Pediatric Hip Dr Fadel Naim Orthopedic Surgeon IUG

")

 n DDH is a term used to describe")







 Feel a Clunk Not hear a click !")
")

 n n n restricted abduction at the")












")

























 Established dislocation (reducible) n n n")










 is a childhood hip disorder that results in infarction of")



 Initial stage – 2) Fragmentation stage")








")
 no lateral pillar involvment – B)")

 to reduce")























")


- Slides: 110
Pediatric Hip Dr. Fadel Naim Orthopedic Surgeon IUG
Developmental Dysplasia of the Hip ( DDH )
The main aim of this presentation is to: – emphasize the importance of the early identification of DDH – The earlier an abnormality of the infant hip is detected, the simpler and more effective the treatment will be
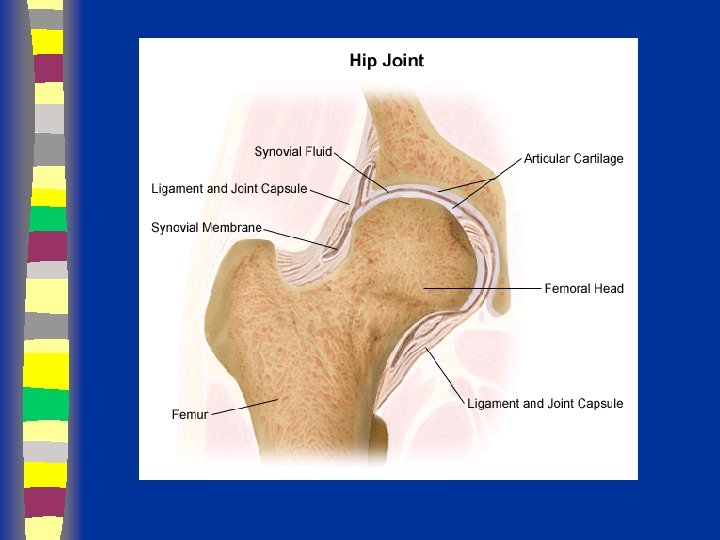
Developmental Dysplasia of the Hip (DDH) n DDH is a term used to describe a spectrum of abnormalities affecting the relationship of the femoral head to the acetabulum. – an immature hip – a hip with mild acetabular dysplasia – a hip that is dislocatable – a hip that is subluxated – a hip that is frankly dislocated.
n Teratologic Hip : Fixed dislocation Occurrs prenatally Often with other anomalies n Dislocated Hip : Completely out May or may not be reducible n Subluxated Hip : Only partially in n Unstable Hip n Acetabular Dysplasia : Shallow Acetabulu : Femoral head can be dislocated Head Subluxated or in place
Epidemiology n 1 in 100 newborns examined have evidence of instability ( positive Barlow or Ortolani) n 1 in 1000 live births true dislocation n most detectable at birth in nursery n 60% stabilize in 1 st week and 88% stabilize in first 2 months without treatment remaining 12% true dislocations and persist without treatment
Risk Factors associated with DDH n n Breech Presentation Family History of DDH (especially if in parent or sibling) Female Baby (DDH is 4 X likely to occur in a female infant) Postnatal Positioning
Risk Factors associated with DDH n n Breech Presentation Family History of DDH (especially if in parent or sibling) Female Baby (DDH is 4 X likely to occur in a female infant) Postnatal Positioning
Risk Factors associated with DDH n decreased intrauterine space – – Large Baby (>4 kg) Overdue > 42 weeks Oligohydramnios Associated with Plagiocephaly, Torticollis and foot deformities – First born baby or multiple pregnancies
PHYSICAL EXAMINATION n The reliability of physical examination changes as the child grows, therefore examination techniques vary depending on the age of the child.
Diagnosis n n Clinical risk factors Physical exam – Ortolani Test – Barlow Test
Neonatal Examination Ortolani (reduction test) Feel a Clunk Not hear a click !
Neonatal Examination Barlow (stress test)
n Ortolani and Barlow tests are accurate within the first 48 hours of birth and then become increasingly less accurate. – Thus Hip examination ideally should be performed within 48 hours n After 3 months of age, the Ortolani and Barlow tests may be unreliable – therefore additional means of examination, used in combination with the Ortolani and Barlow tests, are necessary
Older Infants (> 3 months of age) n n n restricted abduction at the hips leg length discrepancy asymmetrical thigh and gluteal skin folds
Restricted Abduction At The Hips n n n The most sensitive sign associated with DDH in the older infant. The examination should be performed gradually and may need to be repeated a number of times Normal range of motion at the hip is abduction to 60˚ or more, with range less than this suggestive of DDH.
Leg Length Discrepancy n n Total leg length discrepancy should be assessed in prone with hips and knees extended assessing for leg length discrepancy using the Galeazzi Test.
Asymmetrical Skin Folds n n Asymmetrical skin folds alone do not constitute a diagnosis of DDH However this information can be used in combination with other physical signs during assessment.
Bilateral Dislocation n Diagnosis more diffecult – Abduction may be decreased symmetrically with bilateral dislocations. – Galeazzi Test may be negative in bilateral dislocations – There may be no asymmetrical skin folds
Klisic test n An imaginary line between anterior superior iliac spine and great trochanter should point towards or above the umbilicus. – If dislocated will point below
Late Signs n In children who are walking – a limp may be present – the child may toe-walk on the affected side. n If DDH is present in both hips – increased lumbar lordosis – prominent buttocks – a waddling gait
Ultrasound n n n Morphologic and dynamic assessment Indications controversial due to high levels of over-diagnosis Currently not recommended as a routine screening tool other than in high risk patients
Ultrasound
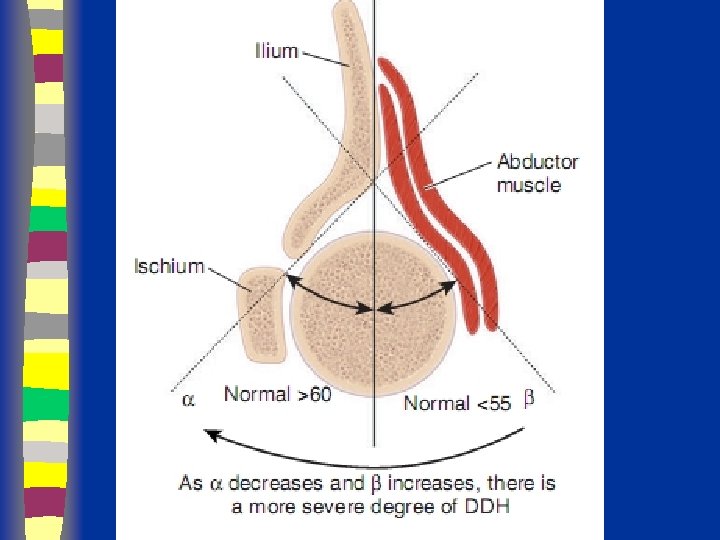
Ultrasound Femoral head Abductors Ilium
Ultrasound Femoral head Abductors Ilium
Ultrasound Femoral head Abductors Ilium
Ultrasound Graf’s alpha angle >60 = normal *line w/ ilium bisects head 50/50
n If the child is 6 weeks to 5 months of age, Ultrasound (US) is generally the most appropriate imaging technique n If the child is 5 months or greater, X-ray is generally the most appropriate imaging technique n Between 4 and 6 months, US and X-ray are equally effective diagnostic tools
Radiography
Radiographs Summary § § § Femoral head appears 4 - 7 months Shenton’s line Perkin’s and Hilgenreiner’s lines § Inferomedial quadrant § Acetabular index § Normal < 30 (Weintroub et al)
Radiography
Radiological Diagnosis X-ray findings • • • Delayed appearance of ossific nucleus Small ossific nucleus Dysplastic acetabulum Proximal displacement of femur Increased acetabular index ( n=27, >30 -35 dysplasia) • Disruption Shenton line
Radiography
Radiography
Radiography in out
Radiography 27 o 39 o
Imaging
Imaging
Imaging
Imaging
Imaging
Imaging
Imaging < 30 wnl
Imaging
Imaging
Imaging
Imaging
Treatment Options § § § Age of patient at presentation Family factors Reducibility of hip Stability after reduction Amount of acetabular dysplasia
Treatment n The presence of the spherical femoral head within the acetabulum is critical for stimulating normal development of the acetabulum n Aims – Obtain and Maintain concentric reduction – In an Atruamatic fashion – Without disrupting the blood supply
Treatment n Method depends on Age n The earlier started, the easier the treatment n The earlier started, the better the results n Should be detected EARLY
Treatment n n n Birth to 6 months : Pavlik harness or hip spica cast 6 months – 12 months : closed reduction UGA and hip spica casts 12 months – 18 months : possible closed / possible open reduction Above 18 months : open reduction and ? Acetabuloplasty Above 2 years : open reduction, acetabulplasty, and femoral osteotomy Above 8 years : open reduction, acetabulplasty cutting three bones, and femoral osteotomy
Treatment Hip instability in the neonatal period Most resolve spontaneously n n n Observation Pavlik harness Double /triple diapers ? ?
Treatment Hip instability in the neonatal period Double / Triple Diapers n n n Often inadequate : therefore inappropriate Gives illusion patient is in “treatment” while wasting valuable time Most hip instability improves spontaneously in early infancy , giving this ineffective management credit
Treatment Birth – 6 months Hip instability (dislocatable) Established dislocation (reducible) n n n Should be actively treated until hip is normal clinically and radiographically Pavlik harness Hip Spica Cast
Treatment Birth – 6 months Pavlik harness
Treatment Birth – 6 months Other Devices - Frejka pillow - Craig - Von Rosen splint Soft abduction splints: Not good enough Rigid abduction splints: Risk AVN
Treatment 6 – 12 months n n n Initially non operative – closed reduction Reduction under anesthesia and immobilization in hip spica cast Position: Human Avoid severe abduction Avoid Frog position n Must be stable and concentrically reduced otherwise needs open reduction
Treatment Above 18 months n Open reduction ? and acetabulplasty ? And femoral shortening – if high
Treatment Above 3 years n Open reduction n And acetabulplasty n And femoral shortening
Salter Osteotomy
Redirectional Acetabuloplasty Salter’s
Adolescent or Adult n Femoral osteotomy should only be used in conjunction with pelvic procedure as no potential for acetabular growth or remodeling but changing orientation of femur shifts the weight-bearing portion
Complications of Treatment n n n Worst complication is disturbance of growth in proximal femur including the epiphysis and physeal plate AVN may be due to vascular insults to epiphysis or physeal plate or pressure injury “ frog leg position “ uniformly results in proximal growth disturbance
Legg Calve Perthes Disease Prepared by Dr fadel Naim MD Orthopedic surgeon 66
n Legg-Calvé-Perthes disease (LPD) is a childhood hip disorder that results in infarction of the bony epiphysis of the femoral head. n LPD represents idiopathic avascular necrosis of the femoral head. 67
Epidemiology n Disorder of the hip in young children n Usually ages 4 -8 yo As early as 2 yo, as late as teens Boys: Girls= 4 -5: 1 Bilateral 10 -12% No evidence of inheritance incidence of positive family hx ranges from 1. 6% to 20% n n n 68
Etiology n n n Unknown Past theories: infection, inflammation, trauma, congenital Most current theories involve vascular compromise 69
Pathophysiology n The primary pathologic abnormality is osteonecrosis resulting in flattening and collapse of the femoral head. n The basic underlying cause of LPD is insufficient blood supply to the femoral head. n Healing occurs by revascularization of the necrotic femoral head. 70
Radiographic Stages n Four Waldenstrom stages: – 1) Initial stage – 2) Fragmentation stage – 3) Reossification stage – 4) Healed stage 71
Initial Stage n Early radiographic signs: – Widening of medial joint space – “Crescent sign” – Irregular physeal plate – Blurry/ radiolucent metaphysis 72
73
Fragmentation Stage n Bony epiphysis begins to fragment 74
Reossification Stage 75
Presentation n n Often insidious onset of a limp C/O pain in groin, thigh, knee 17% relate trauma hx Can have an acute onset 76
Legg-Calve-Perthes Disease n n n n CLINICAL FINDINGS Prolonged limp Waddling gait Pain in groin or thigh Limited painful motion Tenderness to palpation over hip Gluteal Atrophy Trendelenberg sign Positive Leg Length Discrepancy
Physical Exam Decreased ROM, especially abduction and internal rotation n Adductor contracture n Trendelenburg test often positive n Muscular atrophy of thigh/buttock/calf n Limb length discrepency n 78
Imaging n n n AP pelvis Frog leg lateral Key= view films sequentially over course of dz Arthrography MRI 79
Differential Diagnosis n n Important to rule out infectious etiology (septic arthritis, toxic synovitis) Others: – Chondrolysis – JRA – Osteomyelitis – Lymphoma -Neoplasm -Sickle Cell -Traumatic AVN -Medication 80
Lateral Pillar Classification n 3 groups: – A) no lateral pillar involvment – B) >50% lat height intact – C) <50% lat height intact 81
Prognosis n n 60% of kids do well without tx AGE is key prognostic factor: – <6 yo= good outcome regardless of tx – 6 -8 yo= not always good results with just containment – >9 yo= containment option is questionable, poorer prognosis, significant residual defect n Flat femoral head incongruent with acetabulum= worst prognosis 82
The Goal of Treatment n The goal of treatment is four-fold: I) to reduce hip irritability 2) restore and maintain hip mobility 3) to prevent the ball from extruding or collapsing 4) to regain a spherical femoral head 83
Non-operative Tx n Improve ROM 1 st –-abduction usually affected most of ROM – -use PT to regain abduction (overcome spasm) and internal rotation – -may require several weeks of abduction traction 84
Non-operative Tx n Bracing: – Removable abduction orthosis – Pietrie casts – Hips abducted and internally rotated n n n Not necessarily NWB Hips braced in abd/ int rotation to transmit weight over wide area of acetabulum, prevents head collapse Wean from brace when improved x-ray healing signs 85
Bracing 86
Non-operative Tx n Check serial radiographs – Q 3 -4 mos with ROM testing n Continue bracing until: – Lateral column ossifies – Sclerotic areas in epiphysis gone n Cast/brace uninvolved side 87
Operative Tx n n If non-op tx cannot maintain containment Surgically ideal pt: – 6 -9 yo – Catterral II-III – Good ROM – In collapsing phase 88
Surgical Tx n Surgical options: – Excise lat extruding head portion to stop hinging abduction – Acetabular (innominate) osteotomy to cover head – Varus femoral osteotomy – Arthrodesis 89
Late Effects of LCP n n Coxa magna Physeal arrest patterns Irregular head formation Osteochondritis dessicans 91
SCFE
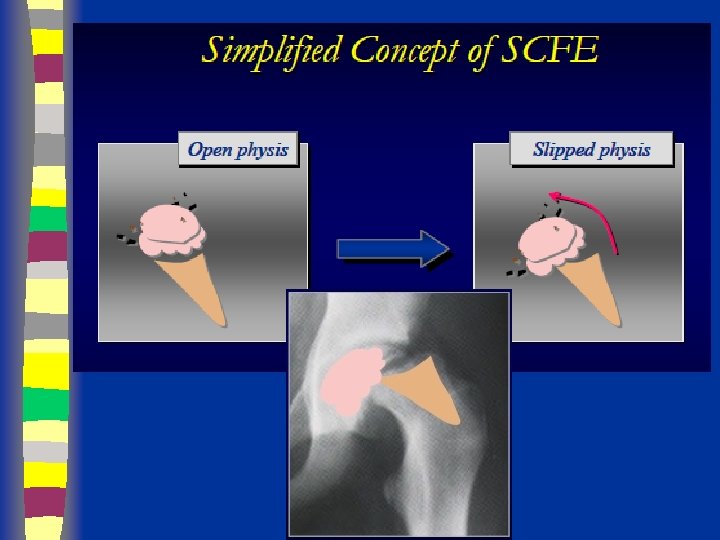
Definition n The femoral neck and shaft displace upward anteriorly on the capital epiphysis, which displaces primarily posteriorly relative to the femoral neck
Classification n According to the onset: 1 -acute 2 -chronic 3 -acute on chronic n According to ability to bear weight: 1 -stable 2 -unstable n According to the displacement extent: 1 -mild 2 -moderate 3 -severe
Etiology • Endocrine – Hypothyroid – Growth hormone treatment • Mechanical – 63% > 95 th percentile weight
Klein’s Line
GRADING n. Grade III
GRADE I < 1/3 Slip
Grade II
GRADING Grade III
Frog Pelvis Radiograph Posterior slip n Wide, irregular physis n
Pre-Op
Early Post-Op
Post-Op (14 y/o)
COMPLICATIONS n n AVN Chondrolysis Hardware Penetration Long-term results are dependent upon avoiding these complications
Thank you for attention