Critical Appraisal Critical Appraisal Analyze the research paper










 21: 146– 151 Knee surgery, sports. Traumatology Arthroscopy")


 • is a measure reflecting the yearly average number of")

















 •")



 d in both groups. • Closed")
")
















![• Salzmann et al. [26] had also shown that Lysholm, Tegner and Visual](https://slidetodoc.com/presentation_image_h2/9564fa51613ea98920750c3202f7e1a8/image-66.jpg "• Salzmann et al. [26] had also shown that Lysholm, Tegner and Visual")
















- Slides: 83
Critical Appraisal
Critical Appraisal Analyze the research paper to judge its trustworthiness, its value and relevance Identify the strengths and limitations in a research paper 2
Anatomy of a Scientific Article • • • Abstract Introduction Materials and Methods Results Discussion Conclusion/ Recommendation 3
Steps of evidence based Medicine 1. 2. 3. 4. 5. patient presents with a clinical problem Formulate a focused research question Search for the best evidence Critically appraise the evidence you find Decide the action to take from findings &evaluate your new practice
• Critical appraisal 1 -Evaluate of the study design 2 -Assess the methodology 3 -suitability of the statistical methods 4 -Relevance of the research to one's own practice
Relevance Personal Knowledge Validity Methods Section Results Section Applicability Personal Interpretation/ Experience
Relevance • 3 C 1. Would I care about the outcome 2. Is the topic common to my practice 3. Would the new knowledge change my practice
TYPES OF STUDIES 1. Studies on the natural history of disease 2. Studies on etiology or causes of disease (cohort studies, case control studies) 3. Studies on benefits of therapy (Clinical trials) 4. Studies on the value of diagnostic tests 5. Studies on prognosis 6. Studies on systematic reviews and meta-analyses 7. Studies on cost and economic analyses 8. Studies on clinical practice guidelines 9. Studies on quality of life measurements
Category Therapy Description Preferred Study Design Tests the effectiveness of a Randomized, double-blinded, placebotreatment, such as a drug, surgical procedure, or other intervention controlled trial Diagnosis and screening Measures the validity and reliability effectiveness of a diagnostic test, Cross-sectional survey Causation Assesses whether a substance is related to the development of an illness or condition Cohort or case-control Prognosis Determines the outcome of a disease Longitudinal cohort study (comparing the new test with a reference standard)
Validity • Were sound scientific methods used? • Bias: A systematic error, either selection, or information. • Confounding: An unmeasured interacting factor • Power: was it addressed Evaluation skills are needed A knowledge of the subject, statistical tests, and research design
Knee Surg Sports Traumatol Arthrosc (2013) 21: 146– 151 Knee surgery, sports. Traumatology Arthroscopy official journal of the ESSKA European Society of Sports Traumatology Knee Surgery and Arthroscopy
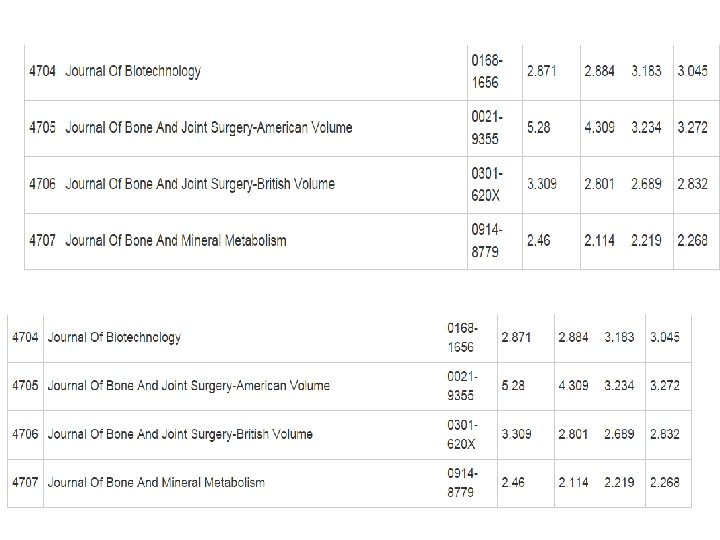
Journal impact factor (JIF) • is a measure reflecting the yearly average number of citations to recent articles published in that journal. • It is frequently used as a proxy for the relative importance o a journal within its field;
AUTHORS
Examining the paper
1
Author details • Who wrote the paper? • Institutions • Name of journal • Impact factor of the journal
2
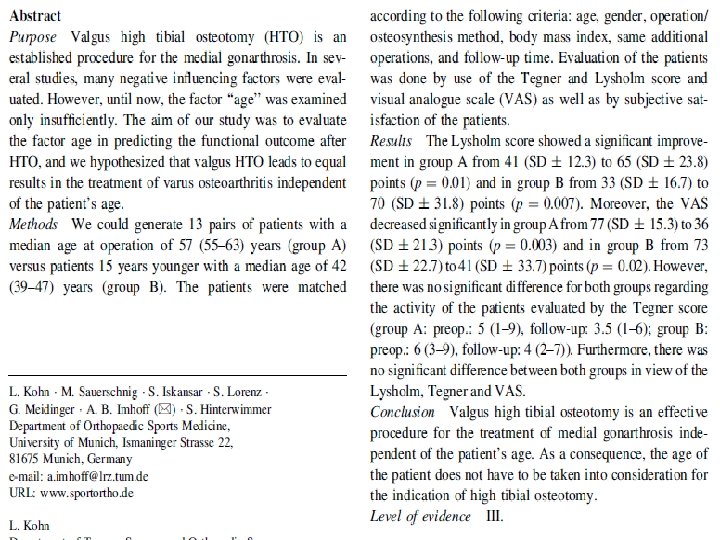
Abstract • Structured abstract • Does it address a related question? • Is the study properly designed analyzed? • Are the results important and worth knowing about? • Do you want to know more after reading the abstract? • Are there reasons to doubt the findings without reading the whole article?
3
Introduction • Is the research question clearly described? • Is the study important to answer this question? • Is the relevant background described? – What is already known and not known on the topic? – How this study differs from the previous similar studies? • Is the literature search adequate?
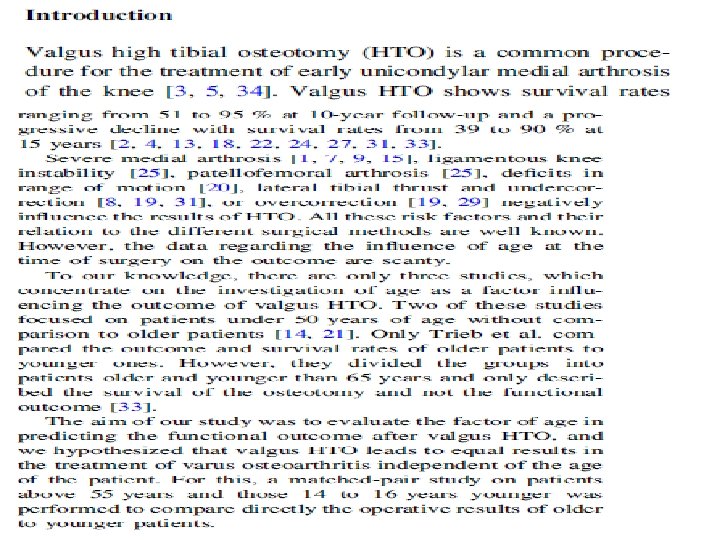
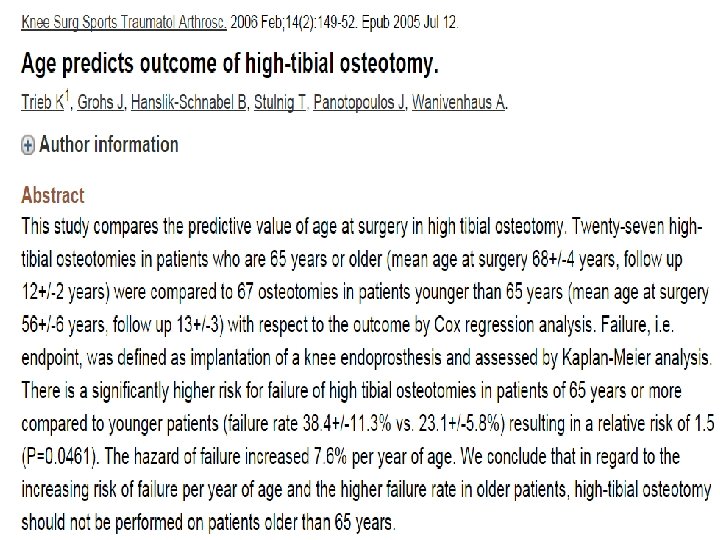
• Valgus HTO is a common procedure for the treatment of early medial OA • Severe medial arthrosis, ligamentous knee instability, PFA , deficits in ROM, tibial thrust and undercorrection, or overcorrection negatively influence the results of HTO. • All these risk factors and their relation to the different surgical methods are well known. However, the data regarding the influence of age at the time of surgery on the outcome are scanty.
• To our knowledge, there are only three studies, which concentrate on the investigation of age as a factor influencing the outcome of valgus HTO. • Two of these studies focused on patients under 50 years of age without comparison to older patients. • Only Trieb et al. compared the outcome and survival rates of older patients to younger ones. However, they divided the groups into patients older and younger than 65 years and only described the survival of the osteotomy and not the functional outcome.
• The aim of our study was to evaluate the factor of age in predicting the functional outcome after valgus HTO, and • we hypothesized that valgus HTO leads to equal results in the treatment of varus osteoarthritis independent of the age of the patient. • For this, a matched-pair study on patients above 55 years and those 14 to 16 years younger was performed to compare directly the operative results of older to younger patients.
Introduction • Is the research question clearly described? • Is the study important to answer this question? • Is the relevant background described? – What is already known and not known on the topic? – How this study differs from the previous similar studies? • Is the literature search adequate?
4
Methods Study design appropriate for question? • What is the Study design • How were the participants selected? • Justification of sample size?
• Prospective or retrospective data collection? • Are the outcomes of interest defined and measured adequately? • Statistical methods appropriate? • Ethical approval?
Materials and methods • We performed a matched-pair analysis by comparing • patients older than 55 years with a median age of 57 years (55– 63) (group A) • with patients 15 ± 1 years younger with a median age of 42 years (39– 47) (group B) • who both received a HTO between 1/2001 and 10/2007.
matching criteria: • Age (over 55 ys compared to patients 15 ys younger) • • Gender (M-F ) Operative method (open wedge–closed wedge), Osteosynthesis method (different locking plates), Additional operations microfracturing, partial internal meniscus resection less 1/3, OATS medial femoral condyle, anterior cruciate ligament reconstruction), • body mass index and follow-up time. the maximum difference between the patients of group A and B regarding to the body mass index was 2 points and regarding to the follow-up time 6 month • Furthermore, the patients of each pair showed a comparable activity level according to their work load.
• • • Exclusion criteria for all patients Chronic or acute ligament instability without reconstruction, lateral OA , absence of the lateral meniscus, Chronic inflammatory diseases like RA metabolic diseases (e. g. diabetes mellitus), hereditary diseases affecting the musculoskeletal system, drug abuse and alcohol abuse
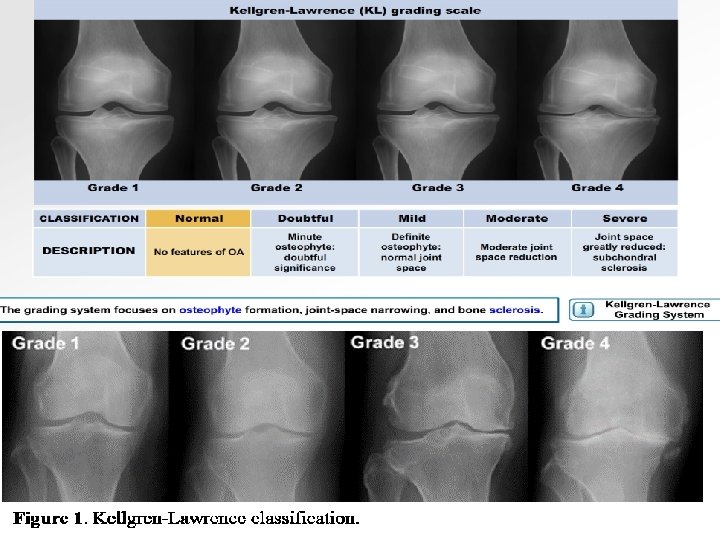
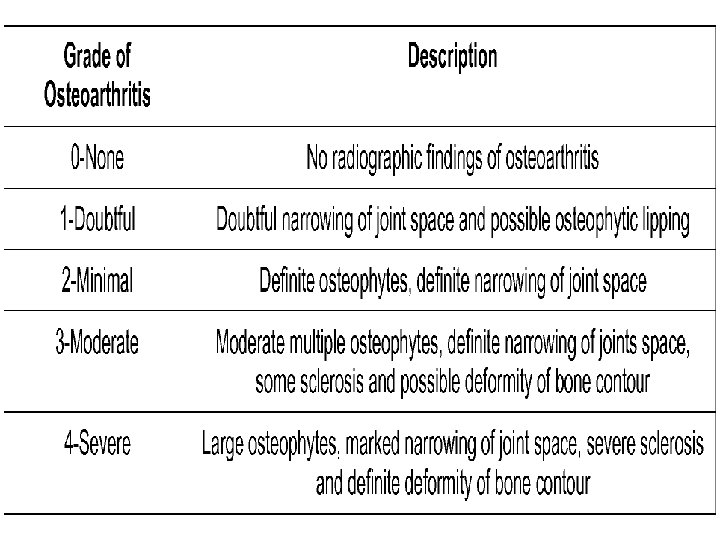
• Finally, there were 13 matched-pairs with 18 male and 8 female patients fulfilling the inclusion criteria. • The median age of group A at the time of surgery was 57 years while the median age of group B was 42 years • The median overall follow-up was 64 months (23– 90) with 68 months in group A and 63 months in group B. • the median BMI was 26. 5 with 26. 0 in group A and 26. 6 in group B. • The degree of osteoarthritis was evaluated with the help of radiographs in three plains (AP, lateral, patella tangential) based on the classification of osteoarthritis by Kellgren and Lawrence. The imaging was not predated than 3 months at time of surgical procedure. • . The median grade of osteoarthritis for the medial compartment was 2 points in group A and also 2 points in group B. Moreover, the median grade of osteoarthritis for the lateral compartment was 0 in group A and 0 in group B.
A B 57 42 68 M 63 M BMI 26 26. 6 degree of osteoarthritis M 2 2 degree of osteoarthritis L 0 0 AGE FOLLOW UP correction Median 8 (5– 14) degrees
• Median correction was 8 (5– 14) d in both groups. • Closed wedge osteotomy was performed in 18 open wedge osteotomy in the remaining 8 subjects. • There were additional procedures in 16 cases, which consisted of microfracturing (6), partial internal meniscus resection less 1/3 (12), OATS therapy of the medial femoral condyle (4) and anterior cruciate ligament reconstruction (4). • The study was performed in accordance with the Declaration of Helsinki. Informed consent from each participant was obtained prior to investigation.
Operative technique • Arthroscopy • closed wedge osteotomy using a non-locking plate (Lplate, ) and open wedge osteotomy using two different locking plates (Puddu Plate 2 nd, Arthrex, and Tomo. Fix Medial Tibial Head Plate, ). • The new mechanical axis was fixed at the Fujisawa position • In accordance with the matched-pair criteria, we only compared patients who underwent similar osteotomies with similar osteosynthesis methods and similar additional surgical procedures.
Tomo. Fix Medial Tibial Head Plate, Germany
Puddu Plate 2 nd, Arthrex
Outcome analysis • The evaluation of the outcome was conducted using a special questionnaire regarding pain (strong pain, moderate pain, sometimes pain and no pain), overall satisfaction (very satisfied = 1, satisfied = 2, partially satisfied = 3, not satisfied = 4), repetition of surgery (‘I would undergo the surgery again’, ‘I reluctantly agree to undergo the surgery again’, ‘No I would never undergo the surgery again’) • To evaluate the functional outcome of the surgery, the Lysholm score and the Visual Analogue Scale as well as the range of motion were used preoperatively and at present.
Statistical analysis • Interpretation of the results was performed using the software SPSS • The data were initially tested for the normal distribution with the Kolmogorov–Smirnov test. • Descriptive statistics for the location and scale of data distribution are given by mean and standard deviation (SD) for normally distributed data and median and range (min–max) in case of ordinal distributed data. Likewise, paired-samples t tests and Wilcoxon’s signedrank tests were used to analyse differences between pre- and postoperative values. • The analysis according to the group difference was performed with the Mann–Whitney Test. The significance level was defined as p ≤ 0. 05.
Methods Study design appropriate for question? • What is the Study design • How were the participants selected? • sample size? • Prospective or retrospective data collection? • • Statistical methods appropriate? • Ethical approval?
5
Results • • Clearly stated? • Is the result statistically significant? Are participants representative of the population to which findings are applied? • Are the analyses appropriate?
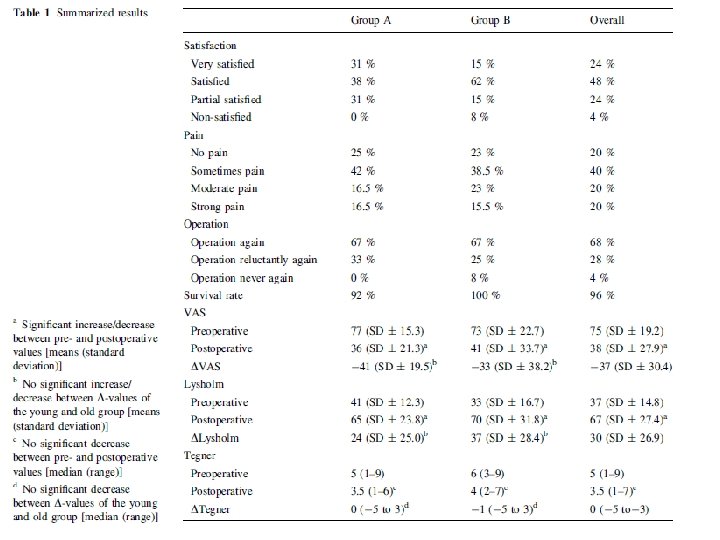
• 69 % of the patients in group A and 77 % of the patients in group B were very satisfied or satisfied with the outcome of the operative procedure. • In both groups, similarly 67 % would have the procedure again. • Regarding to the experience of pain 67 % among group A and 61. 5 % among group B described no pain. • The VAS score decreased significantly from preoperative to time of follow-up. Differences between group A and B were not significant (n. s).
• Lysholm score rose significantly corresponded to the overall collective as well as corresponded to group A and group B from preoperative to time of follow-up. Differences between group A and B were not significant (n. s). • range of motion mean flexion (group A: preop. : 135, follow-up. : 139 (SD ± 6. 7), p = n. s. ; group B: preop. : 130, follow-up: 136 , p = n. s. ) as well as mean extension (group A: preop. : 2 (, follow-up. : 3 , p = n. s. ; group B: preop. : -0. 8 , follow-up: 1. 2 , p = n. s. ) did not change significantly in group A and B preoperatively compared to postoperatively. One year after the osteotomy, one patient of group I had to be revised with an unicondylar prosthesis. This results in a 92 % survival rate for patients of group A and a 100 % survival rate in group B.
6
Discussion Limitations / biases of the study Clinical vs statistical significance? Are the conclusions appropriate? Are the conclusions based on data – do the authors extrapolate beyond data? • Implications for practice/future research? • •
Discussion • The most important finding of the present study, was that the age of the patients does not have an impact on clinical outcome. • We determine the influence of age by performing a matched-pair analysis between patients over 55 years (group A) and patients 15 ± 1 years younger (group B).
• Both groups showed a significant decrease in pain, ascertained by Visual Analogue Scale, and a significant increase in the Lysholm score. However, neither the decrease in the Visual Analogue Scale nor the increase in the Lysholm score was significant between the two groups. • Most patients, regardless of age, were satisfied or very satisfied with the result of HTO and would repeat the procedure.
• Numerous factors influencing the outcome of high tibial osteotomy have been reviewed till present. • However, there are only very few studies that investigate ‘Age’ as an influence factor. In contrast to these studies, we created two comparable groups with a representative age disparity, which permits us to make a statement about the influence factor age.
• Regardless of age, valgus high tibial osteotomy for the treatment of medial OA leads to a decreased overall pain level and thereby the functionality, represented by the Lysholm score, increases. This may be an explanation for the patients’ satisfaction with this procedure.
• The results regarding to satisfaction level, Lysholm score of these study are supported by literature. Our satisfaction rate is comparable with those reported in the previous literature. • Aglietti et al. [1] reported satisfaction rates of 87 %(from 2 to 5 years follow-up) and 70 %(from 6 to 10 years followup). • Similar results were shown in a survey by Rudan and Simurda [25] with 80 % of good or excellence results after an average follow-up of 5. 8 years.
• Salzmann et al. [26] had also shown that Lysholm, Tegner and Visual Analogue Scale scores did not differ between age groups. • However, Holden et al. [14] and Odenbring et al. showed better results in patients below 50 years compared to the outcome of older patients. • Rinonapoli et al. were unable to identify a difference in the outcomes of patients below 60 years to those over 60.
• Trieb et al. reported in their study that the failure rate after high tibial osteotomy was significantly higher in patients over 65 years compared to the younger patients. • Gstottner et al. had concluded that the survival rates of patients below 50 years were higher compared to those over 65 years. •
• The main limitation of this study is the retrospective design. Based on the follow-up, patients were interviewed about their past level of activity and level of pain. • However, this limitation affects both groups because of the matched-pair character of the study. Furthermore, these data reflect the patients’ feedback on the efficacy of high tibial osteotomy several years after the operation. • According to our opinion that makes the results of this study meaningful and interesting despite of the retrospective design.
• The findings of these study show that the indication of valgus HTO in patients with a medial gonarthrosis should not be set absolutely due to the patients’ age • but rather subjected to the status of the osteoarthritis of the medial and lateral compartment as well as to additional ligamentous instability or to a decreased range of motion.
7
Conclusion • We demonstrate that valgus high tibial osteotomy is an effective treatment option likewise in younger and older patients. • Age does not influence the outcome of the procedure in patients with medial OA
References Authorship • Citations presented in a standard format? • List of contributors reasonable? • Conflict of interest- any financial /administrative relationships with institutions related to the outcome of interest
but
Output • • Letter to the editors Further research Does the paper change your clinical practice? Back to the clinical question that made you interested in the article
QUESTION • STRENGHS VS WEAKNESS POINTS ? ? ?
• • • RESRARCH POINT. . new , benificial , common AUTHORS JOURNAL Recent article 2013 Study design and parameters We are interested in this specific point
• • • title Small sample Retrospective Questionaaire –lysholm – Vas MWO HTO ? ? ? LWC HTO
Benefits • Can the study results change management or counseling of the patient? • Next steps for further study of this problem
Paper Selection • Pick a good paper • What makes a "good" J. Club paper? • The article should be selected from a peer-reviewed, wellrespected journal in Pediatrics. • Randomized controlled trials are best, although other types of studies such as cohorts, case-control studies, and meta-analyses can occasionally be chosen. • Case reports and review articles are not appropriate for this purpose and should be avoided. • Papers that present an important concept in a clear manner. Many excellent papers are published but the data does not lend itself well to a clear presentation. .
Paper Selection Overall features: • Should clearly state WHY doing the problem in the first place (significance) – find in introduction, should be well referenced, shouldn't have to go to additional sources unless need to check specifics. • Should clearly state WHAT is the problem to be solved – see introduction. • Should clearly state HOW the problem is to be solved – see Experimental Procedures. • Should clearly state the CONCLUSIONS of the paper – see Discussion.
QUESTIONS TO ASK WHEN CRITICALLY APPRAISING A RESEARCH ARTICLE 1. 2. 3. 4. 5. Is the study question relevant? Does the study add anything new? What type of research question is being asked? Was the study design appropriate for the research question? Did the study design address the most important potential source of bias? 6. Was the study performed according to original protocol? 7. Does the study test the stated hypothesis? 8. Were the statistical analysis performed correctly? 9. Do the data justify the conclusions? 10. Are there any conflicts of interest?
Critical Appraisal of my presentation 83