simple Pneumothorax – AKA: Closed Pneumothorax • Progresses into Tension Pneumothorax – Occurs when lung tissue is disrupted and air leaks into the pleural space – Progressive Pathology • • Air accumulates in pleural space Lung collapses Alveoli collapse (atelectasis) Reduced oxygen and carbon dioxide exchange • Ventilation/Perfusion Mismatch – Increased ventilation but no alveolar perfusion – Reduced respiratory efficiency results in HYPOXIA – Typical MOI: “Paper Bag Syndrome”
Pneumothorax Signs and Symptoms • Dyspnea, tachypnea • Tachycardia • Hyperresonance on injured side • Decreased or absent breath sounds on the injured side • Chest pain • Open, sucking wound on inspiration (open pneumothorax)
Pneumomediastinum • Gas / air forming in the mediastinum » From infection » From penetrating wound
Tension Pneumothorax • Life-threatening injury • Air enters pleural space on inspiration but the air cannot escape on expiration • Increased intrathoracic pressure collapses the injured lung and causes a mediastinal shift
Pathophysiology of Thoracic Trauma Pulmonary Injuries • Tension Pneumothorax – Buildup of air under pressure in the thorax. – Excessive pressure reduces effectiveness of respiration – Air is unable to escape from inside the pleural space – Progression of Simple or Open Pneumothorax
Tension Pneumothorax Signs and Symptoms • • • Severe respiratory distress Hypotension Distended neck veins Tracheal deviation (late sign) Cyanosis (late sign) 41 left-sided tension pneumothorax with mediastinal shift
Planning and Implementation • Ensure patent airway • Administer oxygen • Cover open chest wounds with a sterile, nonporous dressing and tape on three sides • IMMEDIATELY prepare for needle thoracentesis 42
Planning and Implementation Prepare for: • Chest tube insertion • Autotransfusion • Aggressive ventilatory support • Surgical intervention • Emergency thoracotomy 43
Management of the Chest Injury Patient • Tension Pneumothorax – Confirmation • Auscultaton & Percussion – Pleural Decompression • 2 nd intercostal space in mid-clavicular line – TOP OF RIB • Consider multiple decompression sites if patient remains symptomatic • Large over the needle catheter: 14 ga • Create a one-way-valve: Glove tip or Heimlich valve
Hemothorax • Accumulation of blood in the pleural space • Massive hemothorax: Rapid accumulation of 1, 500 ml or more of blood 45
Pathophysiology of Thoracic Trauma Pulmonary Injuries • Hemothorax – Accumulation of blood in the pleural space – Serious hemorrhage may accumulate 1, 500 m. L of blood • Mortality rate of 75% • Each side of thorax may hold up to 3, 000 m. L – Blood loss in thorax causes a decrease in tidal volume • Ventilation/Perfusion Mismatch & Shock – Typically accompanies pneumothorax • Hemopneumothorax
Hemothorax Signs and Symptoms • Dyspnea, tachypnea • Tachycardia • Diaphoresis • Chest pain • Hypotension & Signs of shock • Decreased breath sounds on the injured side • Dullness to percussion on the injured side 47
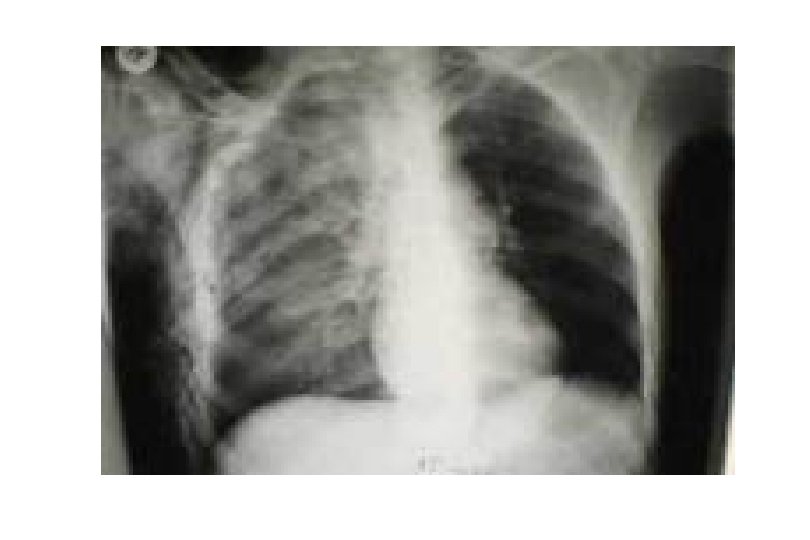
Aortic rupture (a tear in the aorta, which is the major artery coming from the heart) can be seen on a chest x-ray. In this case, it was caused by a traumatic perforation of the thoracic aorta. This is how the x-ray appears when the chest is full of blood (right-sided hemothorax) seen here as cloudiness on the left side of the picture.
Management of the Chest Injury Patient • Hemothorax – High flow O 2 – 2 large bore IV’s • Maintain SBP of 90 -100 • EVALUATE BREATH SOUNDS for fluid overload • Myocardial Contusion – Monitor ECG • Alert for dysrhythmias – IV if antidysrhythmics are needed
Management of the Chest Injury Patient • Open Pneumothorax – High flow O 2 – Cover site with sterile occlusive dressing taped on three sides – Progressive airway management if indicated
Pulmonary Contusion • Occurs as a result of direct impact, deceleration, high velocity bullet wounds • Respiratory insufficiency develops over time
Pathophysiology of Thoracic Trauma Pulmonary Injuries • Pulmonary Contusion – Soft tissue contusion of the lung – 30 -75% of patients with significant blunt chest trauma – Frequently associated with rib fracture – Typical MOI • Deceleration – Chest impact on steering wheel • Bullet Cavitation – High velocity ammunition – Micro hemorrhage may account for 1 - 1 ½ L of blood loss in alveolar tissue • Progressive deterioration of ventilatory status – Hemoptysis typically present
Pulmonary Contusion Signs and Symptoms • Dyspnea • Ineffective cough • Hemoptysis • Hypoxia • Chest pain • Chest wall contusion or abrasions
Ruptured Diaphragm • Potentially life-threatening • Left side more prone to injury • Results in respiratory compromise 54
Ruptured Diaphragm Signs and Symptoms • Dyspnea • Dysphagia • Abdominal pain • Sharp epigastric or chest pain radiating to the left shoulder (Kehr’s sign) • Bowel sounds in lower to middle chest • Decreased breath sounds on injured side
Blunt Cardiac Injury • Formerly called cardiac contusion or cardiac concussion • Suspect following an associated mechanism of injury (motor vehicle crash) or in those patients with poor cardiovascular response to injury
Blunt Cardiac Injury Signs and Symptoms • ECG abnormalities from dysrhythmias – Premature ventricular contractions and AV blocks are the most common • Chest pain • Chest wall ecchymosis
Pathophysiology of Thoracic Trauma Cardiovascular Injuries • Myocardial Contusion – Occurs in 76% of patients with severe blunt chest trauma – Right Atrium and Ventricle is commonly injured – Injury may reduce strength of cardiac contractions • Reduced cardiac output – Electrical Disturbances due to irritability of damaged myocardial cells – Progressive Problems • Hematoma • Hemoperitoneum • Myocardial necrosis • Dysrhythmias • CHF & or Cardiogenic shock
Pathophysiology of Thoracic Trauma Cardiovascular Injuries Myocardial Contusion Signs & Symptoms • • Bruising of chest wall Tachycardia and/or irregular rhythm Retrosternal pain similar to MI Associated injuries – Rib/Sternal fractures • Chest pain unrelieved by oxygen – May be relieved with rest – THIS IS TRAUMA-RELATED PAIN • Similar signs and symptoms of medical chest pain
Pericardial Tamponade • Collection of blood in the pericardial sac • Penetrating injury most common • Results in decreased cardiac output 60
Pathophysiology of Thoracic Trauma Cardiovascular Injuries • Pericardial Tamponade – Restriction to cardiac filling caused by blood or other fluid within the pericardium – Occurs in <2% of all serious chest trauma • However, very high mortality – Results from tear in the coronary artery or penetration of myocardium • Blood seeps into pericardium and is unable to escape • 200 -300 ml of blood can restrict effectiveness of cardiac contractions – Removing as little as 20 ml can provide relief
Pathophysiology of Thoracic Trauma Cardiovascular Injuries Pericardial Tamponade Signs & Symptoms • Dyspnea • Possible cyanosis • Beck’s Triad – JVD – Distant heart tones – Hypotension or narrowing pulse pressure • Weak, thready pulse • Shock • Kussmaul’s sign – Decrease or absence of JVD during inspiration • Pulsus Paradoxus – Drop in SBP >10 during inspiration – Due to increase in CO 2 during inspiration • Electrical Alterans – P, QRS, & T amplitude changes in every other cardiac cycle • PEA
Pericardial Tamponade Signs and Symptoms • Dyspnea • Cyanosis • Beck’s triad • Signs of shock • Decreased voltage of ECG complexes 63
Management of the Chest Injury Patient • Pericardial Tamponade –High flow O 2 –IV therapy –Consider pericardiocentesis; rapidly deteriorating patient
Pericardiocentesis • <iframe width="420" height="315" src="http: //www. youtube. com/embed/n. S_VUNZTk. Y" frameborder="0" allowfullscreen></iframe>
Pathophysiology of Thoracic Trauma Cardiovascular Injuries • Myocardial Aneurysm or Rupture – Occurs almost exclusively with extreme blunt thoracic trauma – Secondary due to necrosis resulting from MI – Signs & Symptoms • Severe rib or sternal fracture • Possible signs and symptoms of cardiac tamponade • If affects valves only – Signs & symptoms of right or left heart failure • Absence of vital signs
Aortic Injuries • Result of penetrating and blunt trauma • Descending aorta more susceptible to rupture • 10 to 30% mortality in those admitted • Ascending aorta immediately fatal 67
Aortic Injuries Signs and Symptoms • Hypotension • Decreased level of consciousness • Decreased quality of femoral pulses • Loud systolic murmur in parascapular region • Chest pain 68
Aortic Injuries Signs and Symptoms • Chest wall ecchymosis • Widened mediastinum on chest radiograph • Paraplegia • Hypertension in upper extremities • Decreased quality (amplitude) of femoral pulses compared to upper extremity pulses
Aortic Aneurysm • AVOID jarring or rough handling • Initiate IV therapy enroute – Mild hypotension may be protective – Rapid fluid bolus if aneurysm ruptures • Keep patient calm
Neck Injuries • Zone I: Extends from the sternal notch and clavicle to the cricothyroid cartilage • Zone II: To the angle of the mandible • Zone III: From the mandible to the base of the skull
Neck Injuries • Zones Clinical Significance – Identification of structures potentially injured – Potential for surgery or observation – Potential to control bleeding
Neck Injuries Signs and Symptoms • Penetrating wounds or objects • Pulsatile or expanding • Less of normal anatomic laryngeal region • Bruits • Active external bleeding impaled hematomas prominence of the
Neck Injuries Signs and Symptoms (continued) • Neurologic deficit • Cranial nerve deficits • Facial sensory or motor nerve deficits • Subcutaneous emphysema • Dysphonia • Dysphagia
Nursing Interventions for a Neck Injury • Monitor for progressive airway edema • Control external bleeding with direct pressure • Monitor for continued bleeding and expanding hematomas
Tracheobronchial Injury • Usually caused by penetrating trauma • Penetrating injuries occur in proximal trachea • Blunt injury is usually to lower trachea • Surgical intervention 76
Tracheobronchial Injury Signs and Symptoms • Dyspnea, tachypnea • Hemoptysis • Potential airway obstruction • Subcutaneous emphysema: Neck, face, suprasternal area • Decreased or absent breath sounds • Suspect/Evaluate for other closed chest trauma
Tracheobronchial Injury • Support therapy – Keep airway clear – Administer high flow O 2 • Consider intubation if unable to maintain patient airway – Observe for development of tension pneumothorax and SQ emphysema
Nursing Care - Assessment History • What was the mechanism of injury? • What are the patient’s complaints? • What were the patient’s vital signs prior to admission?
Nursing Care Physical Assessment Inspection • Observe chest wall for injuries • Assess breathing effectiveness and rate • Observe chest wall for symmetrical movement • Inspect the neck for signs of trauma
Nursing Care Physical Assessment Inspection (continued) • Jugular veins • Zone of injury • Upper abdominal region for evidence of blunt or penetrating injury
Nursing Care Physical Assessment • Percuss the chest • Palpate – Chest wall, clavicles, neck for presence of bony crepitus – Central and peripheral pulses and compare quality – The trachea – Extremities for motor and sensory function
Nursing Care Physical Assessment Auscultation • Compare blood pressure in both upper and lower extremities • Breath sounds • Chest for bowel sounds • Heart sounds • Neck vessels for bruits
Diagnostic Procedures Radiographic Studies • • • Chest radiograph Arteriography Esophagoscopy Bronchoscopy and laryngoscopy Computerized tomography (CT) scan Focused assessment sonography for trauma (FAST) 84
Nursing Diagnoses • • Ineffective airway clearance Ineffective breathing pattern Impaired gas exchange Fluid volume deficit Decreased cardiac output Altered tissue perfusion Pain
Planning and Implementation • Ensure patent airway • Administer oxygen via a nonrebreather mask at a flow rate sufficient to keep the reservoir bag inflated, 12 to 15 L/min • Prepare for ventilatory support • Cover open chest wounds with a sterile, nonporous dressing and tape on three sides • IMMEDIATELY prepare for needle thoracentesis
Planning and Implementation • Prepare for: – Chest tube insertion – Aggressive ventilatory support – Surgical intervention – Emergency thoracotomy – Autotransfusion
Evaluation and Ongoing Assessment Monitor • Airway patency, respiratory effort, and arterial blood gases • Respiratory effort after covering wounds • Vital signs • Chest tube drainage
Management of the Chest Injury Patient • Sternoclavicular Dislocation – Supportive O 2 therapy – Evaluate for concomitant injury • Flail Chest – Place patient on side of injury • ONLY if spinal injury is NOT suspected – Expose injury site – Dress with bulky bandage against flail segment • Stabilizes fracture site – High flow O 2 • Consider PPV or ET if decreasing respiratory status – DO NOT USE SANDBAGS TO STABILIZE FX
Management of the Chest Injury Patient • Traumatic Asphyxia – Support airway • Provide O 2 • PPV with BVM to assure adequate ventilation – 2 large bore IV’s – Evaluate and treat for concomitant injuries – If entrapment > 20 min with chest compression • Consider 1 m. Eq/kg of Sodium Bicarbonate
Planning and Implementation • Stabilize impaled objects • Cannulate 2 veins with large bore 14 - or 16 -gauge catheters and infuse lactated Ringer’s solution • Pericardiocentesis, as indicated • Assist with emergency department thoracotomy • Monitor and treat cardiac dysrhythmias • Administer analgesic medications
Diagnostic Procedures • Laboratory Studies – Cardiac enzymes • Other – Electrocardiogram – Central venous pressure – Echocardiography 92
Evaluation and Ongoing Assessment • Airway patency and respiratory effort – Respiratory effort after covering wounds • Vital signs • Chest tube drainage –FOCA –DOPE 93
Planning and Implementation • • • 94 Stabilize impaled objects Initiate two large-caliber intravenous catheters Assist with pericardiocentesis Monitor and treat cardiac dysrhythmias Administer analgesic medications