Neuromuscular Disorders Dr Fadel Naim Orthopedic Surgion IUG




 • Prenatal (44%) n First trimester")
 • Causes • Labor and delivery")

 • Type")


















- Slides: 29
Neuromuscular Disorders Dr. Fadel Naim Orthopedic Surgion IUG
Cerebral Palsy • Umbrella term covering – A group of non-progressive, but often changing, motor impairment syndromes secondary to lesions or anomalies of the brain arising in the early stages of its development
• The definition of cerebral palsy stress followed features: – Result of a lesion in the immature brain, which is nonprogressive • It is a static encephalopathy – Results in a disorder of posture and movement which is permanent but not unchanging • (progressive musculoskeletal pathology in most affected children)
Etiology • Variety of perinatal, prenatal, and postnatal factors contribute, either singly or multifactorily to CP. • Commonly thought to be due to birth asphyxia; Now known to be due to existing prenatal brain abnormalities. • Premature delivery is the single most important determinant of CP. • In 24% of cases, no cause is found.
Causes of CP • Time (% of cases) • Prenatal (44%) n First trimester n Second trimester • Causes • Teratogens, chromosomal abnormalities, genetic syndromes, brain malformations • Intrauterine infections, problems in fetal/placental functioning
Causes of CP • Time (% of cases) • Causes • Labor and delivery (19%) • Preeclampsia, complications of labor and delivery • Perinatal (8%) • Sepsis/CNS infection, asphyxia, prematurity • Childhood (5%) • Meningitis, traumatic brain injury, toxins • Not obvious (24%)
Classification • Cerebral palsy can be classified according to: n n n Pathology of brain injury e. G. Vascular, infective, inflammatory or traumatic The timing of brain injury such as prenatal, perinatal or postnatal The modified swedish clasification is the widely used classification which is based on the tone, number and distribution of the affected limbs
• Pattern of involvement : Diplegia Hemiplegia Triplegia Quadriplegia (total body) • Type of motor dysfunction : Spastic / Ataxic / Mixed / Athetoid / hypotonic 65% 5% 12% 10% 1%
• The spastic variety is the most common, with mixed varieties now being increasingly diagnosed • The clinical spectrum of CP ranges from: – very minor impairment • Patient with mild hemiplegia with minimal gait deviations – Significant cognitive deficits and motor functional limitations • Children with severe total body involvement
Spastic Form • Most common form of cerebral palsy affecting about 70 -80% of all people with the condition • Results from damage of the motor cortex • Spastic CP can be broken up into 3 subtypes: (1) hemiplegia, affecting one side, (2) diplegia, affecting both arms or both legs, (3) quadriplegia affecting all limbs
Athetoid Form • uncontrolled motion, especially in the face, arms and trunk • Interfering with any skill, which requires coordinated movements – speaking, feeding, reaching, grabbing • Damage to the cerebellum • Mixed muscle tone • The child may develop purposeless, involuntary movements. • May increase due to stress and disappear during sleep
Ataxic Form • Poor balance resulting in stumbles and falls • Damage to the cerebellum • May have tremors that worsen when reach for objects • Ataxic CP only accounts for 10% of individuals with the condition
Mixed Forms • Mixed forms of cerebral palsy are also fairly common, occurring in 25% of people with cerebral palsy • Damage to both the motor cortex and the cerebellum • Both spastic muscle tone and involuntary movements • They may also have low muscle tone in some muscles and high tone in others
Spasticity Treatment Modalities 1. 2. 3. 4. 5. 6. Physical Therapy Orthotic Devices Oral Muscle Relaxants Intramuscular Injections Intrathecal Baclofen (ITB) Selective Dorsal Rhizotomy (SDR)
Orthopedic Problems • An extensive musculoskeletal system examination needs to be performed in children with cerebral palsy looking for evidence of: n n n Osteopenia Hip subluxation Scoliosis Contractures of hamstring muscles and tendo achilles Equinus deformity Foot deformity • In ambulatory children observation of gait in the clinic provides useful information about coordination and musculoskeletal abnormalities;
• Treatment is focused during the early years of growth on: Tone management n Prevention of contractures n Aids for walking n Multilevel bony and soft-tissue surgery to improve gait n
General principles of orth. management • Lengthening a spastic muscle can improve its function by diminishing the overactive stretch response and uncovering any control that was present • Surgery should not be reserved for patients with severe impairment and deformity. • The amount of improvement correlates best with the degree of underlying motor control and not with the severity of the deformity • Individuals with milder degrees of impairment can benefit greatly from relatively simple procedures
General principles “functional” and “nonfunctional” surgical procedures Ø Musculoskeletal surgery aims are classified as hygienic or functional Ø These terms refer to the expected outcomes for a limb but do not indicate the outcome for the person as a whole. Ø Surgical releases of an arm contracted in a flexed and internally rotated position in a hemiplegic patient often allows the person to become independent in dressing, even though the arm itself remains nonfunctional
“Birthday surgery” • Should be avoided in favor of simultaneous multilevel surgery. – A and B, Young child with diplegia and toe-walking (A) undergoes isolated heel cord lengthening, which increases crouch gait (B) – C, One year later, he has isolated hamstring lengthening and develops hip flexion contracture. – D, One year later, he has hip flexor release to allow him to ambulate in upright position.
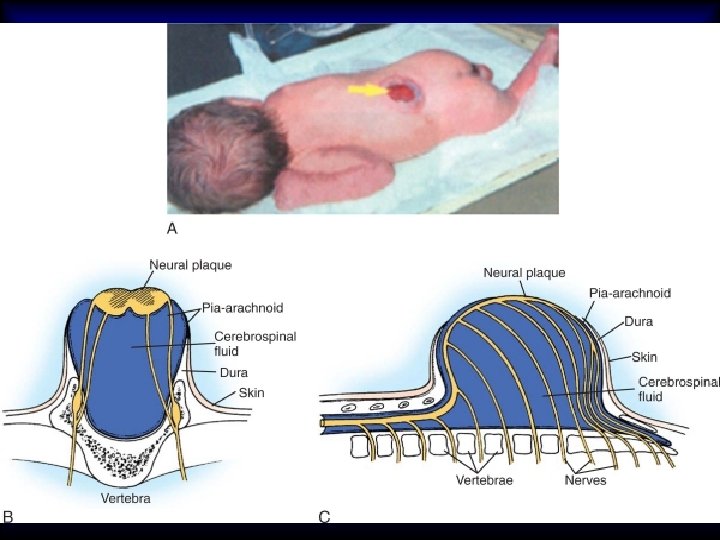
Spina Bifida • Incomplete closure of the laminar arches of the spine • Occurs at birth but may not be detected until later • An unrelated variety, spina bifida occulta, is a small defect in the 5 th lumbar or 1 st sacral arches, a benign finding of no clinical consequence.
• To prevent meningitis, the lesion should be closed immediately and associated hydrocephalus controlled by ventriculoperitoneal shunting procedures
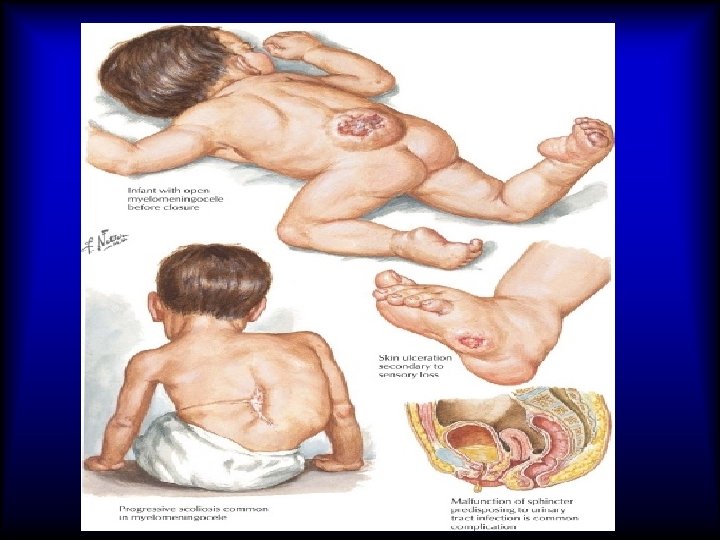
Spina Bifida • May be a clinically significant problem if it is associated with congenital neurologic deficit at the open bony levels • May occur at any level of the spine or at multiple levels, although it is most common at the caudal aspect of the spine • In the presence of a neurologic deficit, secondary problems may develop in the genitourinary tract and lower limbs.
Classification: • Spina bifida occulta: – Skin-covered defect in the lower lumbar spine with no neurologic deficit – associated with slightly increased risk of spondylolisthesis • Myelomeningocele: – Combination of several absent laminae, with exposed meninges and usually neurologic deficit at the same level – High risk of hydrocephalus
• Lipomeningocele: – Caudal fatty mass arising from the spinal canal – palpable under the skin – with an associated neurologic deficit – no substantial risk of hydrocephalus
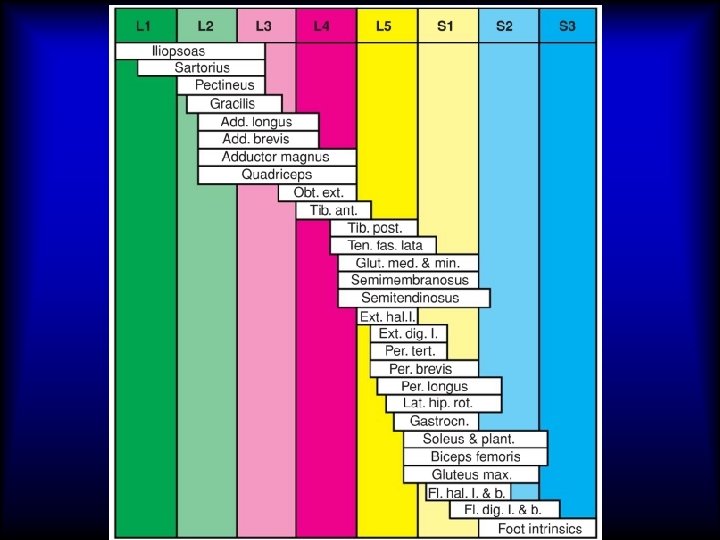
• The most commonly used classification of myelomeningocele is based on the neurological level of the lesion – thoracic level (no L 1 to S 4 function) – upper lumbar level (intact to L 1 or L 2) – lower lumbar level (intact to L 3 or L 4) – sacral level (intact to L 5 or S 1)
• A comprehensive team approach is optimal because patients frequently have multisystem pathology that involves developmental delay, bowel and bladder dysfunction, and progressive joint contractures and bony deformities.