Anatomy of The Forearm Dr Fadel Naim Orthopedic

































 compartment of the forearm")







![• A deep group of three muscles: 1. Flexor digitorum profundus [FDP] 2.](https://slidetodoc.com/presentation_image_h/fcabf7889c251029901bcab66a38a029/image-52.jpg "• A deep group of three muscles: 1. Flexor digitorum profundus [FDP] 2.")




















- Slides: 75
Anatomy of The Forearm Dr. Fadel Naim Orthopedic Surgeon
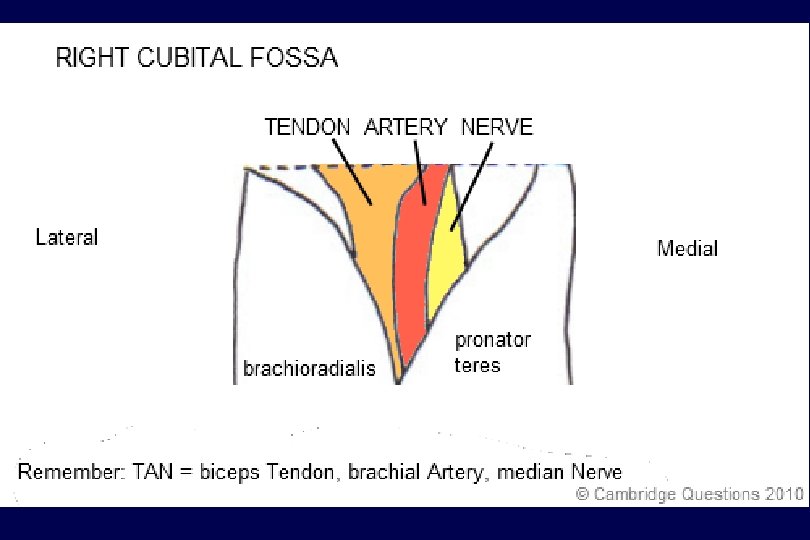
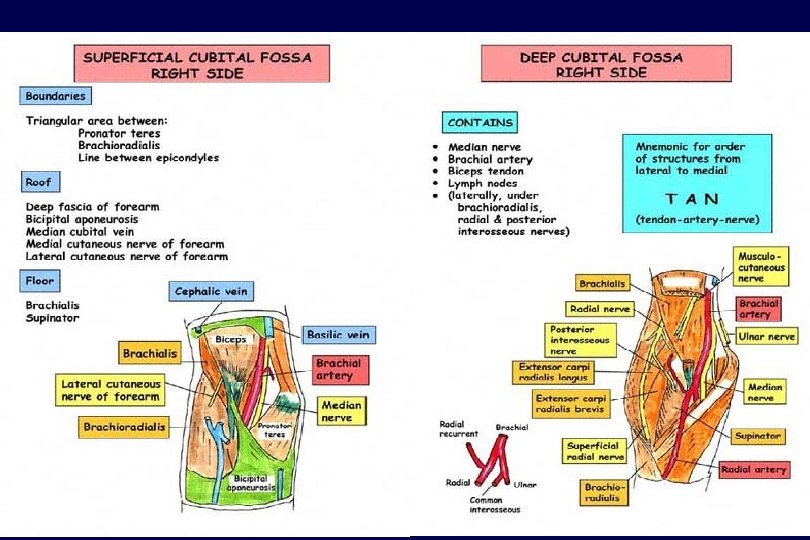
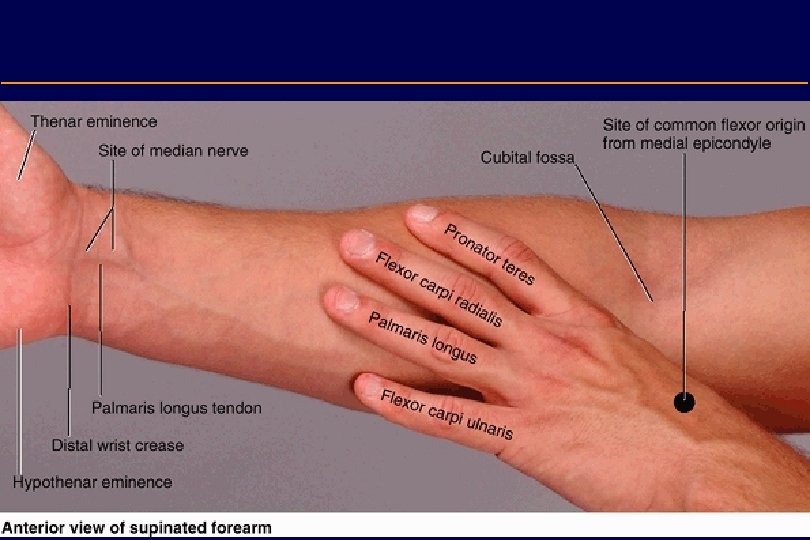
Cubital Fossa • The cubital fossa is the triangular hollow area on the anterior aspect of the elbow The boundaries of the cubital fossa are: • – Superiorly 1. – An imaginary line connecting the medial and lateral epicondyles Medially 2. – The pronator teres Laterally 3. The brachioradialis
• The floor of the cubital fossa formed by: – The brachialis muscle – Supinator muscles of the arm and forearm • The roof of the cubital fossa is formed by: – Deep fascia and reinforced by the: » Bicipital aponeurosis » Subcutaneous tissue » Skin
The contents of the cubital fossa 1. 2. Median nerve Terminal part of the brachial artery and bifurcation into – The radial artery – The ulnar artery 3. (Deep) accompanying veins of the arteries 4. Biceps brachii tendon 5. The deep and superficial branches of the radial nerve are within the floor of the fossa. • Median cubital vein, vein lying anterior to the brachial artery • • Superficially, in the subcutaneous tissue overlying the fossa Medial and lateral antebrachial cutaneous nerves related to the basilic and cephalic veins.
Cubital Fossa Venous layer 1 cephalic vein 2 basilic vein 3 median cubital vein Aponeurotic layer 1 bicipital aponeurosis 2 biceps tendon Artery-nerve layer 1 brachial artery 2 median nerve Muscular floor 1 supinator 2 brachialis 3 biceps tendon
Cubital Fossa venous layer 1 cephalic vein 2 basilic vein 3 median cubital vein Aponeurotic layer 1 bicipital aponeurosis 2 biceps tendon artery-nerve layer 1 brachial artery 2 median nerve muscular floor 1 supinator 2 brachialis 3 biceps tendon
Cubital Fossa venous layer 1 cephalic vein 2 basilic vein 3 median cubital vein aponeurotic layer 1 bicipital aponeurosis 2 biceps tendon Artery-nerve layer 1 brachial artery 2 median nerve muscular floor 1 supinator 2 brachialis 3 biceps tendon
Cubital Fossa venous layer 1 cephalic vein 2 basilic vein 3 median cubital vein aponeurotic layer 1 bicipital aponeurosis 2 biceps tendon artery-nerve layer 1 brachial artery 2 median nerve Muscular floor 1 supinator 2 brachialis 3 biceps tendon
Cubital Fossa • Bony floor 1 humerus 2 radius 3 ulna
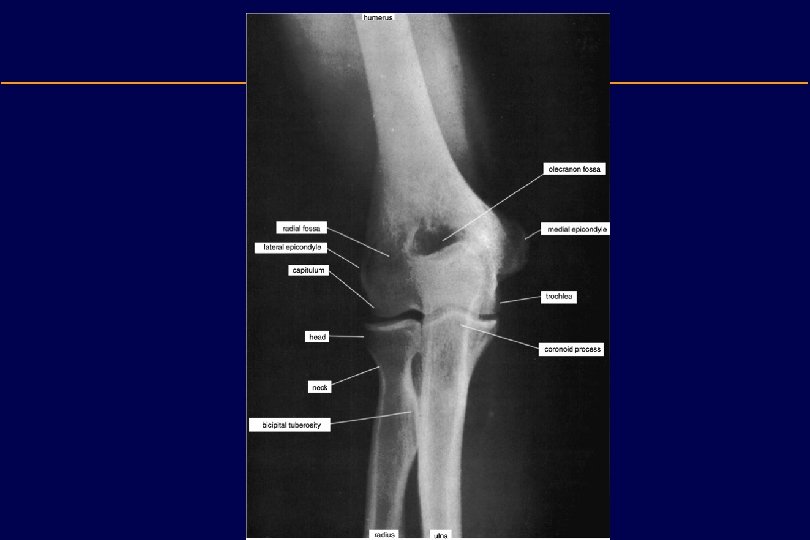
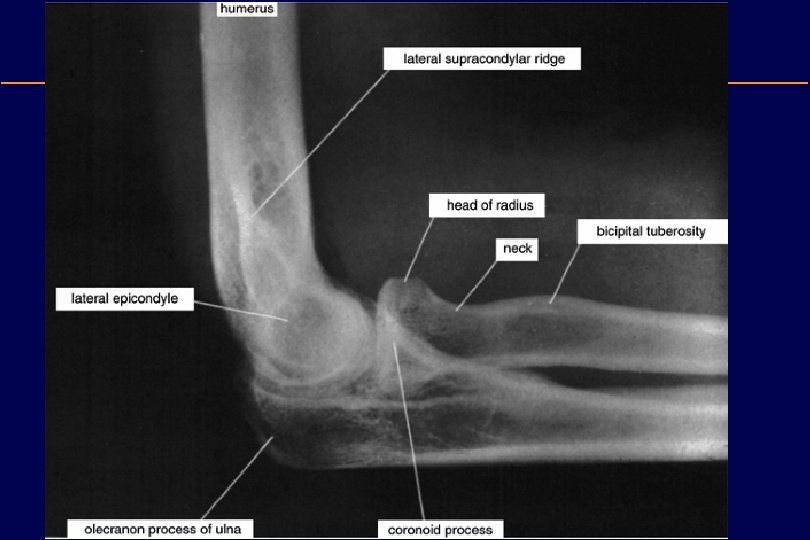
Distal Humerus • Medial epicondyle: – The pronator and flexor muscles of the forearm originate here • Lateral epicondyle: – The extensor and supinator muscles of the forearm originate here • Medial supracondylar ridge • Lateral supracondylar ridge • Trochlea (medial condyle): – Articulates with the trochlear notch of the ulna • Capitulum (lateral condyle): – Articulates with the radial head
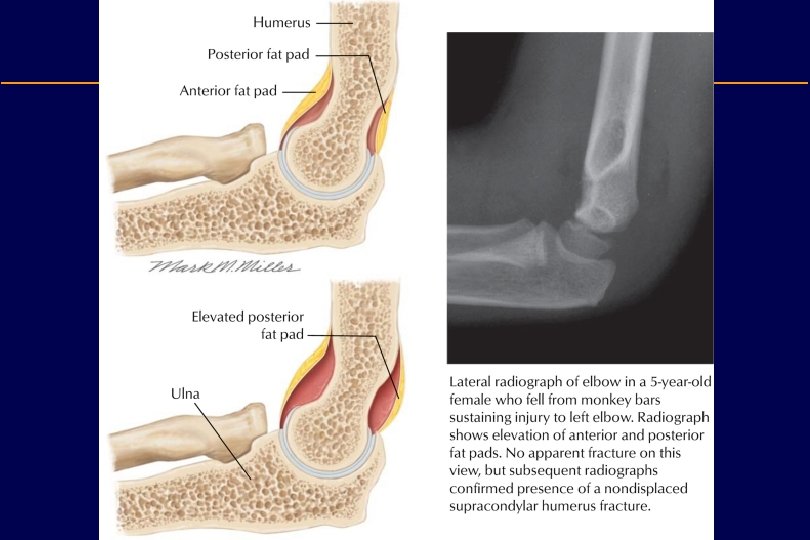
Distal Humerus • Coronoid fossa: – Accommodates the coronoid process of the ulna during flexion. – A fat pad is situated here • Radial fossa: – Accommodates the head of the radius during flexion. – A fat pad is situated here • Olecranon fossa: – Accommodates the olecranon – A fat pad is situated here • Groove for ulnar nerve
Radius • The radius is the lateral and shorter of the two forearm bones. • Its proximal end consists of: 1. A short cylindrical (or thick disc like) head » The smooth superior aspect of the head of the radius is concave for articnlation with the capitulum of the hnmerus during flexion and extension of the elbow joint. » The head also articulates peripherally with the radial notch of the ulna » The head is covered with articular cartilage. 2. A neck » Relatively constricted between the head and the tuberosity. 3. A medially directed tuberosity » The oval radial tuberosity separates the proximal end of the radius from the body.
Radius • The body of the radius has a lateral convexity and gradually and progressively enlarges in girth as it passes distally
Radius • The distal end of the radius is essentially rectangular when sectioned transversely. • Its medial aspect forms a concavity, the ulnar notch, notch which accommodates the head of the ulna. • Extending from its lateral aspect is the radial styloid process • The dorsal tubercle, tubercle (Lister’s) projecting dorsally lies between grooves for the passage of the tendons of forearm muscles
• The radial styloid process is much larger than the ulnar styloid process and extends approximately a finger's breadth further distally • This relationship is of clinical importance when the ulna and/or the radius are fractured
Radius radial tuberosity head styloid process
Ulna • The stabilizing bone of the forearm is the medial and longer of the two forearm bones • Its proximal end has two prominent projections: – The olecranon: » projects proximally from its posterior aspect – The coronoid process » Projects anteriorly.
The olecranon • The olecranon is the most proximal posterior eminence of the ulna • It is on the dorsal subcutaneous border and contains broad attachments for the triceps posteriorly • Anteriorly, the olecranon forms the trochlear notch of the ulna, which articulates with the trochlea • The radial notch – On the lateral side of the coronoid process is a smooth, rounded concavity, which articulates with the head of the radius.
Ulna • Inferior to the coronoid process is the tuberosity of the ulna for attachment of the tendon of the Brachialis muscle. • Inferior to the radial notch on the lateral surface of the ulna is a prominent ridge (the supinator crest) • Between it and the distal part of the coronoid process is a concavity (the supinator fossa) • The deep part of the supinator muscle attaches to the supinator crest and fossa.
The body of the ulna is thick and cylindrical proximally, but it tapers, diminishing in diameter as it continues distally
• At the narrow distal end of the ulna is a abrupt enlargement forming a disclike head and a small, conical styloid process • The articulation between the ulna and humerus allows primarily only flexion and extension of the elbow joint • A small amount of abduction-adduction occurs during pronation and supination of the forearm styloid process
Ulna trochlear notch coronoid process radial notch olecranon process head styloid process
• • A. Right radius B. Right ulna C. Left radius D. Left ulna – – – – 1. Proximal head 2. Neck 3. Radial tuberosity 4. Anterior oblique line 5. Interosseous border 6. Styloid process of radius 7. Ulnar notch 8. Olecranon process 9. Trochlear notch 10. Coronoid process 11. Ulnar tuberosity 12. Styloid process of ulna 13. Distal head 14. Distal neck 15. Radial notch
Colles’ fracture • The ‘dinner fork’ deformity in this fracture of the lower radius • Caused by a fall on the outstretched hand
Smith’s fracture • A Smith’s fracture is a ‘reversed’ Colles’ fracture • Often caused by a blow or fall on the dorsum of the wrist. • There may often be an associated fracture of the ulnar styloid process.
Supracondylar fractures • These fractures occur most commonly in children between the ages of 6 -9 years. • These fractures may lead to vascular and neurological complications
Olecranon Bursitis "student's elbow" • The subcutaneous olecranon bursa is exposed to injury during: – Falls on the elbow – Infection from abrasions of the skin covering the olecranon – Repeated excessive pressure and friction • Subtendinous olecranon bursitis is much less common. – Results from excessive friction between the triceps tendon and olecranon resulting from repeated flexion-extension of the forearm • The pain is most severe during flexion of the forearm because of pressure exerted on the inflamed subtendinous olecranon bursa by the triceps tendon.
Radial Head Fracture • Radial head fractures are generally caused by longitudinal loading from a fall on an outstretched hand or dislocation of the elbow.
Olecranon Fractures • Fracture of the olecranon commonly occur with a direct blow or as an avulsion injury with triceps contracture • The fractures generally are transverse or oblique in orientation and enter the trochlear notch.
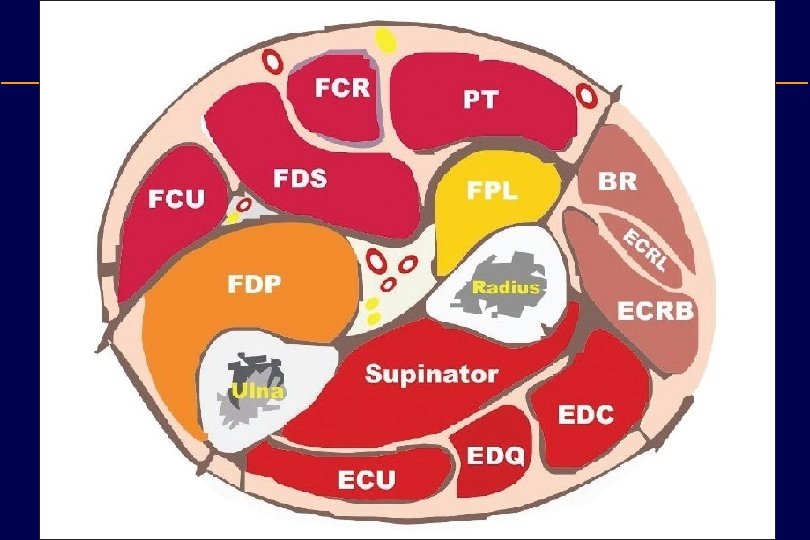
Fascial Compartment Of The Forearm • Four interconnected compartments of the forearm are recognized (1) the superficial volar compartment (2) the deep volar compartment (3) the dorsal compartment (4) the lateral compartment containing the mobile wad of henry » Brachioradialis » Extensor carpi radialis longus » Extensor carpi radialis brevis
Fascial Compartment Of The Forearm • These fascial compartments are separated by an interosseous membrane connecting the radius and ulna. • The flexors and pronators of the forearm are in the anterior compartment and are served mainly by the median nerve; nerve • The one and a half exceptions are innervated by the ulnar nerve • The extensors and supinators of the forearm are in the posterior compartment and are all served by the radial nerve
• The proximal parts of the "anterior" "anterior (flexor-pronator) compartment of the forearm lie anteromedially • The posterior (extensor-supinator) compartment lies posterolaterally • The compartments become truly anterior and posterior in position in the distal forearm and wrist. • The anterior compartment of the forearm is exceptional because it communicates with the central compartment of the palm through the carpal tunnel
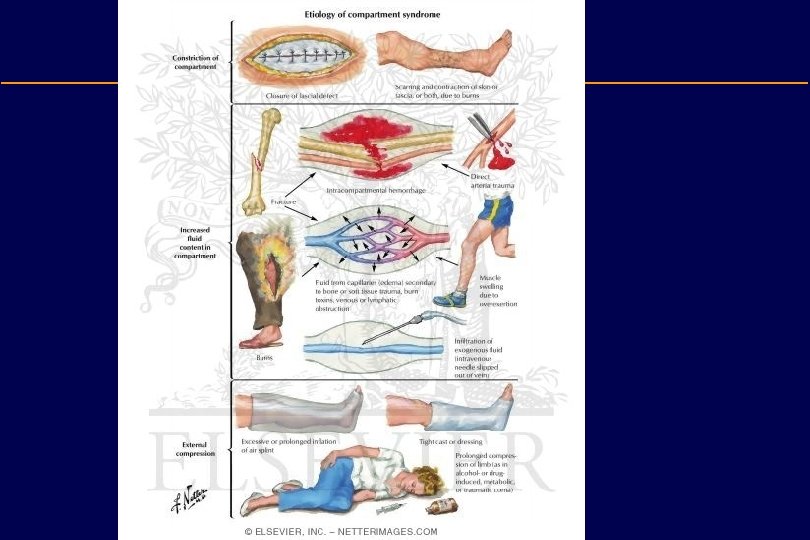
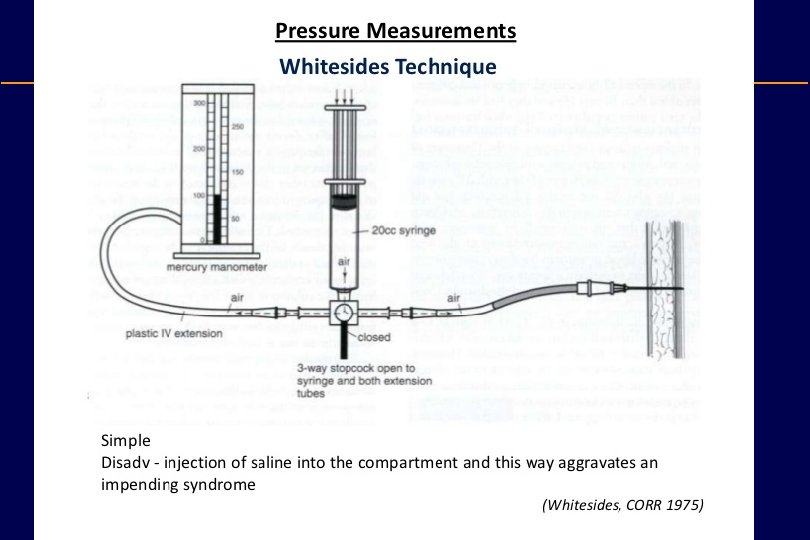
Compartment Syndrome • TRUE ORTHOPEDIC EMERGENCY • A condition characterised by raised pressure within a closed space with a potential to cause irreversible damage to the contents of the closed compartment • Leads to muscle ischemia and necrosis. • Compartment syndrome may result from » » » A fracture A soft-tissue injury An arterial injury causing ischemia, necrosis, and edema A burn By external compression from immobilization
Compartment Syndrome • Sings and symptoms the 6 “P’s”: » » » • Pain? Paresthesias? Paralysis? Pallor? Pulselessness? poikilothermia (cool limb)? Treatment – Emergency fasciotomy » – – Decreases pressure by opening “closed space” Often, will leave skin open because of severe swelling of muscles Delayed primary closure or secondary clousre
Volkmann's ischemic contracture • If compartment syndrome is untreated or inadequately treated, compartmental pressures continue to rise until irreversible tissue ischemia occurs • Volkmann ischemic contracture is the result of several different degrees of tissue injury • The earliest changes usually involve the flexor digitorum profundus muscles in the middle third of the forearm • The typical clinical picture of established volkmann contracture includes: – – – Elbow flexion Forearm pronation Wrist flexion Thumb adduction Metacarpophalangeal joint extension finger flexion
Flexor-Pronator Muscles of the Forearm • In the anterior compartment of the forearm • Separated from the extensor muscles by: – The radius – The ulna – The interosseous membrane • The tendons of most flexor muscles are located on the anterior surface of the wrist and are held in place by – The palmar carpal ligament – The flexor retinaculum • The flexor muscles are arranged in four layers and are divided into three groups – Superficial – Intermediate – Deep
• A superficial group of five muscles 1. 2. 3. 4. 5. • Pronator teres Flexor carpi radialis Palmaris longus Flexor carpi ulnaris Flexor digitorum superficialis [FDS] ( intermediate) intermediate These muscles all attach, at least in part, by a common flexor tendon from the medial epicondyle of the humerus the common flexor attachment
• A deep group of three muscles: 1. Flexor digitorum profundus [FDP] 2. Flexor pollicis longus 3. Pronator quadratus
• All muscles in the anterior compartment of the forearm are supplied by the median and/or ulnar nerves • Functionally, the brachioradialis is a flexor of the forearm • It is located in the posterior (posterolateral) or extensor compartment • It is supplied by the radial nerve • A major exception to the rule that: – The radial nerve supplies only extensor muscles – All flexors lie in the anterior (flexor) compartment.
1. Pronator Teres • Origin: – Humeral head: » Medial epicondyle » Medial supracondylar ridge » Medial intermuscular septum – Ulnar head: » Medial border of coronoid process • Insertion: – Middle of lateral surface of radius – Just posterior to most prominent part of lateral convexity of radius • Innervatlon: – Median nerve (C 6 and C 7) • Action: – Pronator of the forearm and a flexor of the elbow joint.
Pronator Teres • The pronator teres is prominent when the forearm is strongly flexed and pronated • Its lateral border forms the medial boundary of the cubital fossa • To test the pronator teres: – The person's forearm is pronated from the supine position against resistance provided by the examiner. – If acting normally, the muscle can be seen and palpated at the medial margin of the cubital fossa.
2. Flexor Carpi Radialis • Origin: – Medial epicondyle of humerus • Insertion: – Base of 2 nd and 3 rd metacarpal bone • Innervation: – Median nerve (C 6 and C 7) • Action: – Flexion (when acting with the flexor carpi ulnaris) – Abduction of the wrist (when acting with the extensors carpi radialis longus and brevis) – A combination of flexion and abduction at the wrist ( when acting alone )
Flexor Carpi Radialis • Located medial to the pronator teres. • In the middle of the forearm, its fleshy belly • The tendon of the flexor carpi radialis is a good guide to the radial artery, artery which lies just lateral to it • To test the flexor carpi radialis: – The person is asked to flex the wrist against resistance. – If acting normally, the tendon can be easily seen and palpated.
3. Palmaris Longus • Origin: – Medial epicondyle of humerus • Insertion: – Distal half of flexor retinaculum and palmar aponeurosis • Innervation: – Median nerve (C 7 and C 8) • Action: – Flexes hand (at wrist) – Tightens palmar aponeurosis
Palmaris Longus • This small fusiform muscle is absent on one or both sides (usually the left) in approximately 10% of people, people but its actions are not missed. • The palmaris longus tendon is a useful guide to the median nerve at the wrist. • The tendon lies deep and slightly medial to this nerve before it passes deep to the flexor retinaculum. • To test the palmaris longus: – The wrist is flexed and the pads of the little finger and thumb are pinched together. – If present and acting normally, the tendon can be easily seen and palpated.
4. Flexor Carpi Ulnaris • Origin: – Humeral head: » medial epicondyle of humerus – Ulnar head: » olecranon and posterior border of ulna • Insertion: – Pisiform bone – Hook of hamate bone – 5 th metacarpal bone • Innervation: – Ulnar nerve (C 7 and C 8) • Action: – – – Flexes and adducts the hand at the wrist simultaneously if acting alone. Flexes the wrist when it acts with the flexor carpi radialis Adducts it when acting with the extensor carpi ulnaris.
Flexor Carpi Ulnaris • The most medial of the superficial flexor muscles. • This muscle is exceptional among muscles of the anterior compartment, being fully innervated by the ulnar nerve. • The tendon of the flexor carpi ulnaris is a guide to the ulnar nerve and artery, which are on its lateral side at the wrist • To test the flexor carpi ulnaris: – The person is asked to put the posterior aspect of the forearm and hand on a flat table. – The person is then asked to flex the wrist against resistance while the examiner palpates the muscle and its tendon.
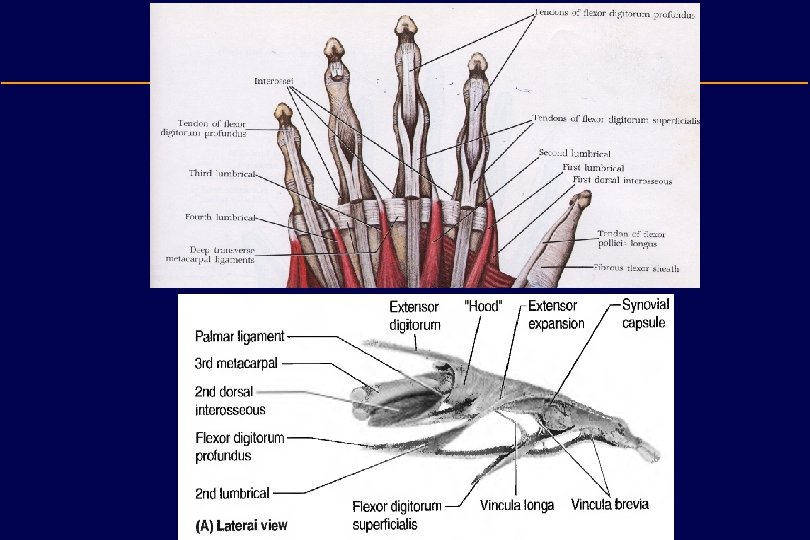
1. Flexor Digitorum Superficialis • Origin: – Humeroulnar head: » Medial epicondyle of humerus » Ulnar collateral ligament, » Coronoid process of ulna – Radial head: » Superior half of anterior border of radius • Insertion: – Bodies of middle phalanges of medial four digits • Innervation: – Median nerve (C 7, C 8, and T 1 ) • Action: – Flexes middle phalanges at proximal interphalangeal joints of medial four digits – Acting more strongly, it also flexes proximal phalanges at metacarpophalangeal joints and hand
Flexor Digitorum Superficialis • The largest superficial muscle in the forearm. • The FDS actually forms an intermediate layer between the superficial and deep groups of forearm muscles. • The tendon to the middle and ring fingers lays anterior to those of the index and little fingers • To test the FDS: – One finger is flexed at the proximal interphalangeal joint against resistance and the other three fingers are held in an extended position to inactivate the FDP.
Flexor Digitorum Profundus • Origin: – Proximal three-fourths of medial and anterior surfaces of ulna – Interosseous membrane • Insertion: – Bases of distal phalanges of medial four digits • Innervation: – Medial part ( the muscle serving digits 4 and 5 ) » Ulnar nerve (C 8 and T 1) – Lateral part: ( the muscle serving digits 2 and 3 ) » Median nerve (C 8 and T 1 ) • Action: – Flexes distal phalanges at distal interphalangeal joints of medial four digits – Assists with flexion of hand
Flexor Digitorum Profundus • The FDP flexes the distal phalanges of the medial four digits after the FDS has flexed their middle phalanges • Each tendon is capable of flexing: – Two interphalangeal joints – Metacarpophalangeal joint – The wrist joint • The tendons of FDP pass posterior to the tendons of the FDS and the flexor retinaculum. • To test the FDP: – The proximal interphalangeal joint is held in the extended position while the person attempts to flex the distal interphalangeal joint. – The integrity of the median nerve in the proximal forearm can be tested by performing this test using the index finger, finger and that of the ulnar nerve can be assessed by using the little finger
Flexor Pollicis Longus • Origin – Anterior surface of radius and adjacent interosseous membrane • Insertion – Base of distal phalanx of thumb • Action – Flexes phalanges of 1 st digit (thumb • Innervation – Anterior interosseous nerve from median nerve (C 8 and T 1)
• The flexor pollicis longus is the only muscle that flexes the interphalangeal joint of the thumb. • It also flexes: – The metacarpophalangeal – Carpometacarpal joints of the thumb – May assist in flexion of the wrist joint. • To test flexor pollicis longus – The proximal phalanx of the thumb is held and the distal phalanx is flexed against resistance.
Pronator Quadratus • Origin – Distal 1/4 of anterior surface of ulna • Insertion – Distal 1/4 of anterior surface of radius • Action – Pronates forearm; deep fibers bind radius and ulna together • Innervation – Anterior interosseous nerve from median nerve (C 8 and T 1)
Pronator Quadratus • Cannot be palpated or observed because it is the deepest muscle in the anterior aspect of the forearm. • The only muscle that attaches only to the ulna at one end and only to the radius at the other end. • The prime mover in pronation. • Initiates pronation • Assisted by the pronator teres when more speed and power are needed.
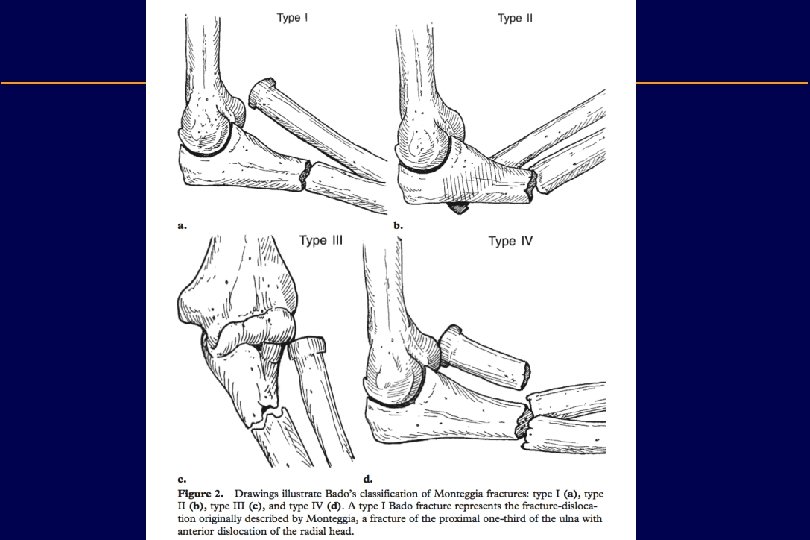
Radius and ulnar shaft fracture Diagnosis • It is important always to X-ray the whole shaft of both radius and ulna and to include both the wrist and the elbow. • Avoid missing: n Monteggia fracture: A dislocated head of radius with an isolated fracture of the ulna n Galeazzi fracture: A dislocated distal radio-ulnar joint with an isolated fracture of the radius
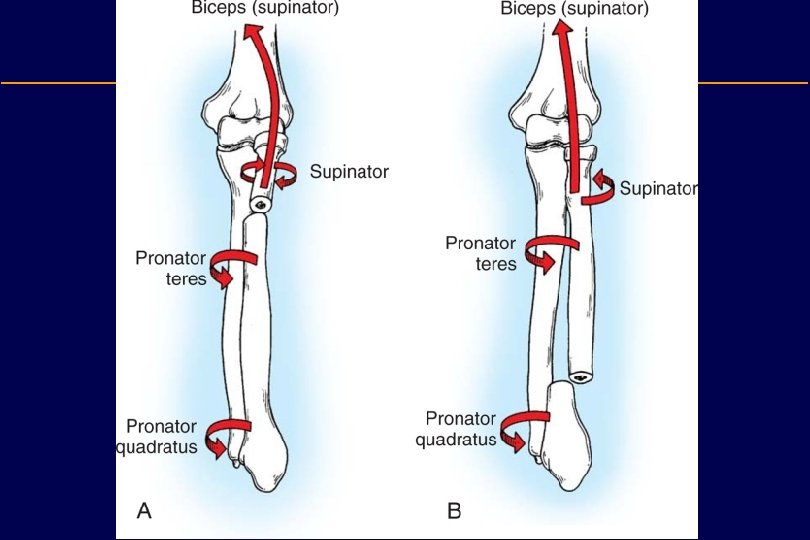
Radial Fracture • Radius fracture proximal to the insertion of pronator teres muscle – The supinator and biceps brachii muscles supinate the proximal fragment and draw it laterally. – The pronator teres and pronator quadratus muscles pronate the distal fragment and draw it medially.