Penetrating Neck Trauma Nate Whittaker 121307 Penetrating Neck


















 in a zone II penetrating neck trauma:")

















 • Sympathetic chain goes")





 •")









 l Does it")


- Slides: 56
Penetrating Neck Trauma Nate Whittaker 12/13/07
Penetrating Neck Trauma l Intro l Anatomy l ABCs l Physical Exam l Diagnosis & Management
Penetrating Neck Trauma l Missile or sharp object penetrating the skin and violating the platysma (GSW, Stab, Puncture wounds, and Impalement Injuries). l 30% of cases are accompanied by injury outside of the neck zones l 5 -10% of all traumas presenting to the ED
Penetrating Neck Trauma l Higher mortality rates with injuries to large vessels (carotid or subclavian arteries and veins) l Civilian mortality rate ranges from 3 -6%
Extent of Tissue Damage l Kinetic Energy = mass x velocity 2 l Low-energy weapons - hand-driven weapons (knives, ice picks) l Medium-energy (handguns) l High-energy weapons (military assault weapons) >2500 ft/s l direct impact VS tissue displacement from temporary cavitation
Anatomy l Anterior Triangle - middle line of the neck, anterior margin of the scm, the mandible. l Posterior Triangle – posterior margin of scm, trapezius, clavicle
Anatomy
Anatomy l Zone I – between the clavicle/suprasternal notch and the cricoid cartilage. Includes the proximal common carotid, vertebral, and subclavian arteries and the lungs, trachea, esophagus, thoracic duct, major cervical nerve trunks.
Anatomy l Zone II - between the cricoid cartilage and the angle of the mandible. Includes the internal and external carotid arteries, jugular veins, larynx, pharynx, esophagus, recurrent laryngeal nerve, spinal cord, trachea.
Anatomy l Zone III - between the angle of the mandible and the base of the skull. Includes the distal extracranial carotid and vertebral arteries, the uppermost jugular veins and the pharynx.
Anatomy l Platysma – the first muscle layer under the skin of the anterolateral neck l If clearly intact, local wound repair is all that is required l If violated, STOP exploration and consult surgery. l Further exploration may dislodge a clot, increase bleeding, or cause an air embolism
ABCs
ABCs
Early Airway Intervention l Acute Respiratory Distress l Compromise from blood/secretions l Massive SQ emphysema l Tracheal Shift l MS alteration
Airway l 25 -30% of neck trauma need an emergent airway l 40% are never intubated l Consider the progression of airway distortion with air or blood transecting through fascial compartments l Unnecessary Intubation VS waiting for a difficult intubation with respiratory distress and a distorted airway
Airway l RSI l Gum Elastic Bougie l Blind Nasotracheal – perceived high failure and complication rates l Fiberoptic l Retrograde tracheal intubation l Cricothyrotomy l Tracheostomy
Emergency airway management in penetrating neck injury. Mandavia DP, Qualls S, Rokos I Ann Emerg Med. Mar 2000; 35(3): 221 -5. l LA County, Level I trauma center, 1993 -1996 l 748 cons. patients with penetrating neck injury l 82 (11%) required immediate airway management l 24 excluded because of out-of-hospital traumatic arrest or out-of-hospital intubation l 58 patients - 39 RSI with SUCC, 100% l 5 comatose - orotracheal intubation w/o paralysis l 2 - emergency tracheostomies l 12 fiberoptic intubations by ENT - 3 failed RSI l 47 (81%)total orotracheal intubations
Blind nasotracheal intubation for patients with penetrating neck trauma. Weitzel N, Kendall J, Pons P. J Trauma. May 2004; 56(5): 1097101 l Denver, Colorado, 1993 - 2001 l 240 patients with penetrating neck trauma l 89 (37%) required emergent airway management l 40 (17%) prehospital blind nasotracheal intubation l. Success rate - 90% l. Mean # of attempts was 1. 16 (range, 1 -4) l. Paramedics very experienced at blind nasotracheal intubation
Use of a gum elastic bougie (GEB) in a zone II penetrating neck trauma: a case report. Steinfeldt J, Bey TA, Rich JM. J Emerg Med 2003; 24: 267 -70 l Self inflicted 5 cm deep slash wound in zone II w/ transection of his pharynx l Blind intubation through the wound failed x 3 2/2 constant blood blow l Bougie used to intubate trachea with confirmatory clicking on tracheal rings l ET tube successfully placed over bougie into trachea
Cricothyrotomy l Favored surgical back up if RSI fails l Have kit opened and neck prepped before RSI in tenuous circumstances l Risk of disrupting stable hematoma in some trauma patients obscuring operative field and significant hemorrhage l If integrity of larynx is questionable, tracheostomy may be the best option
Airway l C-spine – maintain the best you can – No reports of unstable c-spine injuries from stab wounds (not enough force) – GSW – instability = fx in 2 columns, requiring the bullet to traverse the spinal cord neurological symptoms – Airway takes priority • Remove the collar – Use in-line cervical traction for c-spine stabilization.
Breathing l Possible to have injury to both the base of the neck and thorax – Zone I l High-Flow Oxygen/ Pulse OX l Difficulty ventilating could be an upper airway or thoracic injury l Unequal breath sounds or asymmetric chest movement = pneumo/hemothorax l Watch for tracheal deviation – tension pneumothorax
Circulation l Hard signs of Vascular Injury • • Bruit or Thrill Expanding or Pulsatile Hematoma Pulsatile or Severe Hemorrhage Pulse Deficit l Soft signs of Vascular Injury • Hypotension and Shock • Stable, nonpulsatile hematoma • Central or Peripheral nervous system ischemia • Proximity to a major vascular structure
Circulation l Control active bleeding with direct pressure l 2 Large Bore IVs and judicious fluid resuscitation l Do not clamp bleeding vessels as this can cause additional vascular and/or nerve damage l Avoid NG tubes initially as gagging may dislodge a clot hemorrhage l Mild Trendelenburg position to decrease the risk of air embolization in venous injuries
Circulation l The EJ vein can be tied off w/o adverse affect l Do NOT remove impaled objects l Deep Zone I injuries that do not stop bleeding with pressure may be from a subclavian artery injury – consider temporizing with a foley catheter
Foley catheter balloon tamponade for life-threatening hemorrhage in penetrating neck trauma. Navsaria P, Thoma M, Nicol A. World J Surg. Jul 2006; 30(7): 1265 -8 l Cape Town, South Africa 07/04 – 06/05 l 220 penetrating neck traumas l 17/18 successfully txed with foley tamponade l Foley filled with 5 ml of h 20 or until resistance felt l Zone I – 3, Zone II – 8, Zone III – 1, Posterior triangle – 5
Disability Spinal Cord Phrenic Recurrent Laryngeal Cranial Nerves IX-XII Brachial Plexus Focal neurological deficits from damage to the carotid or vertebral artery CNS Ischemia
Exposure l Expose the entire body, looking for evidence of additional trauma (30 % of penetrating neck trauma)
ED Stand-up l www. youtube. com/watch? v=k 9 m 2 F LHl. Ew. A
Who goes emergently to the OR ? l Absolute Criteria: – – – Shock Uncontrolled Bleeding No Radial Pulse Rapidly Expanding or Pulsatile Hematoma Respiratory Distress l Relative Criteria: – Air Bubbles from Wound – Hemoptysis – Crepitus
Physical Exam l Controversial how much weight should be placed on physical exam l Regardless, the more we gather from the PE, the more appropriate and timely our w/u and management will be l Demetriades et al, Los Angeles (OR full, stock in PE, chart)
Physical Exam l Vascular – 25 – 50% of cases – Active Bleeding (w/ direct pressure) • Degree – Hypotension • >100, 60 -90, <60 – Peripheral Pulses (brachial, radial) • Diminished, absent – Bruit – heard in 50% of carotid injuries • where – Hematoma (size, expanding? )
Physical Exam l Possible Vascular Injuries – Pseudoaneurysm – Dissection – Arteriovenous Fistula – Complete Transection – Thrombus Formation Stroke
Physical Exam l Larynx/Trachea – 10 % of cases – Hemoptysis (ask pt to cough) – Air bubbling though the wound (ask pt to cough) – Subcutaneous emphysema – Crepitation – Hoarseness – Trachea Midline
Physical Exam l Esophagus – 5% of cases – the most missed injury in penetrating neck trauma – – Hematemesis Pain on Swallowing sputum Subcutaneous emphysema Drooling l Mortality Rates reported as high as 17%, if detection is delayed >12 hours – Mediastinitis l Occult Injury bad outcome, but usually accompanied by suspicious signs/symptoms
Physical Exam l Nervous System - Approximately 10% have a spinal cord or a brachial plexus injury – GCS (eye, verbal, & motor responses) – Localizing Signs • Pupils • CNs – Facial – Glossopharyngeal (midline palate elevation) – Recurrent laryngeal –X- (horseness, good cough) – Accessory (shoulder shrugging) – Hypoglossal (tongue protrusion)
Physical Exam l Nervous System – Horners Syndrome (myosis, ptosis) • Sympathetic chain goes up the Carotid – Spinal cord – moving all 4 ext. – Brachial Plexus • • • Median – fist Radial – wrist ext Ulnar – abduction/adduction of fingers Musculocutaneous – forearm flexion Axillary – arm abduction
Physical Exam l Obvious signs/symptoms suggestive of major vascular or aerodigestive injuries require emergent or urgent operative intervention
Who goes emergently to the OR ? l Absolute Criteria: – – – Shock Uncontrolled Bleeding No Radial Pulse Rapidly Expanding or Pulsatile Hematoma Respiratory Distress l Relative Criteria: – Air Bubbles from Wound – Hemoptysis – Crepitus
Diagnosis & Management l Institution, Resource, and Surgeon dependant l All hemodynamically unstable patients or those with obvious aerodigestive injuries should go immediately to the OR l Everybody gets a an AP CXR & a Lateral/AP Neck l Type and Cross l Consider LA, base deficit, or bicarb
Diagnosis & Management l Historically, after WWII, routine surgical exploration of Zone II penetrating wounds was accepted l Studies in the 1980 s demonstrated a high rate of negative exploration encouraging a more selective approach to surgical management l Since then, the greatest controversy has been over how to w/u stable Zone II trauma pts without evidence of Aerodigestive injury
Diagnosis & Management l Unless hemodynamically unstable or there is evidence of aerodigestive tract injuries, surgeons prefer the selective approach in Zone I & III, given difficulty of exposure l Operative management of Zone I may require a median sternotomy or a thoracic approach and Zone III may require disarticulation of the mandible or resection of the styloid or mandible angle.
Diagnosis & Management l Three major structures to evaluate: – Vascular (namely arterial) • 4 Vessel Angiography (Gold Standard) • Duplex Ultrasonography – 90 -95% sensitivity in experienced hands to injuries requiring intervention compared to >99% w/ Angio – Esophagus • Esophagoscopy • Esophagram • Varying sens (90%), spec, & accuracy – Recommended to use both – ( almost 100% sens. Per 1 study) – Airway • Laryngoscopy • Tracheoscopy/Broncoscopy (Gold Standard)
Diagnosis & Management l l. Britt LD: Neck Injuries: Evaluation and Management, Moore EE, Feliciano DV, Mattox KL (eds): Trauma, 5 th ed New York, NY: Mc. Graw-Hill, 2004, p. 450
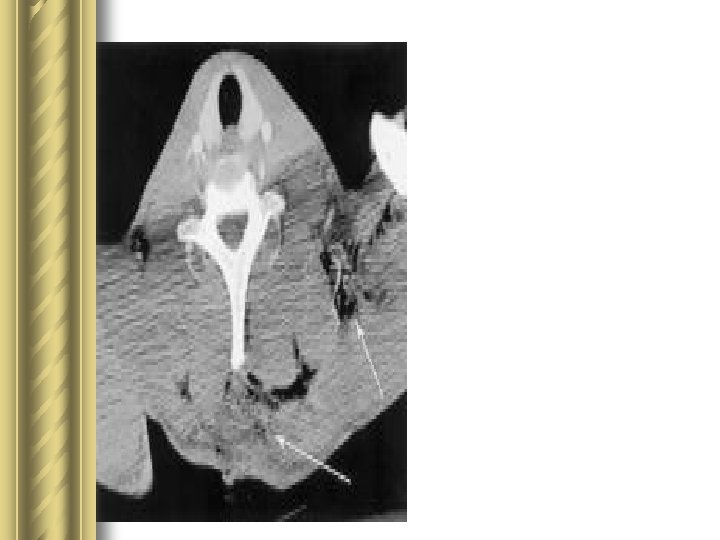
Penetrating injuries of the neck: use of helical computed tomographic angiography. Munera F, Cohn S, Rivas LA. J Trauma. Feb 2005; 58(2): 413 -8 l University of Miami l 24 – month prospective study with 60 pts with penetrating neck trauma referred for conventional angiography (vertebral and carotid) l Pts received both studies (HCTA) l Sensitivity 90%, Specificity 100% – single lesion missed from a technical error l PPV 100%, NPV 98%
Penetrating injuries of the neck: use of helical computed tomographic angiography. Munera F, Cohn S, Rivas LA. J Trauma. Feb 2005; 58(2): 413 -8 l 2 nd Study with HCTA l 27 - month prospective study – 146 pts l Sensitivity 100%, Specificity 98. 6% l PPV 92. 8%, NPV 100% l Outcomes with 46 day f/u was the standard of reference l 27 pts (15. 6%) with vascular injuries – Arterial occlusion-14, pseodoaneurysm-8, av fistulas-4, partial thromboses-2 detected
Penetrating injuries of the neck: use of helical computed tomographic angiography. Munera F, Cohn S, Rivas LA. J Trauma. Feb 2005; 58(2): 413 -8 l The 2 studies also found associated lesions in 81 pts – – – C-spine fxs – 28 Mandibular or Facial fxs – 25 Aerodigestive injuries – 4 Hematoma compressing airway – 22 Hematoma w/ spinal cord compression – 3 l No esophageal or airway injuries missed
CT Angiography in Penetrating Neck Trauma Reduces the Need for Operative Neck Exploration. Woo K et al. American Surgeon. 71(9): 754 -8, 2005 Sep. l Conclusions from this study recommend HCTA as a screening test, as the tract of injury can be seen – 1. Tract seen, no injuries NO surgery – 2. Injury to vascular or aerodigestive structure surgery – 3. Indeterminate scan further eval.
HCTA/MDCT l Limitations – Artifact from bullet fragments or other metallic foreign bodies and shoulders of large pts – Inability to perform endovascular therapy simultaneously – Not in real time
HCTA/MDCT l Benefits – Less expensive – Don’t have to call in the angio team – Less Invasive – 3 -D reconstruction – Can see trajectory of penetrating injury and proximity to structures
Diagnostic Algorithm for Penetrating Neck Trauma Penetrating neck trauma Unstable -Hemorrhagic Shock Stable -Evolving Stroke -Expanding Hematoma -Unstable Airway Physical Exam AP Chest x-ray AP/lateral soft tissue neck x-ray Normal Surgical Exploration Abnormal III Observation (Maybe) II Zones I, III - Head CT? I MDCTA/Conventional Angiography Suspicion of Aerodigestive Injury Vascular Injury Esophagoscopy/Esophagram Laryngoscopy/Bronchoscopy No Injury Observation Injury Surgical Exploration Rathlev NK, Mendozen R, Bracken ME. Evaluation and Management of Neck Traum. Emergency Med Clin N Am 25 (2007) 679 -694.
Moonlighting l Soooo…. What do you do when you are moonlighting in Marlette and a Penetrating Neck Injury walks in? l Is the platysma violated? l What would you do even if you had a HCT scanner and you found an injury? l What is your on call surgeon comfortable with?
Summary l ABCs l RSI with a back up (cric. ) l Does it penetrate the platysma l All unstable patients immediately go to the OR l Good Physical Exam l Don’t miss the esophageal Injury l If stable, consider MDCTA as a screening evaluation
References l l l Britt LD: Neck Injuries: Evaluation and Management, Moore EE, Feliciano DV, Mattox KL (eds): Trauma, 5 th ed New York, NY: Mc. Graw-Hill, 2004, p. 445 Mandavia DP, Qualls S, Rokos I. Emergency airway management in penetrating neck injury. Ann Emerg Med. Mar 2000; 35(3): 221 -5 Weitzel N, Kendall J, Pons P. Blind nasotracheal intubation for patients with penetrating neck trauma. J Trauma. May 2004; 56(5): 1097 -101 Steinfeldt J, Bey TA, Rich JM. Use of a gum elastic bougie (GEB) in a zone II penetrating neck trauma: a case report. J Emerg Med 2003; 24: 267 -70 Tintinalli, J. E. , Kelen, G. D. , and Stapczynski, J. S. (Eds. ) (2004) Disaster Medical Services: Chapter 258. Emergency Medicine: A Comprehensive Study Guide, 6 th Edition. Mc. Graw-Hill. Levy D. Neck Trauma, Emedicine. Available at: www. emedicine. com/emerg/topic 331. htm Cheng E. Penetrating Neck Trauma, Emedicine. Available at: www. emedicine. com/med/topic 2802. htm Munera F, Cohn S, Rivas LA. Penetrating injuries of the neck: use of helical computed tomographic angiography. J Trauma. Feb 2005; 58(2): 413 -8. Woo K et al. CT Angiography in Penetrating Neck Trauma Reduces the Need for Operative Neck Exploration. American Surgeon. 71(9): 754 -8, 2005 Sep. Kuzniec S, Kauffman P, Molnar LJ, et al. Diagnosis of Limb and Neck Arterial Trauma using Duplex Ultrasonography, Cardiovasc Surg. 1998: 6: 358 -66 Rathlev NK, Mendozen R, Bracken ME. Evaluation and Management of Neck Traum. Emergency Med Clin N Am 25 (2007) 679 -694. Collucciello S. Neck Trauma (Soft Tissue Injuries). EMRAP: Emergency Medicine Reviews and Perspectives 2006 Aug.
l www. youtube. com/watch? v=UMHWkbn. Dfg&feature=related