Oral and Maxillofacial Radiology for the Child Juan



 Smithsonian American Art")




: it is used to compare the")






")



 ALARA:")


















 originating at different")























- Slides: 64
Oral and Maxillofacial Radiology for the Child Juan F. Yepes DDS, MD, MPH, MS, Dr. PH
Introduction
Radiation Safety and Protection http: //www. pedrad. org/associations/5364/ig/
Radiation…. Who cares? People in the Sun (Edward Hopper 1882 -1967) Smithsonian American Art Museum
Radiation…. Who cares? Photos by GEORGE STEINMETZ and Google images
Radiation…. Who cares? www. webmd. com/melanoma-skin-cancer/slideshow
Antepartum dental radiography and Infant low birth weight Potential mothers Chronic exposure to radiation (stochastic) Develop subclinical hypothyroidism Got pregnant Delivery babies with LBW “ 374 CT scans in 1 year 992 m. Sv / year” 3. 6 m. Sv annual dose
Radiation Worries For Children in Dentist’ Chairs CBCT increases productive and generate more profit http: //video. nytimes. com/video/2010/11/22/us/1248069363524/the-price-of-a-smile. html
Radiation Safety and Protection Dosimetry Equivalent dose (Ht): it is used to compare the biological effects of different types of radiation to a tissue or organ. It is the sum of the products of the absorbed dose (Dt) averaged over a tissue or organ and the radiation weighting factor (Wr) depends on the type of radiation Ht = Σ Wr x Dt IS Unit sievert (Sv) Traditional unit rem 1 Sv = 100 rem
Radiation Safety and Protection Sources of Radiation Exposure Natural Radiation Cosmic Sources Subatomic particles and photons from the sun. It is primarily a function of altitude Sea level: 0. 24 m. Sv / Year Denver (Colorado): 0. 50 m. Sv/Year Exposure resulting from airline travel 5 hours flight: 25µSv
Radiation Safety and Protection Natural Radiation Cosmic Terrestrial Sources External Radiation: Radioactive nuclides in the soil, primarily potassium 40 and the radioactive decay products of uranium 238, and thorium 232 (0. 5 m. Sv / year) Radon: Radon is a decay product in the uranium series. It is responsible of 52% of the radiation exposure of the world’s population (1. 2 m. Sv/Year). It is a GAS attached to dust particles LUNGS Other Internal: Ingestion of uranium
Radiation Safety and Protection
Radiation Safety and Protection Man-Made Radiation Medical Diagnosis and Treatment Well over one billion medical x-ray examinations are performed annually worldwide. Dentistry is responsible for less than 1% of the man-made sources of radiation Consumer and Industrial Products Domestic water supply, tobacco products, combustible fuels, dental porcelain, television receivers, pocket watches, smoke alarms, and airport inspection systems.
Radiation Safety and Protection Cosmic Natural Sources of Radiation Exposure 83% (3 m. Sv / year) Terrestrial radon 3. 6 m. Sv / year Artificial Internal 17% (0. 6 m. Sv / year) Ingestion of food 2. 4 m. Sv
Radiation Safety and Protection From EPA website
Radiation Safety and Protection Medical x-ray 0. 39 m. Sv (2. 5% dental x-rays) 3. 6 m. Sv 2. 4 m. Sv / Year
Radiation Safety and Protection Dose and Risk in Radiology The NCRP and the ICRP established guidelines for limitations on the amount of radiation received by both occupationally exposed Individuals and the public. Dose Limits There are no limits on the exposure a patient can receive from diagnostic or therapeutic exposures. Dentist and their staff are occupationally exposed workers no more than 50 m. Sv/Year
Radiation Safety and Protection Effective Dose from Diagnostic Radiology and equivalent background Examination Effective Dose (m. Sv) Equivalent background radiation (days) Intraoral Posterior BW (F-speed) (rectangular collimation) 0. 005 0. 6 FMX (rectangular c. ) FMX (round collimation) 0. 035 0. 171 4 21 Panoramic Cephalometric 0. 009 -0. 026 0. 003 -0. 066 1 -3 0. 5 -1 CBCT I-CAT® (extended 0. 235 29 CT Head 2 243 Extraoral view) Background radiation: 3. 6 m. Sv / year
Radiation Safety and Protection Risk Estimates • The primary risk from dental radiography is radiation-induced cancer (stochastic ) • The risk for cancer being induced in human as a result of exposure to low doses of radiation is difficult to estimate for different reasons: - The data for the cancer risk from radiation exposure involve exposures many times larger than dental radiology - Cancer is a common disease. It is difficult to detected the effect of dental radiography - The time between the radiation exposure and the development of cancer may be years to decades.
Radiation Safety and Protection Dosimetry Dose Limits NCRP and ICRP (private nonprofit organizations) ALARA: As low As Reasonable Achievable Maximum Permissible Dose (MPD) for occupationally exposed workers NCRP: ICRP: 50 m. Sv/yr
Radiation Safety and Protection Thyroid • Intraoral – full mouth survey with round collimation is 0. 94 m. Sv; the same study with rectangular collimation results in a dose of 0. 26 m. Sv • Panoramic Radiograph 0. 11 m. Sv
Radiation Safety and Protection Reducing Dental Exposure
Radiation Safety and Protection Patient Selection Criteria • Little evidence to support radiographic exposure of all edentulous areas of the oral cavity. • Clinical evaluation + Combined selected periapical radiographs can result in a 43% reduction in the number of films without a clinical consequential increase in the rate of undiagnosed disease. • ADA and FDA developed guidelines for the selection of patients for dental radiographic examination.
Radiation Safety and Protection Patient Selection Criteria Radiographs must be limited to the areas required for adequate diagnosis and treatment based on professional judgment Dentist should not prescribe routine radiographs at preset intervals for all patients For new or referred patients, clinicians should obtain recent dental radiographs from the patient’s previous dental health care provider Dental radiographs my be prescribed for pregnant patients with careful adherence to the radiation safety protocols Dentist should prescribe dental radiographs ONLY after clinical evaluation
Patient Protective Equipment • Leaded aprons and thyroid shields that contain lead or other materials are patient – protective equipment. • If all the NCRP recommendations are followed rigorously, the use of lead apron on patients is not required. (1) • Thyroid shielding with a leaded thyroid shield or collar is strongly recommended for children and pregnant women. (2) • Thyroid collars are also recommended for adults when it will not interfere with the exposure. (1) • To prevent cracks in the leaded shield, practitioners should enforce that leaded aprons and collars are hung and not folded (1) National Council for Radiation Protection & Measurements; 2003 (2) US Department of Health and Human Services, Public Health Service, FDA and American Dental Association Council of Scientific Affairs, 2004
Patient Protective Equipment
Radiation Safety and Protection of the Personnel Radiation Safety Procedures • If leaving the room or making use of some other barrier is impossible, strict adherence to POSITION DISTANCE RULE is mandatory 6 feet ADA: Council of Scientific Affairs 2006 6 feet Except: New Mexico
Selection Criteria -Exposing radiographs in asymptomatic children -Development of the dentition as criterion -Risk of caries as criterion -Radiographic examination
Selection Criteria • The stage of dentition development • The risk of dental caries
Selection Criteria Exposing radiographs in asymptomatic children
Selection Criteria Exposing radiographs in asymptomatic children
Selection Criteria Development of the dentition as criterion
Selection Criteria Risk of caries as criterion
Selection Criteria Risk of caries as criterion
Selection Criteria Guidelines for prescribing dental radiographs New Patient Child with primary dentition (prior to the eruption of first permanent tooth) -Individualized radiographic exam -Selected periapicals / occlusal views or posterior bitewings ** Patients without evidence of disease and with open proximal contacts may not require a radiographic examination at this time ADA, December 2004
Guidelines for prescribing dental radiographs New Patient Child with transitional dentition (After eruption of first permanent tooth) -Individualized radiographic exam consisting of posterior bitewings with panoramic exam or posterior bitewings and selected periapical images. ADA, December 2004
Guidelines for prescribing dental radiographs New Patient Adolescent with permanent dentition / Adult dentate or partially edentulous (prior to the eruption of third molars) Individualized radiographic exam consisting of posterior bitewings with Panoramic exam or posterior bitewings and selected periapicals A full mouth intraoral radiographic exam is preferred when the patient has clinical evidence of generalized dental disease or history of extensive dental treatment ADA, December 2004
Commonly used radiographic techniques in Pediatric Dentistry • Bitewing • Paralleling • Bisecting
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Photons (x-rays) originating at different places on the focal spot result in a zone of unsharpness on the radiograph The larger the focal spot area, the greater the loss of clarity Three methods to improve the quality of the radiograph: 1. Use as small an effective focal spot as practical (1. 0 mm or less) 2. Increase the distance between the focal spot and the object by using a long, open-ended cylinder 3. Minimize the distance between the object and the film
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Image Size Distortion • Image size distortion (magnification) is the increase in size of the image on the radiograph compared with the actual size of the object. • Image size distortion results from the relative distance of the focal spot-to-film and object-to film • Increasing the focal spot-to film distance and decreasing the object-to-film distance minimizes image magnification
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Image Shape Distortion • Image shape distortion is the result of unequal magnification of different parts of the SAME object. • This situation arises when not all the parts of an object are at the same focal spot-to-object distance. 10 cm 8 cm
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Image Shape Distortion • To minimize shape distortion, the practitioner should make an effort to align the tube, object, and film carefully according to the following guidelines: - Position the film PARALLEL to the long axis of the object - Orient the central x-ray perpendicular to the object and film: Image shape distortion occurs if the object and film are parallel BUT the central x-ray is not directed at right angles to each. This is most evident on maxillary molar projections. Copyright permission from Oral Radiology, White-Pharoah
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Paralleling and Bisecting-Angle Techniques • An early method for aligning the x-ray beam and the film with the teeth and jaws was the bisecting-angle-technique. - The film is placed as close to the teeth as possible without deforming it. - However, when the film is in that position , it is not parallel to the long axes of the teeth - Imaginary plane that bisects the angle between the teeth and the film. Copyright permission from Oral Radiology, White-Pharoah
Commonly used radiographic techniques in Pediatric Dentistry Projection Geometry Paralleling and Bisecting-Angle Techniques • The paralleling technique is the preferred method for making intra-oral radiographs. • It derives its name as the result of placing the film parallel to the long axis of the tooth. • This procedure minimizes image distortion and best incorporates the principles of image geometry. • To achieve this parallel orientation, the practitioner often must position the film towards the middle of the oral cavity, away from the teeth (image magnification and loss of definition) • Use of film holders Copyright permission from Oral Radiology, White-Pharoah
Specific Dental Projections in Pediatric Dentistry • periapical • occlusal • panoramic
Occlusal Projections
Occlusal Techniques -Occlusal radiographs are named for the fact that the film is placed upon the occlusal surface for exposure -Usually # 4 size films, also called occlusal films -Standardized projections
Maxillary Occlusal Projections Occlusal Mandibular Occlusal Projections
Maxillary Occlusal Views 2. Standard Occlusal View Bridge of the nose Similar to anterior occlusal view Film long axis: Side to side (cross) 70 degrees
Glabellum Standard Occlusal Views 70° Film
Standard occlusal view
Mandibular Occlusal Views 1. Anterior Occlusal View Film placed on the occlusal surfaces Long axis: antero-posterior direction The film extends ¼ inch labial In pediatric patients # 2 Beam: Just above the chin point 60 degrees
Film Chin point Anterior Occlusal Views 60°
Panoramic Imaging
Panoramic Imaging Principal Advantages: • Broad coverage of the facial bones and teeth • Low patient radiation dose • Ability to use in patients unable to open their mouths • Short time required to make panoramic image : 3 – 4 minutes (including patient positioning)
Panoramic Imaging Basic Principles • Panoramic imaging is most useful clinically for the diagnostic problems requiring broad coverage of the jaws: Trauma Location of third molars Extensive disease Tooth development
Panoramic Imaging Basic Principles Disadvantages • The images do not display the fine anatomic detail available on intra-oral periapical radiographs. • Unequal magnification • Geometric distortion across the image • Overlapping structures cervical spine in the anterior region
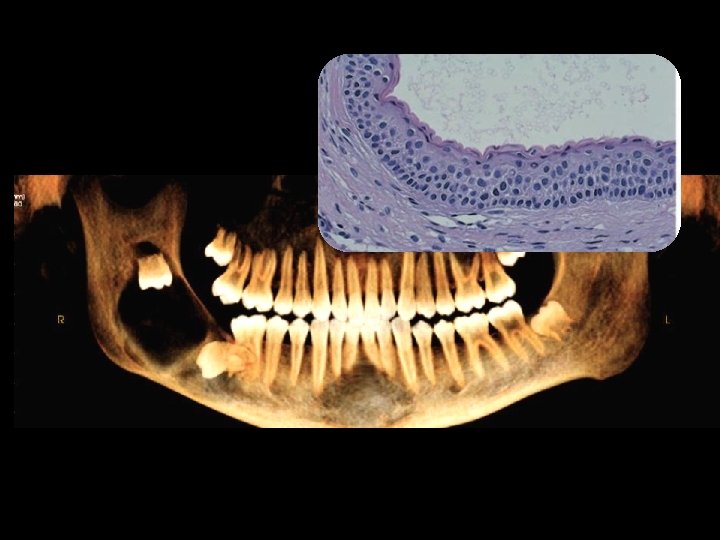
Panoramic Imaging Basic Principles Interpreting the Panoramic Image • Recognizing normal anatomy structures MOST IMPORTANT - Complex of the anatomy of the mid-face - Superimposition of anatomical structures - Changing projection orientation Absence of a normal anatomic structure maybe the MOST IMPORTANT finding on the image.
Panoramic Imaging Anatomic Landmarks
CBCT