LA PRISE EN CHARGE THERAPEUTIQUE DE LHTA EN


 Hommes Femmes")











































 MDRD (132 mm.")
















- Slides: 87
LA PRISE EN CHARGE THERAPEUTIQUE DE L’HTA EN 2017 Docteur Lagren Afef Service de cardiologie - CHU Sahloul
L’HTA en 2017 l’HTA reste une cause importante de mortalité et un problème important de santé publique Selon l’OMS, 30% de la population européenne ont des chiffres anormaux de PA Il y aurait aux USA, ~65 millions d’hypertendus En Tunisie, environ 34 % de la population tunisienne est hypertendue… L’hypertension s’accompagne d’un risque majeur de complications : cérébrales, coronaires et rénales
Prévalence de l’hypertension artérielle selon les régions en Tunisie en 2005 (%) Hommes Femmes Total Dist Tunis 33. 8 35. 0 34. 4 NE 24. 3 27. 6 25. 9 NO 20. 9 29. 3 25. 3 CE 32. 4 32. 1 32. 2 ► Hypertension artérielle : Près de 34% des CO 25. 2 28. 7 27. 0 Tunisiens âgés de plus de 35 ans sont 27. 6 38. 3 33. 0 hypertendus ! SO 25. 9 30. 9 28. 5 SE Source INSP 2005
L’HTA est la 1ère cause de mortalité dans le monde Hypertension Tabac Hypercholesterolemie Faible poids corporel Rapport sexuel non protégé IMC élevé Inactivité Physique Alcoolisme Inhalation d’émanations d’hydrocarbures Carence en fer 0 Régions en développement à forte mortalité Régions en développement à plus faible mortalité Régions industrialisées 1000 2000 3000 4000 5000 6000 7000 8000 Mortalité attribuable (En milliers; total 55 861 000) Ezzati et al. , Lancet 2002
La pression artérielle et le risque de mortalité par coronaropathie
La pression artérielle et le risque de mortalité par AVC
Mais l’hypertension artérielle est potentiellement responsable de plusieurs autres complications
Le spectre des complications cardio-vasculaires de l’hypertension artérielle AOMI Anévrysme Aortique Insuffisance cardiaque HVG Infarctus du Myocarde HYPERTENSION Encephalopathie Hypertensive Cardiopathie ischémique Dissection de l’aorte Insuffisance rénale chronique AVC Preéclampsie Hémorragie cérébrale Dustan HP et al. Arch Intern Med. 1996; 156: 1926 -1935
Evaluation initiale de nos patients hypertendus
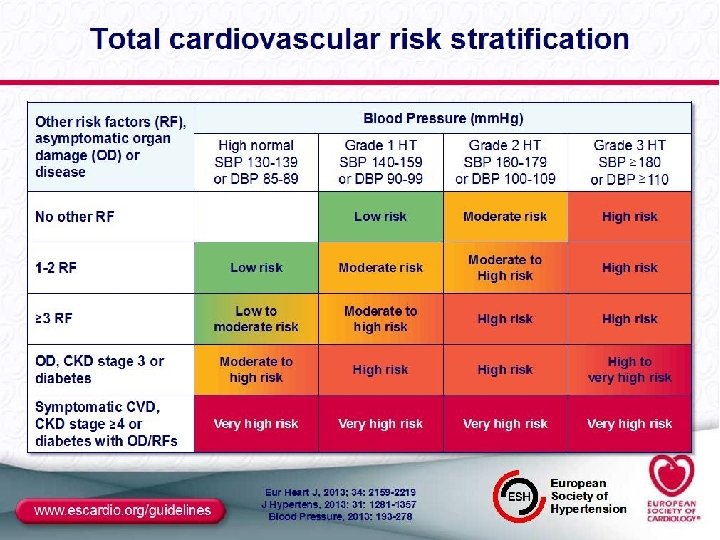
Les chiffres tensionnels n’ont en soi qu’une valeur toute relative. Ils sont l’une des données de l’évaluation du risque CV globale qui seule détermine les décisions thérapeutiques. JNC VII
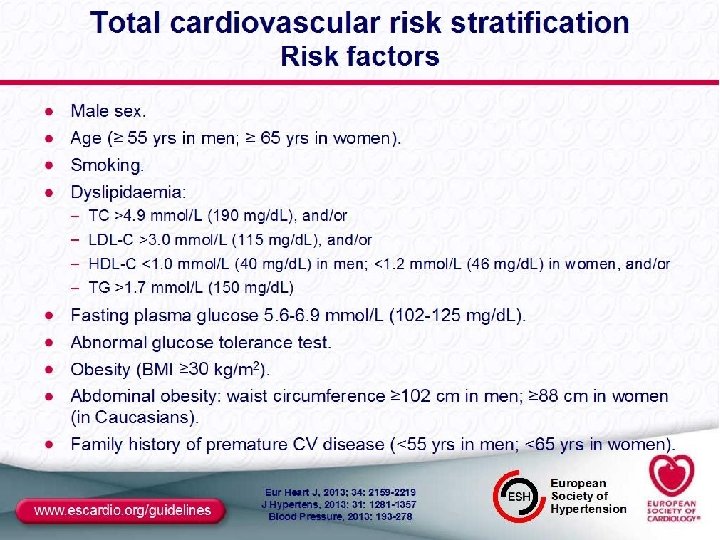
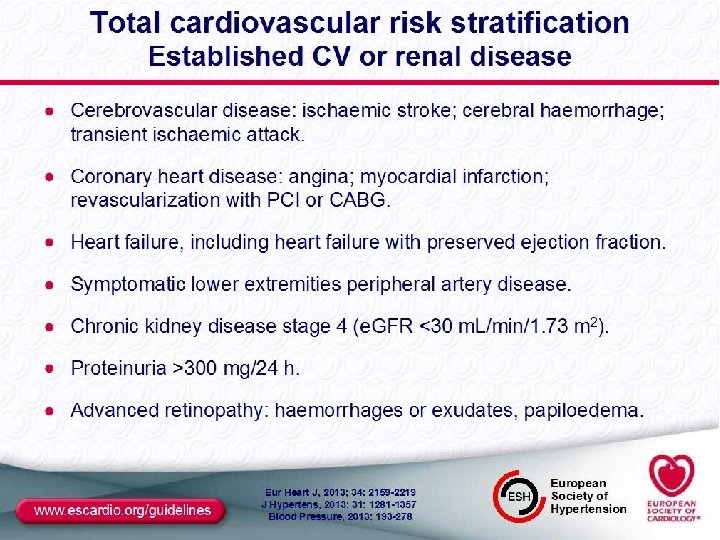
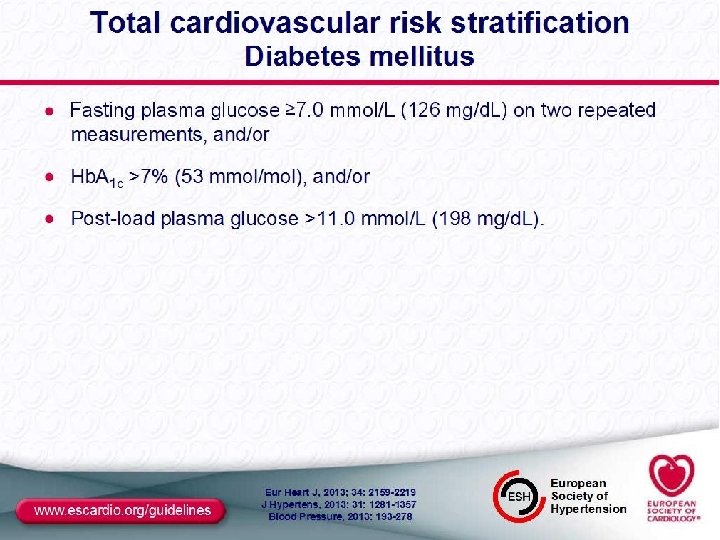
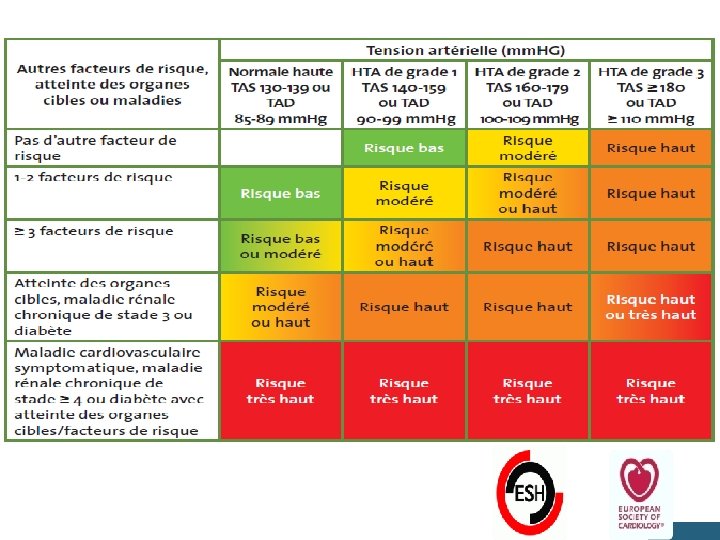
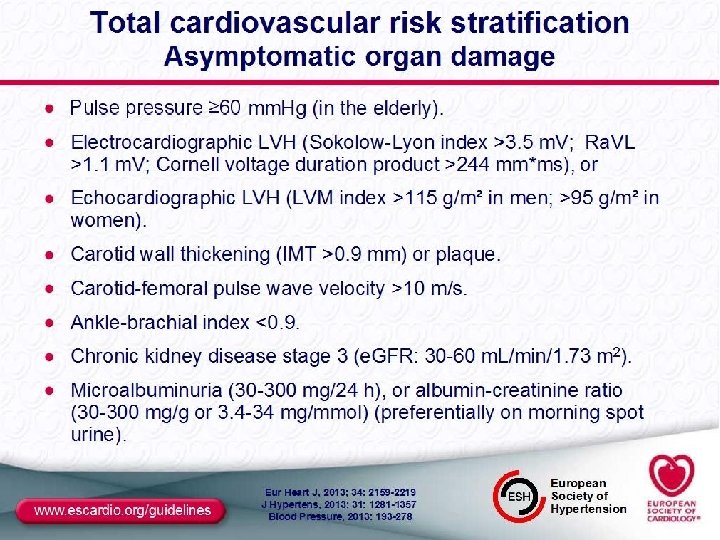
Évaluation initiale de nos hypertendus IL FAUT IDENTIFIER : ► les facteurs de risque ► une atteinte des organes cibles ► un Diabète ► et/ou une maladie cardio-vasculaire et rénale associée afin d’estimer le niveau de RCV du patient et ne pas méconnaître une HTA secondaire
Atteinte des organes cibles Cœur HVG Angine de poitrine ou IDM Insuffisance cardiaque Cerveau AIT ou AVC Rein IR chronique Vaisseaux Artériopathie des MI Œil Rétinopathie hypertensive
Les patients hypertendus Tunisiens suivis sont souvent à haut risque cardiovasculaire L’hypertension artérielle prise en charge en médecine générale. A propos d’une cohorte tunisienne de 2662 cas F Jarraya et al. Archives des Maladies du cœur et des vaisseaux 2007
1976 -1980 1988 -1991 -1994 2008 Pts se sachant hypertendu 51% 73 % 68 % 50 Pts traités 31% 55 % 54 % 78 % d’HTA contrôlées 10% 29 % 27 % 33
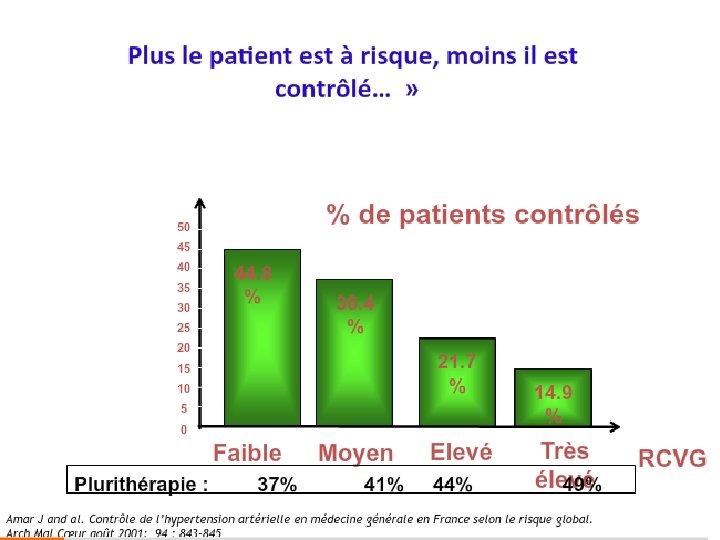
Le plus grand paradoxe de l’HTA: plus le patient est à risque, moins il est contrôlé % de contrôlés Etude sur 15 514 patients hypertendus traités 44. 8% 36. 4% 21. 7% 14. 9% faible moyen élevé Risque très élevé CV Amar J and al. Contrôle de l’hypertension artérielle en médecine générale en France selon le risque global. Arch Mal Cœur août 2001; 94 : 843 -845
les objectifs du traitement
Objectifs du Traitement de l’HTA Réduire les risques de morbidité et de mortalité CV ♥ La prise en charge des facteurs de risque réversibles: le tabagisme, la dyslipidémie , le diabète sucré… ♥ La prise en charge des pathologies associées: insuffisance cardiaque, coronaropathie, atteintes vasculaires … ♥ Atteindre les objectifs tensionnels. ♥ Dépister et traiter les complications de HTA.
Increases in Antihypertensive Prescriptions and Reductions in Cardiovascular Events in Canada Norm R. C. Campbell, Rollin Brant, Helen Johansen, Robin L. Walker, Andreas Wielgosz, Jay Onysko, Ru-Nie Gao, Christie Sambell, Stephen Phillips, Finlay A. Mc. Alister; for the Canadian Hypertension. Education Program Outcomes Research Task Force Hypertension. 2009; 53: 128 -134
Les Objectifs en 2013 - 2014
Comment traiter ?
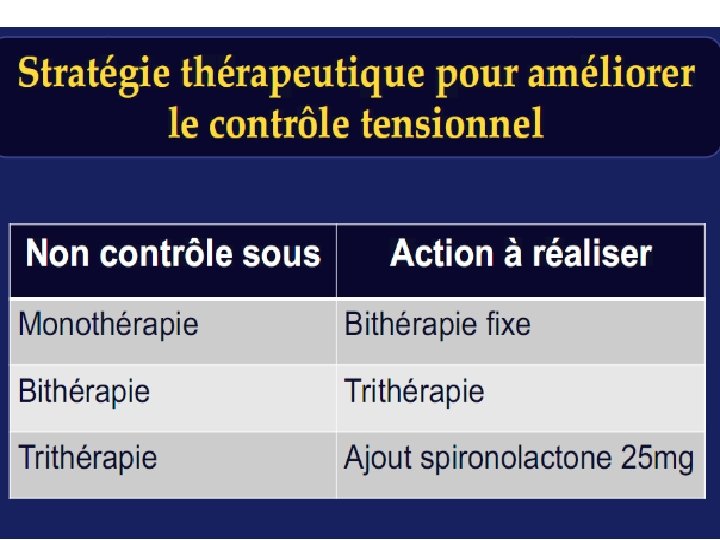
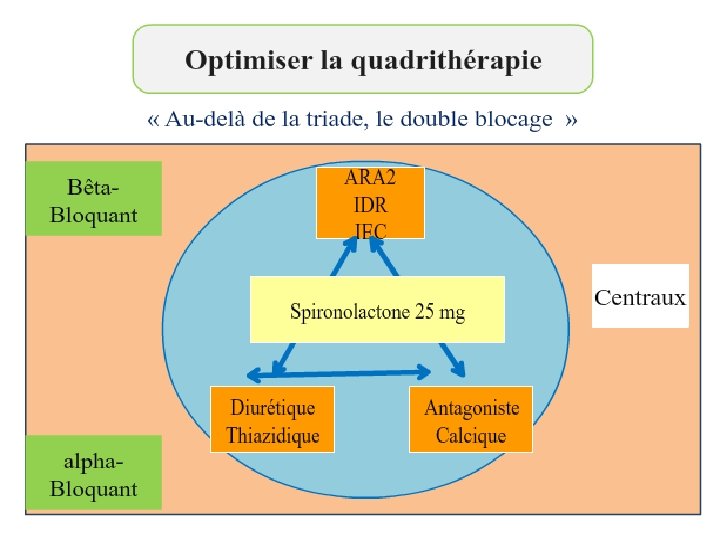
Stratégie thérapeutique
Recommandations relatives aux habitudes de vie pour la prévention et le traitement de l’HTA Réduction du risque d’HTA Diminution de l’apport en sodium à moins de 1500 mg/jour Alimentation saine : riche en fruits et en légumes frais, en produits laitiers à faible teneur en matières grasses, en fibres alimentaires solubles, en céréales de grains entiers et en protéines de source végétale, et pauvre en graisses saturées, en cholestérol et en sodium, conformément aux recommandations du Guide alimentaire canadien pour manger sainement Activité physique régulière : total de 30 à 60 minutes d’activité d’aérobie d’intensité modérée (p. ex. marche rapide), 4 à 7 fois par semaine, en plus des activités quotidiennes Consommation modérée d’alcool : pas plus de 2 consommations standard par jour et moins de 14 par semaine pour les hommes et moins de 9 par semaine pour les femmes Maintien d’un poids santé : indice de masse corporelle entre 18, 5 et 24, 9 kg/m 2 Tour de taille Hommes Femmes - Type europoïde, africain subsaharien, moyen-oriental <94 cm < 80 cm - Type asiatique méridional; Chinois < 90 cm < 80 cm Environnement sans fumée 29 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Recommandations concernant l’apport quotidien en sodium ge Apport recommandé 19 -50 1500 51 -70 1300 71 et plus 1200 • 2300 mg de sodium (Na) – = 100 mmol de sodium (Na) – = 5, 8 g de sel (Na. Cl) – = 1 cuillérée à thé de sel de table • 80 % de l’apport quotidien moyen en sodium provient des aliments transformés • Seulement 10 % provient de l’ajout de sel à la cuisson ou à la consommation. 30 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Mesure du tour de taille Tissu adipeux sous-cutané Extrémité de la dernière côte Couche musculaire Distance moyenne Tissu adipeux intraabdominal Crête iliaque 31 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Recommandations relatives aux habitudes de vie – Gestion du stress Patients hypertendus chez qui le stress semble constituer un problème important. Modification du comportement Les interventions cognitivo-comportementales individualisées ont plus de chances d’être efficaces lorsqu’elles sont associées à des techniques de relaxation. 32 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Modification des habitudes de vie chez les adultes hypertendus – Résumé Intervention Cible Consommation réduite d’aliments contenant du sodium ajouté < 2 300 mg /jour Perte de poids IMC < 25 kg/m 2 Alcool < 2 consommations/jour Activité physique 30 à 60 minutes, 4 à 7 jours/semaine Régime alimentaire Régime DASH Abandon du tabagisme Environnement sans fumée Tour de taille - Type europoïde - Type asiatique méridional; Chinois 33 Hommes Femmes <94 cm <80 cm <90 cm <80 cm Programme éducatif canadien sur l’hypertension – Recommandations 2011
Effet des modifications des habitudes de vie sur la PA chez les adultes hypertendus Intervention Consommation réduite d’aliments contenant du sodium ajouté Intervention - 1 800 mg de PAS/PAD sodium/jour Pers. hypertendues -5, 1/-2, 7 par kg perdu -1, 1/-0, 9 -3, 6 consommations/ jour -3, 9/-2, 4 Activités d’aérobie 120 à 150 min/ semaine -4, 9/-3, 7 Régime alimentaire Régime DASH Pers. hypertendues -11, 4/-5, 5 Perte de poids Alcool Padwal R. et al. CMAJ ・ SEPT. 27, 2005; 173 (7) 749 -751 34 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Les règles hygiéno-diététiques devraient cibler en priorité les pré-hypertendus Hypertension. 2006; 47: 162 -167
Chez un malade hypertendu, il est inéluctable d’utiliser des médicaments reduisants le risque évolutif …
Development of JNC-8 • 3 critical questions for adults with hypertension – Does initiating antihypertensive pharmacologic therapy at specific blood pressure thresholds improve health outcomes? [When to start therapy? ] – Does treatment with antihypertensive pharmacologic therapy to a specified blood pressure goal lead to improvements in health outcomes? [How low should I go? ] – Do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes? [What drug do I use? ] James PA et al. JAMA 2014; 311: 507 -20.
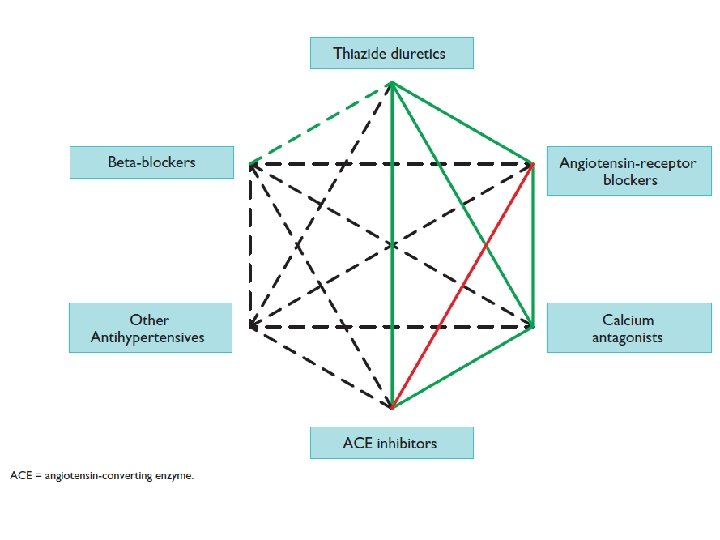
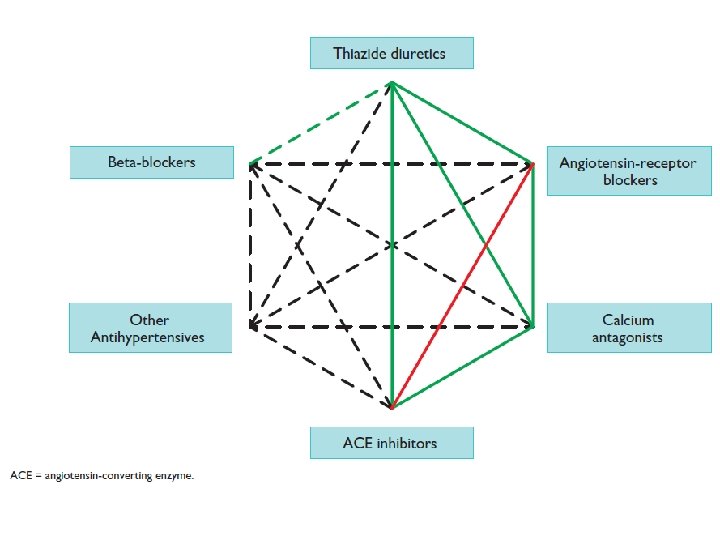
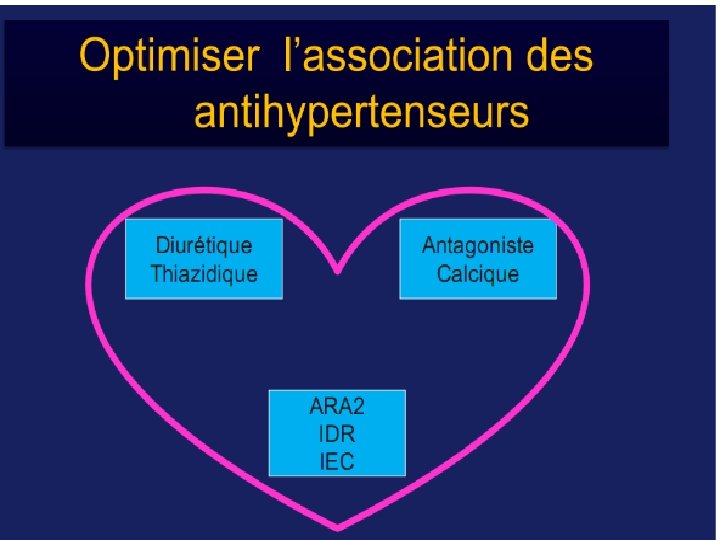
Combinaisons recommandeées divers antihypertenseurs Diuretiques ARA 2 -bloqueurs Inhibit. calciques IEC Preferred combinations Other possible combinations J Hypertens. 2007; 25: 1105– 1187. J Hypertens. 2009; 27: 2121 -2158.
Pour quelle association opter ? Guidelines ESH/ESC 2007 Guidelines ESH 2009 Neil R Poulter, Journal of Hypertension 2011, 29 (suppl 1): S 15–S 21
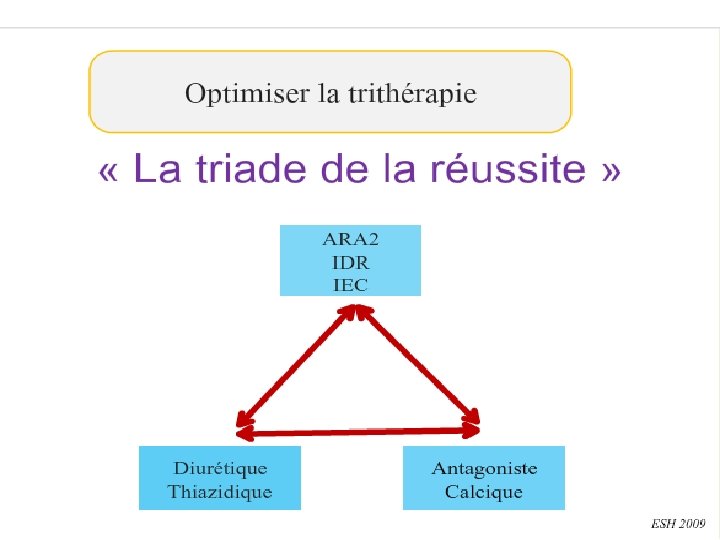
ESC 2013
2013 ESH/ESC Guidelines for the management of arterial hypertension Monotherapy vs. drug combination strategies to achieve target BP Choose between Mild BP elevation Low/moderate CV risk Single agent Marked BP elevation High/very high CV risk Two–drug combination Switch to different agent Previous agent at full dose Full dose monotherapy Two drug combination at full doses Previous combination at full dose Add a third drug Switch to different two–drug combination Three drug combination at full doses Moving from a less intensive to a more intensive therapeutic strategy should be done whenever BP target is not achieved. BP, blood pressure; CV, cardiovascular. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
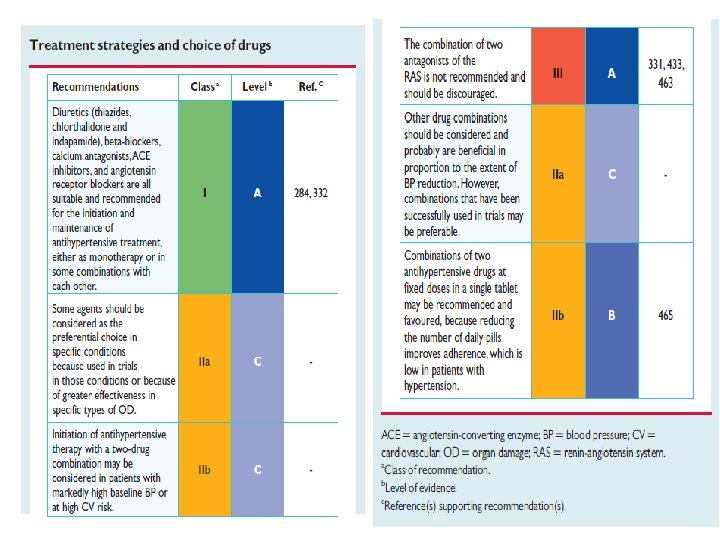
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment options Clinical scenario Recommendations Initiation and maintenance treatment Monotheray or in combination • Diuretics (thiazides, chlorthalidone, indapamide) • BBs • CCBs • ACE-I • ARBs Consider some agents as preferential choice in specific conditions due to: • Use in trials in those conditions • Great effectiveness in specific types of OD Consider two-drug combination therapy in patient with: • High baseline BP • High CV risk Combination of two RAS antagonists Not recommended Consider other drug combinations for BP reduction Most preferable option may be combinations successfully used in trial Combination therapy with fixed doses of two drugs in a single tablet May be recommended due to potential for improved adherence BB, beta-blocker; CCB, calcium channel blockers; ACE-I, angiotensin-converting-enzyme inhibitor; ARB, angiotensin receptor blocker; OD, organ damage; BP, blood pressure; CV, cardiovascular; RAS, renin–angiotensin system. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
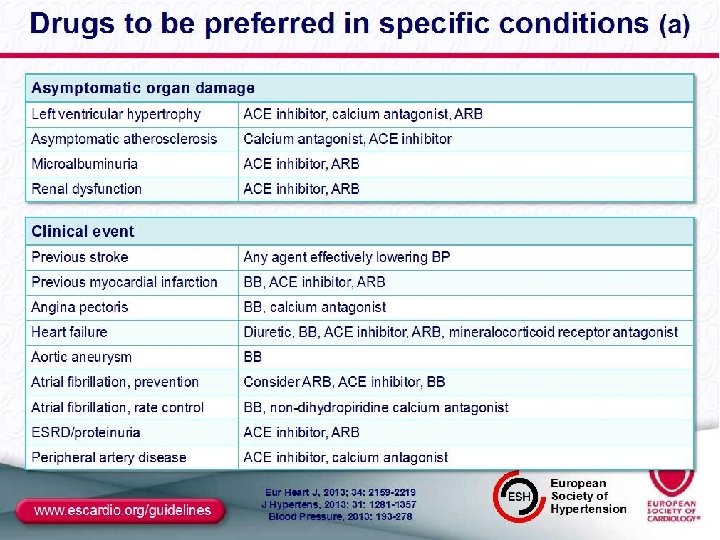
JNC-7 Compelling Indications Chobanian AV et al. JAMA 2003; 289: 2560 -72.
1
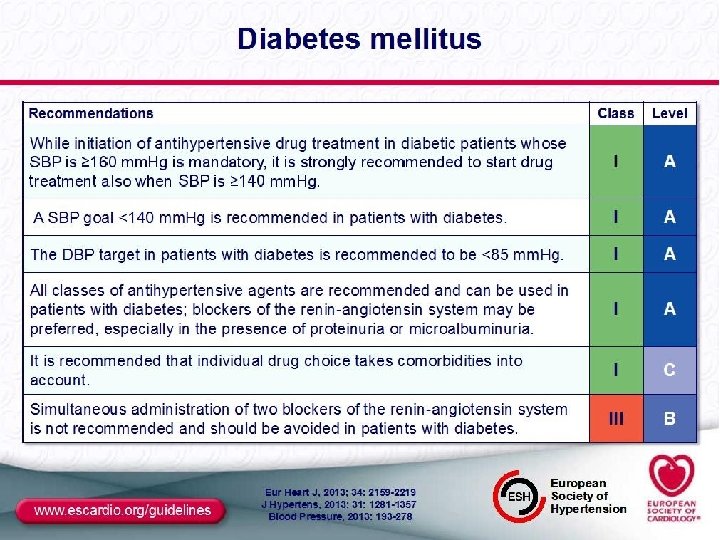
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment for people with diabetes Recommendations Additonal considerations Mandatory: initiate drug treatment in patients with SBP ≥ 160 mm. Hg • Strongly recommended: start drug treatment when SBP ≥ 140 mm. Hg SBP goals for patients with diabetes: <140 mm. Hg DBP goals for patients with diabetes: <85 mm. Hg All hypertension treatment agents are recommended and may be used in patients with diabetes • RAS blockers may be preferred • Especially in presence of preoteinuria or microalbuminuria Choice of hypertension treatment must take comorbidities into account • Avoid in patients with diabetes Coadministration of RAS blockers not recommended SBP, systolic blood pressure; DBP, diastolic blood pressure; RAS, renin–angiotensin system. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
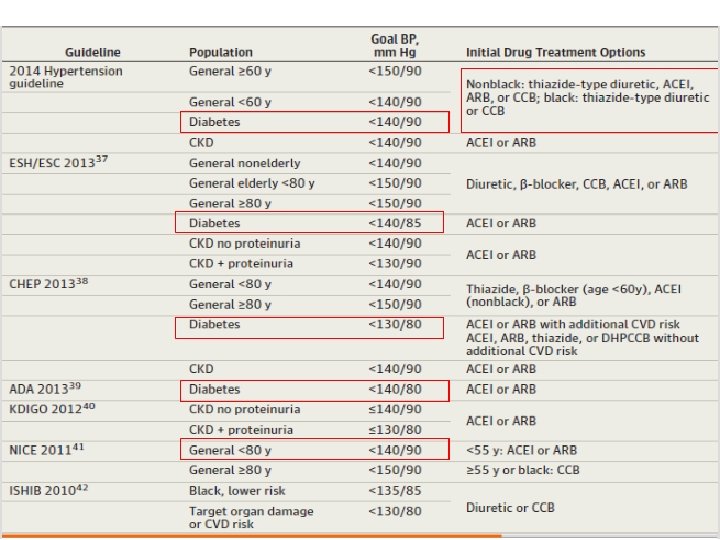
Comparisons to Other Guidelines BP Goal JNC-7 JNC-8 ASH/ISH ESC/ESH CHEP Age < 60 <140/90 <140/90 Age 60 -79 <140/90 <150/90 <140/90 Age 80+ <140/90 <150/90 Diabetes <130/80 <140/90 <140/85 <130/80 CKD <130/80 <140/90 <130/90 <140/90 Adapted from Salvo M et al. Ann Pharmacother 2014; 48: 1242 -8.
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment for people with nephropathy Recommendations Additonal considerations Consider lowering SBP to <140 mm. Hg Consider SBP <130 mm. Hg with overt proteinuria • Monitor changes in e. GFR RAS blockers more effective to reduce albuminuria than other agents • Indicated in presence of microalbuminuria or overt proteinuria Combination therapy usually required to reach BP goals • Combine RAS blockers with other agents Combination of two RAS blockers • Not recommended Aldosterone antagonist not recommended in CKD • Especially in combination with a RAS blocker • Risk of excessive reduction in renal function, hyperkalemia SBP, systolic blood pressure; CKD, chronic kidney disease; e. GFR, estimated glomerular filtration rate; RAS, renin–angiotensin system. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment for people with metabolic syndrome Recommendations Additonal considerations Lifestyle changes for all • Especially weight loss and physical activity • Improve BP and components of metabolic syndrome, delay diabetes onset Antihypertensive agents that potentially improve – or not worsen – insulin sensitivity are recommended • RAS blockers • CCBs BBs and diuretics only as additional drugs • Preferably in combination with a potassiumsparing agent Prescribe antihypertensive drugs with particular care in patients with metabolic disturbances when… • BP ≥ 140/90 mm. Hg after lifestyle changes to mantain BP <140/90 mm. Hg No drug treatment in patients with metabolic syndrome and high normal BP BP, blood pressure; BB, beta blockers; CCB, calcium channel blockers; RAS, renin–angiotensin system. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment in the elderly Clinical scenario Recommendations Elderly patients with SBP ≥ 160 mm. Hg • Reduce SBP to 140 -150 mm. Hg Fit elderly patients aged <80 years with initial SBP ≥ 140 mm. Hg • Consider antihypertensive treatment • Target SBP: <140 mm. Hg Elderly >80 years with initial SBP ≥ 160 mm. Hg • Reduce SBP to 140 -150 mm. Hg providing in good physical and mental condition Frail elderly • Hypertension treatment decision at discretion of treating clinician, based on monitoring of treatment clinical effects Continuation of well- tolerated hypertension treatment • Consider when patients become octogenarians All hypertension treatment agents are recommended and may be used in elderly • Diuretics, CCBs, preferred for isolated systolic hypertension SBP, systolic blood pressure; CCB, calcium channel blockers. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
HYVET • HYpertension in the Very Elderly Trial – Randomized, double-blind trial – Included patients aged 80 or older with SBP>160 mm. Hg – Randomized to indapamide +/- perindopril or placebo – Target BP of 150/80 mm. Hg – Primary outcome of fatal or nonfatal stroke Beckett NS et al. N Engl J Med 2008; 358: 1887 -98.
HYVET • Results – Mean BP at the end of the trial • Indapamide +/- perindopril - 143/78 mm Hg • Placebo – 158/84 mm Hg – 48. 0% of indapamide patients achieved goal BP vs. 19. 9% of placebo patients (p<0. 001) – Outcomes with indapamide +/- perindopril • 30% reduction in stroke (p=0. 06) • 64% reduction in heart failure (p<0. 001) • 21% reduction in all-cause mortality (p=0. 02) Beckett NS et al. N Engl J Med 2008; 358: 1887 -98.
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment for people with heart disease Recommendations Additonal considerations SBP goals for hypertensive patients with CHD: <140 mm. Hg BBs for hypertensive patients with recent MI • Other CHD: other antihypertensive agents can be used; BBs, CCBs preferred Diuretics, BBs, ACE-I, ARBs, and/or mineralcorticoid receptor antagonist for patients with heart failure or severe LV dysfunction • Reduce mortality and hospitalization No evidence that any hypertension drug beneficial for patients with heart failure and preserved EF • However, in these patients and patients with hypertension and systolic dysfunction: consider lowering SBP to ∼ 140 mm. Hg • Guide treatment by symptom relief Consider ACE-I and ARBs (and BBs and mineralcorticoid receptor antagonist in coexisting heart failure) in patients at risk of new or recurrent AF Antihypertensive therapy in all patients with LVH • Initiate treatment with an agent with greater ability to regress LVH (ACE-I, ARBs, CCBs) SBP, systolic blood pressure; BB, beta-blocker; MI, myocardial infarction; ACE-I, angiotensin-converting-enzyme inhibitor; ARB, angiotensin receptor blocker; LV, left ventricular; EF, ejection fraction; CHD, coronary heart disease; CCB, calcium channel blockers; AF, atrial fibrillation; LVH, left ventricular hypertrophy. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
2013 ESH/ESC Guidelines for the management of arterial hypertension Hypertension treatment for women Clinical scenario Recommendations Hormone therapy and selective estrogen receptor modulators • Not recommended; should be used for primary or secondary CVD prevention If treatment of younger perimenopausal women is considered for severe menopausal symptoms • Weigh risk/benefit profile Drug treatment of severe hypertension in pregnangy (SBP >160 mm. Hg or DBP >110 mm. Hg) • Recommended Pregnant women with persistent BP elevations ≥ 150/95 mm. Hg • Consider drug treatment BP ≥ 140/90 mm. Hg in presence of gestational hypertension, subclinical OD, or symptoms High risk of pre-eclampsia • Consider treating with low-dose aspirin from 12 weeks until delivery • Providing low risk of GI hemorrhage Women with child-bearing potential • RAS blockers not recommended Methyldopa, labetolol, nifedipine • Consider as preferential drugs in pregnancy • For pre-eclampsia: intravenous labetolol or infusion of nitroprusside SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood presure; OD, organ damage; CVD, cardiovascular disease; GI, gastrointestinal; RAS, renin–angiotensin system. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) - J Hypertension 2013; 31: 1281 -1357 Medical Education & Information – for all Media, all Disciplines, from all over the World Powered by
Plusieurs Antihypertenseurs sont nécessaires pour atteindre l’objectif tensionnel Essai (PAS atteint) MDRD (132 mm. Hg) HOT (138 mm. Hg) RENAAL (141 mm. Hg) AASK (128 mm. Hg) ABCD (132 mm. Hg) IDNT (138 mm. Hg) UKPDS (144 mm. Hg) ASCOT-BPLA (136. 9 mm. Hg) ALLHAT (138 mm. Hg) ACCOMPLISH* (132 mm. Hg) 1 Initial 2 -drug combination therapy *Interim 6 -month data 2 3 no moyen des antihypertenseurs 4 Bakris et al. Am J Med 2004; 116(5 A): 30 S– 8
50 à 75 % des patients hypertendus vont nécessiter une association d’antihypertenseurs pour atteindre la cible thérapeutique Les associations d’antihypertenseurs: une nécessité dans la pratique clinique
AVANTAGES DES ASSOCIATIONS FIXES …
Une révolution au quotidien pour les hypertendus
Avantages de l’association fixe Versus l’association libre de deux antihypertenseurs Fixe Libre Simplicité du traitement + – Compliance + – Efficacité + + Tolérance +* – Coût + – Flexibilité – + *De faibles doses sont généralement utilisés dans les associations fixes + =avantage potentiel
Intérêt de l’association fixe Perindopril / Amlodipine Bangalore S, Messerli FH. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007; 120: 713 -719.
QUELLE ASSOCIATION POUR INITIER LE TTT ? Les antihypertenseurs sont –ils égaux en efficacité et en prévention des événements CV ?
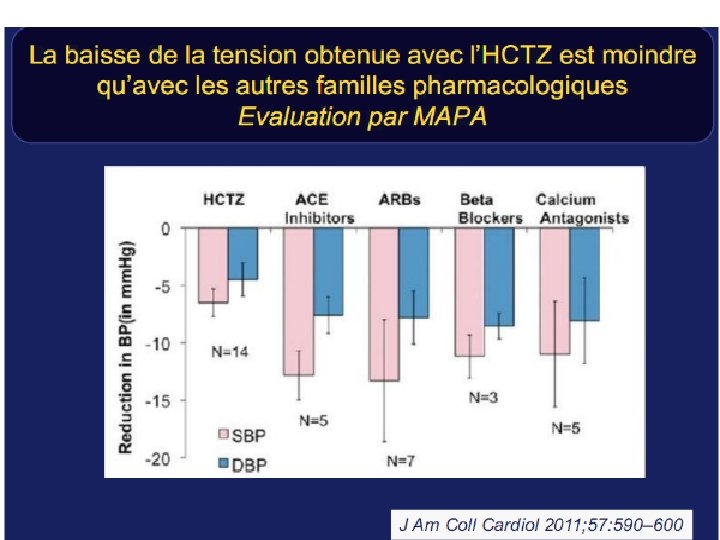
Méta-analyse de 47 essais randomisés dans la prévention des maladies cardiovasculaires Bénéfices comparés des traitements Les Bêtabloquants sont moins efficaces que les antagonistes calciques pour la prévention des AVC. Toutes les familles sont équivalentes pour la prévention de la maladie coronaire. BMJ 2009; 338; b 1665;
Tous les antihypertenseurs sont-ils équivalents ? Physicians Desk Reference. NJ: Medical Economics Company; 2008.
Une efficacité tensionnelle garantie sur 24 h Tous les antihypertenseurs ne sont pas équivalents Rapport vallée/pic 8 AM 12 AM 16 PM 20 PM 24 PM 4 AM 8 AM Antihypertenseurs avec T/P < 60 % Antihypertenseurs avec T/P = 60 -90 % Antihypertenseurs avec T/P = 75 -100 % mm Hg Baisse tensionnelle 24 h après administration Captopril Enalapril Ramipril Irbesartan Olmesartan Losartan Aliskiren Telmisartan Lercanidipine Périndopril Amlodipine
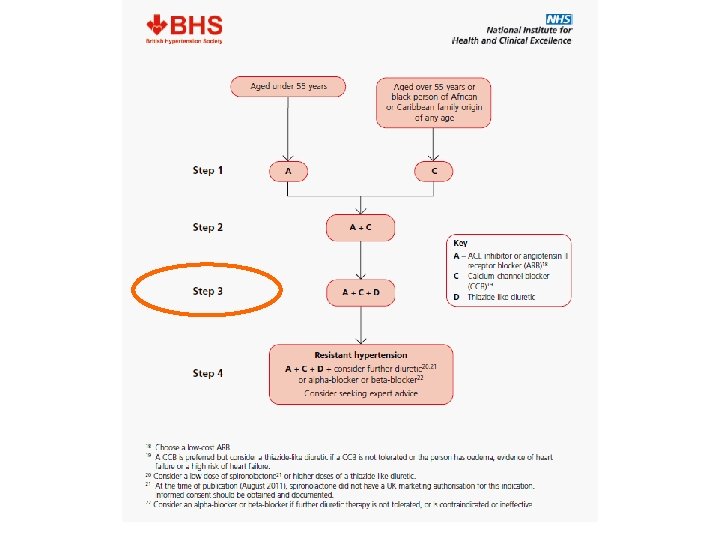
Place de la bithérapie en association fixe - En première intention si HTA grade II ou si PAS > 20 et PAD > 10 mm Hg par rapport à cible thérapeutique: (ESC ASH SFH NICE) - En deuxième intention après un mois si échec monothérapie: (SFH) - En cas de résistance à une bithérapie il est légitime d’essayer une autre association fixe (SFH )
Place de la bithérapie en association fixe single pill combination Association initiale recommandée: - IEC/ARA 2 plus IC : ( NICE) - IEC/ARA 2 plus IC ou diurétique: (ESC/ESH, SFH, ASH) - Béta bloqueurs plus diurétiques à éviter : (ESC, ASH, NICE, SFH, )
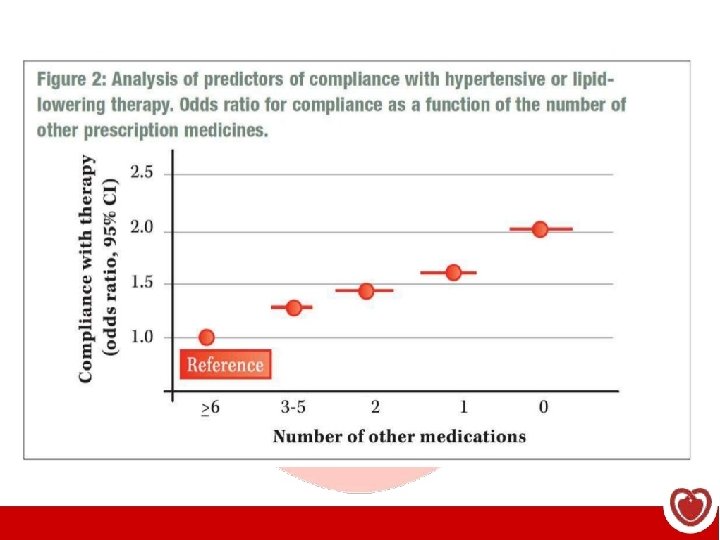
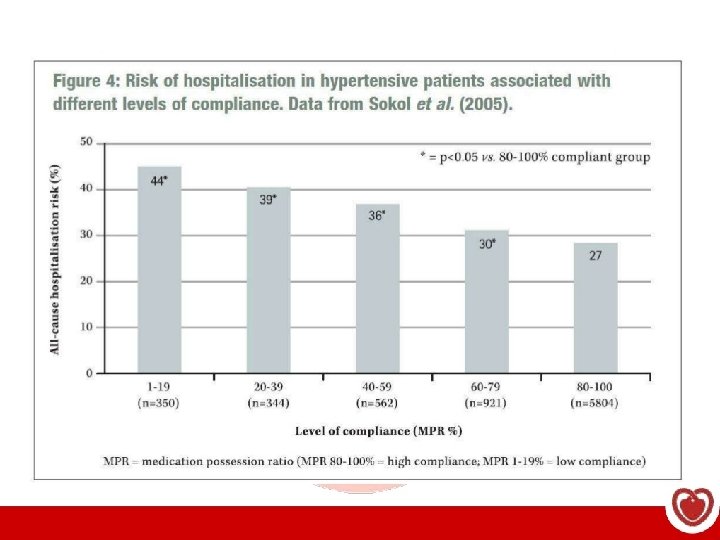
Les médicaments ne sont pas efficaces chez les patients qui ne les prennent pas
Recommandations relatives aux habitudes de vie – Perte de poids Mesurer la taille, le poids et le tour de taille et calculer l’indice de masse corporelle (IMC) chez tous les adultes. Tous les patients, notamment les hypertendus IMC supérieur à 25 - Perte de poids - IMC santé : 18, 5 à 24, 9 kg/m 2 Tour de taille Hommes Femmes - Type europoïde, africain subsaharien, moyen-oriental < 94 cm < 80 cm - Type asiatique méridional; Chinois, Japonais < 90 cm < 80 cm Associée à la pharmacothérapie, la perte de poids accentue l’effet antihypertenseur. Les stratégies de perte de poids devraient reposer sur une approche pluridisciplinaire et prévoir des conseils nutritionnels, une augmentation de l’activité physique et des modifications du comportement. CMAJ 2007; 176: 1103 -6 88 Programme éducatif canadien sur l’hypertension – Recommandations 2011
Traitement de l’HTA systolo-diastolique sans autre indication formelle chez l’adulte CIBLE : < 140/90 mm Hg TRAITEMENT INITIAL ET MONOTHÉRAPIE Modification des habitudes de vie Thiazide IECA ARA ICC à action prolongée Bêtabloquant (BB)* L’association de deux médicaments de première intention peut être envisagée comme traitement initial si la PA systolique excède de 20 mm Hg ou plus la valeur cible ou si la PA diastolique excède de 10 mm Hg ou plus la valeur cible. *Les BB ne sont pas indiqués en première intention chez les adultes de 60 ans et plus. Les IECA, les ARA et les inhibiteurs directs de la rénine sont contre-indiqués en cas de grossesse et il faut faire preuve de prudence chez les femmes en âge de procréer. 89 Programme éducatif canadien sur l’hypertension – Recommandations 2011
sont plus nombreux à répondre à leur traitement et à atteindre leur Les patients tension artérielle cible. Avantages des associations fixes La tolérance est maintenue ou améliorée, ce qui peut rendre le traitement plus commode et améliorer son observance. Le rapport coût-efficacité peut être plus favorable. Recommandé par les sociétés savantes