Deformities of the Lower Limb Dr Fadel Naim

Deformities of the Lower Limb Dr. Fadel Naim Consultant Orthopedic Surgeon Faculty of Medicine IUG

n Positional deformations: abnormalities mechanically produced by alterations of the normal fetal environment, which restrict fetal movement and/or cause significant fetal compression.

n Common variations include: – Rotational problems • Intoeing • Out-toeing – Angular problems • Genu varum [bowlegs] • Genu valgum [knock-knees] n In most cases, the complaint is a variation of normal growth and development n In most cases, the problem resolves without treatment as the child grows

n The normal range of rotation of the foot, leg, and hip includes measurements that fall within 2 standard deviations of the mean n A variation becomes a deformity when the amount of deviation from normal for that particular age is more than two standard deviations n A careful history and physical examination are all that are necessary to determine whether a complaint requires further evaluation

History n n n What is the specific concern? Who is concerned? When does it manifest? Duration? Improving or worsening?

History Taking n Chief complaint. – Know exactly what concerns the parents in order to provide prognostic information and discussion of natural history. n Complete medical history. – Maternal pregnancy, birth, and development. – Questioning perinatal events and motor development ( cerebral palsy? ). n Duration of complaint and progression. – History should clarify if the problem began at birth, or before or after walking. – How has the problem changed during the past few months? n Family history. – Frequently familial tendency. – Parents' experience and attitudes toward similar problems.

History Taking n Signs and symptoms – – n Pain Limping Tripping Falling Why the concern – Gait or cosmoses – A lack of understanding regarding the maturation of the gait n Sitting habits – Sitting on the feet ( internal tibial torsion ) – Sitting in a "W" position (increased femoral anteversion) n Aggravating factors – Torsional deformities become more apparent with fatigue

Physical Examination n Assessment of height and weight – Normal size for age makes pathologic conditions unlikely (e. g. Hypo-phosphatemic rickets, metabolic bone disease) n Examination of the spine: – Scoliosis – Hairy patches – Sinus openings n A neurologic examination should be done to rule out neuromuscular disorders

Generalized Ligamentous Laxity 1. 2. 3. 4. Passive foot dorsiflexion in excess of 45 degrees The ability to hyperextend the knees (recurvatum) The ability to hyperextend the elbows Passive extension of the metacarpal phalangeal joints of the hands beyond 90 degrees 5. The ability to touch the thumb to the forearm with the wrist fully flexed n Evidence of joint laxity mimics the appearance of a torsional/angular deformity n The majority of children less than three years of age will have all the findings

Rotational Profile n The child’s rotational profile, as described by Staheli, should be recorded. n The four components in this profile are: 1. Hip rotation – Internal rotation – External rotation n Thigh foot axis Heel bisection line Foot progression angle

Torsional Profile Measuring a child’s torsional profile and comparing values with published normal values can differentiate conditions that cause intoeing and determine the level and severity of the problem
 v The angle formed between the longitudinal axes of the")
Foot progression angle (FPA) v The angle formed between the longitudinal axes of the feet relative to the line of forward progression during ambulation. v For children and adults, the normal FPA measures 0 -30° external rotation v When estimating the FPA, focus on one foot at a time, because the FPA will often change with each step

Foot Progression Angle

Prone Hip Rotation

Assessing hip rotation Medial Rotation Hip Lateral Rotation Hip

Femoral Anteversion Values n n n Birth = average 40º Usually corrects 25º by 10 years old Adult = average 15º
 v With the relaxed child’s ankle held gently in neutral dorsiflexion,")
Thigh-foot Axis (TFA) v With the relaxed child’s ankle held gently in neutral dorsiflexion, a goniometer may be used to measure the angle formed by the longitudinal axis of the heel and the long axis of the thigh v By walking age, the normal TFA measures 0 -30° external rotation
 Age 10")
Normal TFA Values n n n Birth = -5º (-30º to 20º) Age 10 = 8º (-5º to 30º) Adult = 23º (0º to 40º)
 L TFA R TFA")
Thigh-foot Axis (TFA) L TFA R TFA

Assessing alignment of the foot n n Shape of the foot Heel-bisector angle

Intoeing n n n n Toeing-in is the most common rotational deformity seen in the growing child This term applied to ambulatory children who consistently point their feet toward the midline Quantified by measuring the “foot progression angle” (FPA) Significant intoeing has both functional (tripping) and cosmetic implications More likely than outtoeing to be brought to the attention of the parents and health providers Intoeing is often worse when children are tired or when running The intoeing can be expected to resolve spontaneously in >95% by the age of 8 years

n In-toed gait can be due to any rotational forces applied to the lower extremity at any point from the pelvis to the toe n the underlying anatomical and physiological basis for an in-toed gait – Osseous involvement – soft tissue involvement – a combination of both

Causes Of Intoeing n The causes of in-toeing can be divided into three broad categories 1. At the level of the hip (Femoral anteversion) 2. At the level of the leg (Internal tibial torsion ) 3. At the level of the foot (Metatarsus adductus) n In order to manage the problem effectively, the level of the deformity must be determined

Cause Of Intoeing In Relation To The Age Of The Child – In the first year of life: • Metatarsus adductus, alone or combined with internal tibial torsion – In toddlers: • Internal tibial torsion alone or combined with metatarsus adductus – In early childhood: • Femoral anteversion

n The most common causes of intoeing are: – internal tibial torsion – internal femoral torsion (excessive femoral anteversion) n These two deformities may be additive, occurring together to cause significant intoeing n The diagnosis of both of these conditions can be reasonably made using physical examination alone, and imaging studies are rarely indicated

In-toeing at the Level of the Foot n n Metatarsus adductus is one of the causes of in-toeing at the level of the foot Overpowering: – tibialis anterior muscle – tibialis posterior muscle – adductor hallucis muscle • An overactive tibialis posterior muscle: – a reducible forefoot varus, with associated forefoot adduction • Tibialis anterior overactivity – an inversion of the forefoot n Fatigue has also been stated as one of the causes of in-toeing in a child, in particular associated with stiff, heavy shoes

Metatarsus Adductus n The most common congenital foot deformity n Occurring in one out of 1, 000 live births n More frequently in female children and on the left side more than the right n The most likely cause is intrauterine packing (first born children) n Forefoot is pulled inward at the tarso-metatarsal joints as viewed in the transverse plane n 85 - 90 % of cases of metatarsus adductus identified at birth resolve without treatment by one year of age n The ankle has normal motion

v The foot should be assessed for flexibility v If this cannot be done, then the deformity is rigid (i. E. , Metatarsus varus) v The foot is placed in neutral with one hand, while the opposite hand forcibly attempts to reduce the deformity by grasping the metatarsals on the transverse plane

n Mild cases – manually correctable without force n Moderate cases – manually correctable only with force n Severe cases – fixed and not manually correctable The heel bisector should pass between toes two and three

Placing the child's foot into a 'V' formed between the second and third fingers of the examiner's hand

Conservative Treatment n n n Stretching and manipulation Plaster/serial casting Splints and braces Modification of sleeping habits Shoe therapy Often, combinations of these treatment options

n Flexible metatarsus adductus is managed by stretching exercises during the first 8 months of life n Parents are instructed to hold the infant's hindfoot in one hand, the forefoot in the other, and stretch the midfoot, opening the "c"-shaped curve and slightly overcorrecting it n This exercise should be performed five times at each diaper change n This position is then held for a period of about 15 - 20 seconds, then released. This should be continued for about 10 to 15 minutes n Better results occur if treatment is begun before 8 months of age but can succeed up to age 2 years

n Flexible deformities that persist beyond 8 months, and rigid deformities, deformities may need a cast n Casts should be changed biweekly with correction usually achieved after three or four casts n Generally, if treated early, 1 or 2 casts over a period of 2 - 4 weeks is enough to achieve a full correction of the deformity n Following the use of serial casting use of a splint or brace should be used to maintain the correction
 n Inward or medial torque of the tibial shaft an")
Internal Tibial Torsion (ITT) n Inward or medial torque of the tibial shaft an inward rotation of the ankle joint n The most common cause of intoeing n Affects males and females equally n Often asymmetrical with the left side affected more than right n Walking with the patella facing forward and the feet pointing inward n The cause is believed to be: – Intrauterine position – Sleeping in the prone position after birth – Sitting on the feet

Transmalleolar Axis medially rotated compared to Transcondylar Axis

n Persistent ITT less than 10° is of little consequence if femoral torsion is normal – since the hips may readily compensate with sufficient external rotation to prevent tripping n Asymmetrical tibial torsion, with > 10° difference requires a more thorough evaluation for – growth disturbance (infantile tibia vara) – a neurological etiology (spastic monoparesis) n ITT ( > 15°) associated with progressive bowleg warrants radiographic evaluation of the knees – rule out infantile tibia vara (blount’s disease) in a child greater than 20 months of age

n 90% of ITT cases resolve by the time the child reaches 8 years of age n Avoiding – prone sleeping – sitting on feet n No efficacy in the treatment of tibial torsion, and their expense is rarely justified – – braces, casts twister cables exercises orthopedic shoes have shown

Orthopedic management for: n – – – A toddler with asymmetrical ITT, Severe ITT > 15°, ITT associated with progressive bowleg Surgical derotation of the tibia, usually at the level of the distal metaphysis, is typically reserved for n (1) Older than 8 years of age (2) A child with significant or functional deformity (3) A thigh-foot angle of greater than 3 STD beyond the mean Osteotomy of the tibia has been associated with a high complication rate n – (Compartment syndrome or peroneal nerve injury)

Excessive Femoral Anteversion n Femoral “anteversion” relates to the anterior projection of the femoral neck relative to the transverse axis of knee flexion n One of the most common diagnoses in a general pediatric orthopedic clinic occurs more frequently in girls n – usually diagnosed after 3 years of age – peaks at 4 to 6 years – then gradually resolves usually bilateral, n Other than patellar mal-tracking, there is little evidence that EFA predisposes to any other orthopedic problems

n Problems primarily cosmetic n an increased incidence of patellofemoral pain in females n no evidence of hip or back problems or functional deficit in adults

n When an adult stands in the anatomic position with the patellae facing anteriorly, the femoral neck typically points forward approximately 15° n Infants frequently 30°-40° of femoral anteversion, – gradually regresses by 1 -2° per year until skeletal maturity n ("kissing patellae“ ”squinty patella sign” ) – The child with increased femoral anteversion walks with his or her patellae and feet pointing inward n With the knee in neutral rotation, the greater trochanter can be palpated posteriorally rather than in its normal lateral presentation

n To objectively measure femoral neck anteversion a CT scan of the femoral neck and distal femoral condyles is needed, n Reserved only for preoperative evaluation of complex hip deformities n One of the easiest methods is to compare internal versus external hip rotation in the prone child n With increasing internal femoral torsion, the hip will show greater internal rotation with a corresponding decrease in external rotation
 when hip internal")
n Intoeing tends to become clinically evident (assuming neutral tibial torsion) when hip internal rotation exceeds 70° or measures at least 30° greater than hip external rotation n Each increment of 10° femoral torsion above 70° increases the degree of severity ( mild, moderate, and severe ) n The hip range of motion can be measured every six to 12 months to document gradual decrease in femoral anteversion

Causes of excess rotation n Soft tissues vs. bony anatomy n Hip joint - soft tissue contractures – Newborns have an posterior capsular contracture, producing excessive lateral rotation of the hips n Femoral antetorsion - bony anatomy – produces excessive medial rotation at the hip

Femoral antetorsion

n n n The hips of pre-walkers have limited internal rotation later show excessive internal rotation after the external rotation contracture has resolved with ambulation If there is sufficient external tibial torsion to compensate – may have a normal FPA – the knees rotate internally during ambulation n Soft tissue factors contributing to in-toeing include – spastic contracture or tight internal hip rotators – tight hip capsules – a tight ilio-tibial band

n Spontaneous resolution occurs in more than 80 % of cases by late childhood n Nonoperative treatment is ineffective n Spontaneous correction of EFA cannot be accelerated with: – Braces • including twister cables • denis-browne bars) – Orthopedic shoes – Exercises – Sleeping in the prone position

n n Correction can be obtained only by femoral osteotomy Orthotic devices are contraindicated because they will produce an external tibial torsion rather than derotating the femur

n The spontaneous correction of intoeing from EFA is due to – gradual reduction in the anterior projection of the femoral neck with growth – as a result of the child’s development of selfimage in the pre-teen years n The process of correction can be aided with – various stretching of affected muscles and muscle groups.
 older than 8 years")
n Conditions that may support a surgical approach include: (1) older than 8 years of age (2) severe deformity with significant cosmetic and functional disability (3) anteversion in excess of 50 degrees (4) deformity more than 3 STD beyond the mean (5) a family who is aware of the risks of the procedure n The derotation osteotomy at the proximal femur n One must carefully consider the relative cosmetic effect of intoeing versus the surgical scars required for femoral derotation
")
1. Protective in-toeing – In developmental genu valgum and flat foot (flexible pes planovalgus) • 2. child is shifting the center of gravity to the foot center Neuromuscular (all ages) – Spasticity of ant and/or post tibial muscles – hip med rotators and hip adductors

Metatarsus adductus Internal Tibial Torsion Femoral Anteversion Age 4 -12 Months 1 -2 Years 3 -6 Years Natural History 85% Resolve Spontaneously 99% Resolve Spontaneously Most Resolve Spontaneously Normal Values Heel Bisector Between Toes 2 and 3 5 degree external 45 degree-Newborn 20 degree 32 degree-Age 1 Year external-Adult 15 degree-Adult Problems Cosmesis Shoe Wear Foot Pain if Severe and Rigid Usually None Cosmesis Occasionally Knee Pain Early Tr. Seria Manipulation and Casts None Treatment-Late for Persistent Deformity Mid-foot osteotomy or Metatarsal Osteotomy Derotational Osteotomy (Supra-Malleolar) Derotational Osteotomy (Intertrochanteric

Out-toeing n n n less common than intoeing Its causes are similar but opposite to those of in-toeing Toddlers may walk with outtoeing due to – external rotation contracture of newborn hips – decreased femoral anteversion n n The contracture of external hip rotators typically resolves within 1 year after ambulation Outtoeing after age 2 is probably due to – decreased femoral anteversion – to external tibial torsion n Both typically resolve spontaneously, but may take up to 8 years

Femoral Retroversion – Common in early infancy – Unilateral, R side > L side – More common in obese children – apparent when the pre-walking child stands with his or her feet turned out to nearly 90 degrees ("Charlie Chaplin appearance") – It may gradually improve on its own during the first year of walking

Femoral Retroversion –Nonoperative treatment is ineffective – Tx ultimately surgical if required – Refer if: • >3 yrs old (higher risk osteoarthritis in hip, stress fracture, SCFE)

External Femoral Torsion

External Tibial Torsion n n usually seen between 4 to 7 years of age often unilateral and more common on the right side Disability from lateral tibial torsion is usually caused by PF instability and pain Refer if: – >10 yrs old – severe deformity (thigh-foot angle >40°) – pain

n Lateral tibial torsion is a more common indication for osteotomy than internal torsion n Surgery has a high complication rate n Should not be done until after the child is more than 10 years of age n Deformity should be severe – a thigh-foot angle of more than 40 degrees
 common in children – arch development primarily")
Flat Feet n (pes planus, pes planovalgus) common in children – arch development primarily before four years of age with a wide variation in the rate or onset n n The most common etiology of the flexible flat foot is ligamentous laxity, Test for Flexibility: – arch reconstruction • on toe standing • foot is dependent – hanging over the examination table n No treatment is indicated for painless flexible flat foot

n foot rolls out: – abnormal wear on the inner side of the shoe n No pain except – an older child or adolescent with severe flatfoot after excessive standing or walking n significant pain is a warning signal – often associated with • peroneal muscle spasm • a rigid flatfoot

Assessment of the child's shoes should be done. Shoe wear patterns can give an excellent clue to the severity of the condition.

Classification of Flat foot Flexible 1. Idiopathic 2. Familial 3. Secondary to tight heel cord 4. Ligamentous Hyperlaxity-Connective Tissue Disorders a. Marfan's Syndrome b. Down's Syndrome c. Ehlers-Danlos Syndrome 5. Neuromuscular a. C. P. b. Polio c. Muscle disease d. Peripheral nerve injury Rigid 1. Tarsal Coalition 2. Arthritis a. Inflammatory b. Traumatic 3. Congenital convex pes valgus-vertical talus 4. Infection 5. Neoplasm

Flexible Flat Foot n n n usually caused by laxity of ligaments in the foot idiopathic or familial in origin Increased angulation between the talus and the os calcis in weight-bearing AP and lateral planes

Cause of A Stiff And Painful Flat Foot n n n n Trauma Juvenile rheumatoid arthritis Occult infection A foreign body Congenital vertical talus Tarsal coalition Bone tumors Osteochondrosis of the tarsal navicular bone

n It is now recognized that the vast majority of mild to moderate flexible flatfeet do not require any treatment parental reassurance

Treatment Principles n The longitudinal arch of children under the age of three years is often filled with a fat pad that does not disappear until this age n No type of shoe support or orthosis will produce a lasting structural improvement in a flatfoot. n No therapy is for a mild or moderate flexible flatfoot n Exercise programs for foot or leg muscles (other than for a tight heelcord) have no therapeutic value

Treatment Principles n Flatfoot in the older child with discomfort – treated with a scaphoid pad and one eighth inch medial heel wedge for relief of pain n Severe flexible flatfoot with heel valgus and no underlying neurologic or muscular disorder – a foot orthosis n Rigid flat feet – orthopaedic evaluation and management

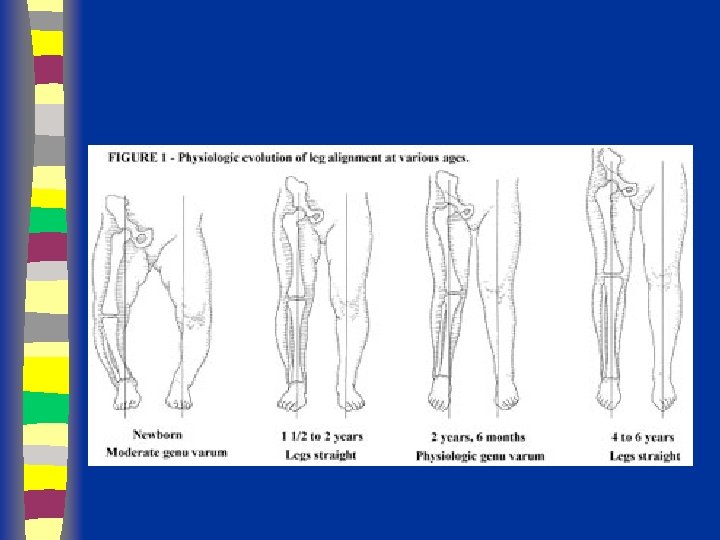
Angular Variations n Many children will Look – bowlegged when they start to walk – knock-kneed between three to seven years n The gradual change from varum to valgum may be caused by a widening pelvis n Genu varum (bowlegs) is seen from birth until two years of age, while genu valgum (knock-knees) peaks from two to four years

Angular Deformities Evaluation Should differentiate between “physiologic” and pathologic” deformities

Angular Deformities Evaluation Physiologic • Symmetrical • Mild – moderate • Regressive • Generalized • Expected for age Pathologic • Asymmetrical • Severe • Progressive • Localized • Not expected for age

The Natural History Of The Tibial Femoral Angle n At birth, – approximately 15 degrees of genu varum n At one and one-half to two years of age – Gradual spontaneous correction to zero degrees n During the next year – a valgus of 10 degrees to 12 degrees n Gradually correction to the normal adult value – 5 to 6 degrees valgus at about age 7 years n This process is identical in boys and girls.

n The most common reason – physiologic or a normal developmental variation n serial measurement of intercondylar /intermalleolar distance to document gradual spontaneous resolution
 in bow")
Angular Deformities Evaluation Physical Examination Measure Angulation ( standing / supine ) in bow legs / genu varum Inter-condylar distance
 in knock")
Angular Deformities Evaluation Physical Examination Measure Angulation ( standing / supine ) in knock knees /genu valgum Inter-malleolar distance

n A more accurate measurement would be the tibial femoral angle as seen on the standing x-ray n One must be careful that the legs are in neutral rotation when the x-ray is taken, – internal or external rotation will alter this angle. n Internal tibial torsion and external rotation contracture of the hips – accompany genu varum • accentuate the deformity.

Differential Diagnosis for Genu Varum and Genu Valgum n Genu varum – Physiologic bowlegs – Infantile tibia vara – Hypophosphatemic rickets – Metaphyseal chondrodysplasia – Focal fibrocartilaginous dysplasia n Genu valgum – Hypophosphatemic rickets – Previous metaphyseal fracture of the proximal tibia – Multiple epiphyseal dysplasia – Pseudoachondroplasia
 n n Many infants are born with mild bowleg deformities known")
Bowlegs (Genu Varum) n n Many infants are born with mild bowleg deformities known as “physiologic genu varum” Torsion of the lower extremity long bones can affect the “appearance” of angulation

Treatment n n n reassurance Observation Shoe corrections, splints and exercise not programs do produce any change different than the normal expected spontaneous correction

Angular Deformities When To Refer ? n Pathologic deformities Asymmetrical Localized Progressive Not expected for age Severe n Exasurated physiologic deformities

Non-physiologic Conditions Causing Genu Varum n Blount’s disease – Infantile tibia vara – Late-onset (adolescent) tibia vara n Osteodystrophy – Vitamin-D-resistant rickets – Hypophosphatasia n Bone dysplasia – Achondroplasia – Metaphyseal dysplasia n Trauma – Proximal tibial or distal femoral partial physeal arrest n Tumors – Osteochondroma – Focal fibrocartilaginous dysplasia of distal – femur/proximal tibia n Congenital anomalies – Congenital longitudinal deficiency of the tibia
 n n n Between the ages of 2. 5 and")
Knock Knees (Genu Valgum) n n n Between the ages of 2. 5 and 5 years, many normal children develop significant genu valgum The peak physiologic valgus angulation was 12° ± 8° at this age Parents reassurance if: – Child has normal stature – Symmetrical genu valgum <15° – And an intermalleolar distance = 8 cm n Full-length lower extremity a-p roentgenograms should be reserved for children who do not meet these criteria.

n n Physiologic genu valgum rarely requires treatment. Shoe wedges are ineffective, and long leg braces are rarely appropriate Knee valgus more than 15 degrees can cause medial foot strain, synovitis of the knee joint, patello-femoral instability, and gait abnormalities. Surgical treatment (hemi-epiphysiodesis) is typically performed only for those rare children with >15° genu valgum (mechanical axis) after adolescence

n Treatment for significant physiologic genu valgum may commence as soon as one is sure that spontaneous correction is not occurring n This usually will be after age 5 years n Initially, a knock knee brace may be tried at night time and for most of the day. n If the deformity persists, – a medial epiphyseal stapling or epiphyseodesis • if there is sufficient growth potential for correction (usually at a skeletal age of 10 in girls and 11 in boys). n This is most often performed in the distal femur, but can be done in the proximal tibia if the deformity appears to be arising there.

Angular Deformities

n Progressive or asymmetrical genu valgum usually suggests the presence of a non-physiologic condition n Osteodystrophy – Vitamin D-resistant rickets – Renal osteodystrophy n Bone dysplasia – Pseudoachondroplasia – Multiple epiphyseal dysplasia – Morquio’s mucopolysaccharidosis n Trauma – Proximal tibia medial metaphyseal fracture with – malunion / overgrowth – Proximal tibial or distal femoral partial physeal arrest n Tumors – Osteochondroma – Focal fibrocartilaginous dysplasia of distal – femur/proximal tibia n Congenital anomalies – Congenital femoral hypoplasia – Congenital longitudinal deficiency of the fibula – Congenital or developmental coxa vara n Neuromuscular – Myelomeningocele – Polio – Iliotibial band contracture

n A fairly common form of progressive unilateral genu valgum occurs after fracture of the proximal tibial metaphysis in children aged 2 -8 years n Tibial overgrowth may result in up to 10° additional valgus angulation within one year after injury n This asymmetry typically resolves significantly without treatment by adolescence. n Treatment consists of a corrective osteotomy if the deformity does not remodel in 2 to 3 years.
- Slides: 88