Biopsy techniques Department of Oral and Maxillofacial Surgery

Biopsy techniques Department of Oral and Maxillofacial Surgery

CONTENTS • • • INTRODUCTION OBJECTIVES INDICATIONS CONTAINDICATIONS TYPES COMPLICATIONS
 • Bio- meaning")
WHAT IS BIOPSY? • Biopsy is derived from Greek word (By-op-see) • Bio- meaning life and Opsy- to look (vision) • Biopsy is the removal of tissue from a living organism for the purpose of microscopic examination and diagnosis.

OBJECTIVES • To confirm a diagnosis made on clinical finding • To determine the treatment plan • Define a lesion on the basis of its histopathological aspect • As a medical record • Valuable self teaching diagnostic aid
 •")
INDICATIONS • Persistent hyperkeratosis changes in surface tissues (eg: lips or oral mucosa) • Lesion that interfere with local function (eg: fibroma) • Any inflammatory lesion that does not respond to local treatment after 10 to 14 days(i. e. after removing local irritants)

INDICATIONS • Bone lesions not specifically identified by clinical and radiographic findings • Grading of tumor • Any lesion that has the characteristics of malignancy

CONTRAINDICATIONS • • • Angiofibroma Receiving intravenous biphosphonates Uncontrolled bleeding Hemangioma Local infection near the site Multiple neurofibroma

STEPS 1. 2. 3. 4. Selection of area of biopsy Preparation of surgical field Local anesthesia : infiltration or field block Incision : scalpel/punch> electrocautery (23 mm of normal tissue) 5. Handling of specimen 6. Suturing of the resulting wound 7. Making a slide and viewing a slide under microscope
 Excisional or total biopsy 2) Incisional biopsy a) Punch biopsy b) Drill")
TYPES 1) Excisional or total biopsy 2) Incisional biopsy a) Punch biopsy b) Drill biopsy c) Curettage biopsy 3) Needle biopsy i) Aspiration needle biopsy – Fine Needle Aspiration Cytology(FNAC) ii) Core needle biopsy 4) Brush Biopsy

Excisional biopsy An excisional biopsy implies the complete removal of the lesion.
 Should be employed with small lesion less than 1")
EXCISIONAL BIOPSY • Indications: 1) Should be employed with small lesion less than 1 cm. 2) The lesion on clinical exam appears benign. 3) When complete excision with a margin of normal tissue is possible without mutilation. • Technique : The entire lesion with 2 to 3 mm of normal appearing tissue surrounding the lesion is excised

INCISIONAL BIOPSY • If a lesion is large or has different characteristics in various locations more than one area are need to be sampled. • Indications : 1) Size limitations 2) Hazardous locations of the lesion 3) Great suspicion of malignancy • Disadvantages: Crush, splits and hemorrhage are the artifacts most frequently found in incisional biopsy.
 Representative areas are biopsied in a wedge fashion.")
INCISIONAL BIOPSY • Technique : 1) Representative areas are biopsied in a wedge fashion. 2) Margins should extend into normal tissue on the deep surface. 3) Necrotic tissue should be avoided. 4) A narrow deep specimen is better than a broad shallow one.

PUNCH BIOPSY • Useful with mucosal lesion that have different areas such as white, erythematous , ulcerated areas.
 Easy of technique 2) Sutures may not be required")
PUNCH BIOPSY • Advantages: 1) Easy of technique 2) Sutures may not be required if small diameter punch. 3) May produce a more satisfactory specimen in bound down tissues. (eg: hard palate ) • Disadvantages: 1) May not be adequate for biopsy of deeper pathology. 2) May be difficult to biopsy freely movable tissues. (eg: soft palate, floor of mouth)

DRILL BIOPSY CURETTAGE BIOPSY • Particularly useful for • Intraosseous lesions obtaining biopsy material from central • Friable cellular lesions fibro-osseous lesions when only small amount of in the jaw. surface materials is necessary for evaluation. • Osteolytic bony lesions that exceed 1 cm in diameter are aspired prior

ASPIRATION BIOPSY • This is the use of needle and syringe to penetrate a lesion for aspiration of its contents.
 To determine the presence of fluid within a lesions 2) To a")
Indications: 1) To determine the presence of fluid within a lesions 2) To a certain the type of fluid within a intaosseous lesion as cyst. 3) To rule out vascular lesion that can cause life threatening hemorrhage 4) To diagnose multiple tumor or enlarged lymphnodes 5) To confirm suspected malignancy 6) In cases where biopsy is contraindicated on

Technique:

CORE NEEDLE BIOPSY • Also a trucut needle biopsy • Using an 8 to 14 gauge needle • Provides a larger tissue sample than FNAC and lower false negatives rates • Fast and easy to perform and allows histological diagnosis BUT: • It has risks of seeding some types of neoplasm into the tissues and damaging adjacent anatomical structures.

Technique:

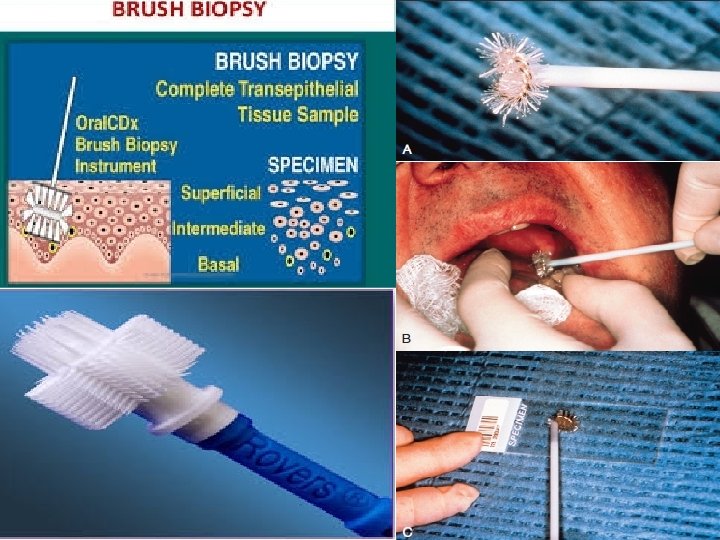
BRUSH BIOPSY • Diagnosis of oral epithelial dysplasia has traditionally been based upon histopathological evaluation of a full thickness biopsy specimen from lesional tissue. • It has recently been proposed that cytological examination of “brush biopsy” samples is a noninvasive method of determining the presence of cellular atypia, and hence the likelihood of oral epithelial dysplasia.

COMMON ERRORS Inadequate tissue specimen Lost specimen Mislabeling of specimen Failure to fix specimen properly Errors occurring during fixation and transit Crushing, cauterizing or other disfigurement of specimen • Failure to note orientation of specimen • Failure to obtain a margin of adjacent normal tissue then desirable • • •

COMPLICATIONS • Hemorrhage • Infection • Poor wound healing • Paresthesia • Injury to adjacent organs/structures

REFERENCES • Neelima Anil Malik-Textbook of Oral and Maxillofacial Surgery, 4 th edition • Contemporary Oral and Maxillofacial Suurgery, 6 th edition • Shafer's Textbook of Oral Pathology, 7 th edition • SRBs manual of surgery, 4 th edition

THANK YOU
- Slides: 27