Infectious Diseases of the Respiratory System Meral SNMEZOLU





 in Europe. Welte T et al.")





")




 doi:")










 are of little")





 Respiratory rate (>30) Blood Pressure")














 • Influenza virus Fungal Infections • Coccidiodomycosis")
 RNA virus • Spread by respiratory droplets •")




 67")
 68")

 • Influenza A")





 Neuraminidase (NA) M 2 Nucleoprotein (NP) M")




 Fever Childre n Adults Elderl")



 – NP aspirates and swabs only –")

: CONTRAINIDATIONS • Hypersensitivity to eggs or vaccine components • Acute febrile")







")
")
")
")











- Slides: 109
Infectious Diseases of the Respiratory System Meral SÖNMEZOĞLU, MD Yeditepe University Hospital Professor of Department of Infectious Diseases and Microbiology
Infections of the Respiratory tract • Most common entry point for infections • Upper respiratory tract – nose, nasal cavity, sinuses, mouth, throat • Lower respiratory tract – Trachea, bronchioles, and alveoli in the lungs
Upper Respiratory Infections • • • Common Cold Pharyngitis, tonsillitis Acute sinusitis Acute laryngotracheobronchitis (Croup) Otitis media, otitis externa, mastoitidis
Fig. 21. 1 a
Aetiology
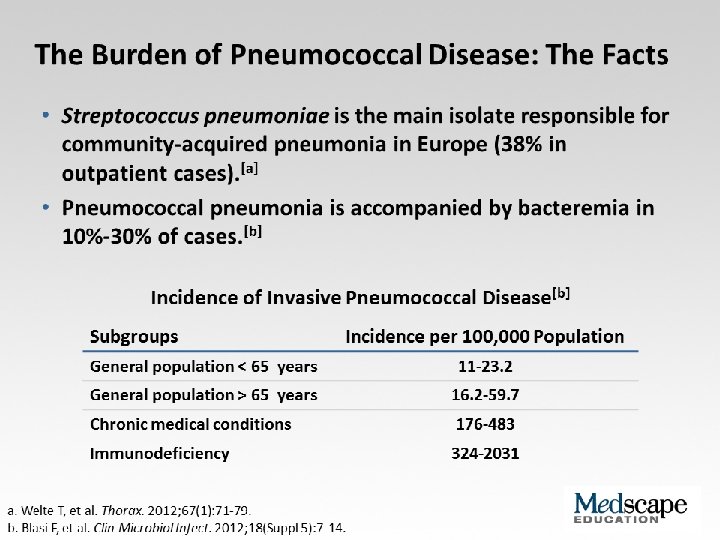
Frequency of causative organisms of community-acquired pneumonia (CAP) in Europe. Welte T et al. Thorax 2012; 67: 71 -79 Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.
Treatment setting
Frequency of Isolation of Causative Organisms of CAP in Europe by Country Percentage Means of Frequency of Isolation in Each Country Franc e Italy Spain Turkey UK German y S pneumoniae 37. 2 11. 9 33. 7 25. 5 42. 1 40 Haemophilus influenzae 10. 3 5. 1 5. 3 44. 9 12. 3 8 Legionella spp. 2. 0 4. 9 12. 9 0 9. 1 3. 1 Staphylococcus spp. 11. 7 6. 5 3. 2 1. 0 2. 6 5 Moraxella catarrhalis 3. 3 1. 0 2. 7 12. 2 0. 8 0 Gram-negative bacilli 16. 8 24. 3 7. 9 4. 1 2. 6 7 Mycoplasma pneumoniae 0. 7 7. 0 8. 4 0 5. 3 5. 6 1 2. 4 7. 2 0 5. 9 1. 3 Coxiella burnetii 0. 2 0. 4 6. 2 0 0. 3 0 Viruses 1. 7 11. 6 5. 9 0 18. 6 9 No pathogen identified 35. 6 67. 3 56. 8 40. 6 38. 4 NR Chlamydophila spp.
Protective Mechanisms Normal flora: Commensal organisms • Limited to the upper tract • Mostly Gram positive or anaeorbic • Microbial antagonist (competition)
Defense Mechanisms • 80% of cells lining central airways are ciliated, pseudostratified, columnar epithelial cells • Each ciliated cell contains about 200 cilia that beat in coordinated waves about 1000 x/minute • So the lower respiratory tract is normally sterile
Protective Mechanisms Clearance of particles and organisms from the respiratory tract Cilia and microvilli move particles up to the throat where they are swallowed. Alveolar macrophages migrate and engulf particles and bacteria in the alveoli deep in the lungs.
Other Protective Mechanisms • • • Nasal hair, nasal turbinates Mucus Involuntary responses (coughing) Secretory Ig. A Immune cells
Fate of Droplets Organisms Liberated Talking 0 -200 Coughing 0 -3500 Sneezing 4500 -1, 000 Droplets can remain suspended in the air for hours.
First cause of death in the United States from infectious disease is: A. Meningitis B. Pneumonia C. Gastroenteritis D. Urinary Tract Infections E. Toe fungus
First cause of death in the United States from infectious disease is: A. Meningitis B. Pneumonia C. Gastroenteritis D. Urinary Tract Infections E. Toe fungus
First cause of death in the United States from infectious disease is: A. Meningitis B. Pneumonia C. Gastroenteritis D. Urinary Tract Infections E. Toe fungus
Mortality due to infections DM Morens et al. Nature 463, 122 -122 (2010) doi: 10. 1038/nature 08554
All cause mortality in Turkey 3, 29 1, 67 1, 22 0, 43 0, 42 0, 2 2, 6 1, 75 0, 07 4, 1 4, 29 4, 76 6 9, 67 21, 58 0, 0200000001 D N o S e l E o a D n lp ş S id u lı 37, 93 Y iğ o n a m G a n e ku zs S e rim i P in a risa E e n ild n il K n rd ta u m sa o fio n ye tr n e rü m u te jka ira m e stm izb i n ia n e o h iyle h la to ris a n rzt lm a
Antimicrob Agents Chemother. 2014 Aug 4.
Pneumonia • Most deadly infectious disease in the U. S. • 6 th leading cause of death • Average mortality 14% • $20 billion/year in U. S. 1 • Community acquired pneumonia affects ~4 million patients and results in 10 million physician visits, • 1 million hospitalizations, and >50, 000 deaths annually File Chest 2004; 125: 1888 -1901
Pneumonia Pathophysiology • Microbial pathogens enter the lung by: • Aspiration of organisms from oropharynx – More common in patients with impaired level of consciousness: alcoholics, IVDA, seizures, stroke, anesthesia, swallowing disorders, NG tubes, ETT – Gram positive and anaerobes: Strep pneumo, H flu, Mycoplasma, Moraxella, Actinomyces – Gram negatives: • more likely with hospitalization, debility, alcoholism, DM, and advanced age • Source may be stomach which can become colonized with these organisms with use of H 2 blockers • Inhalation of Infectious Aerosols – Influenza, Legionella, Psittacosis, Histoplasmosis, TB • Hematogenous Dissemination – Staph aureus – Fusobacterium infections of the retropharyngeal tissues: Lemierre’s syndrome • Direct inoculation and Contiguous Spread – Tracheal intubation, stab wounds
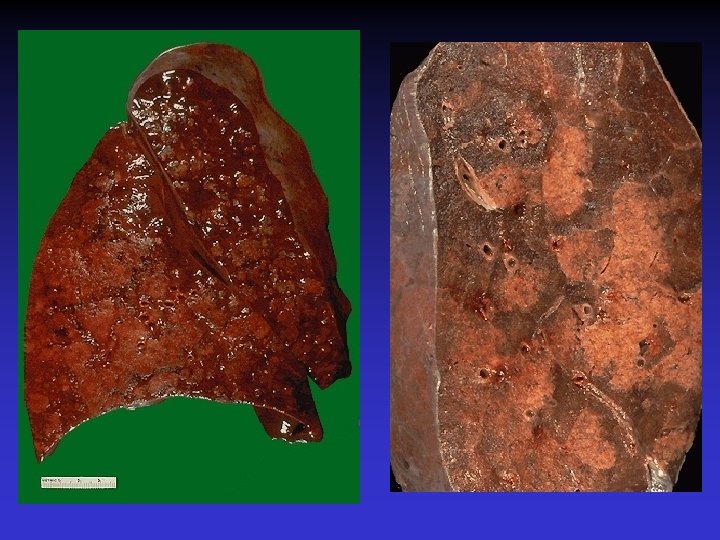
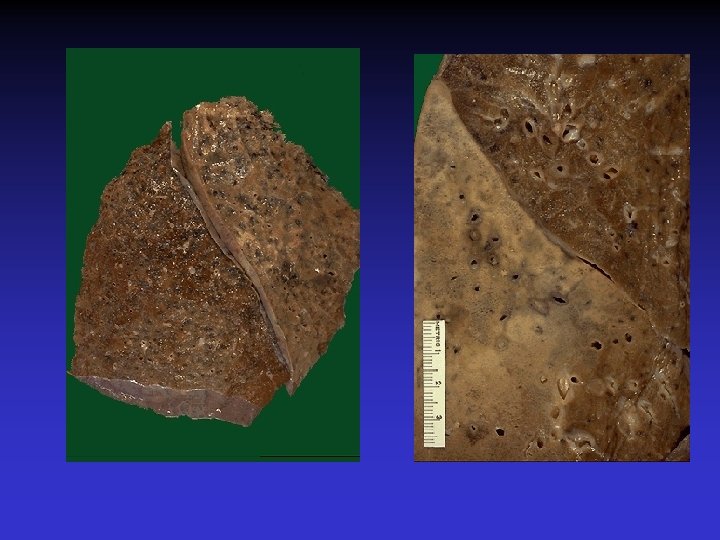
At the left the alveoli are filled with a neutrophilic exudate that corresponds to the areas of consolidation seen grossly with the bronchopneumonia. This contrasts with the aerated lung on the right of this photomicrograph.
Clinical presentation • Pneumonia should be considered in any patient who has newly acquired respiratory symptoms: cough, sputum production, dyspnea, especially if accompanied by fever and abnormal breath sounds and crackles • In elderly or immunocompromised, pneumonia may present with confusion, failure to thrive, worsening of underlying chronic illness, falling
Pneumonia Symptoms • “Typical” pneumonia: sudden onset of fever, cough productive of purulent sputum, pleuritic chest pain • “Atypical”: gradual onset, dry cough, prominence of extrapulmonary symptoms: headache, myalgias, fatigue, sore throat, nausea, vomiting • Includes diverse entities and has limited clinical value
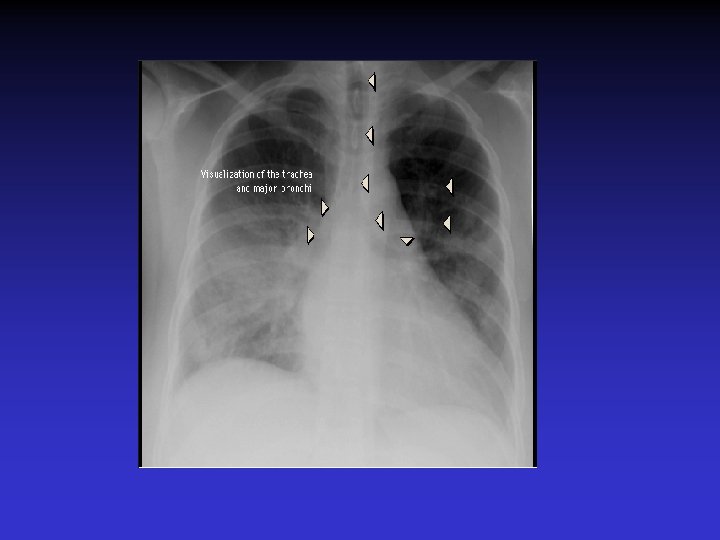
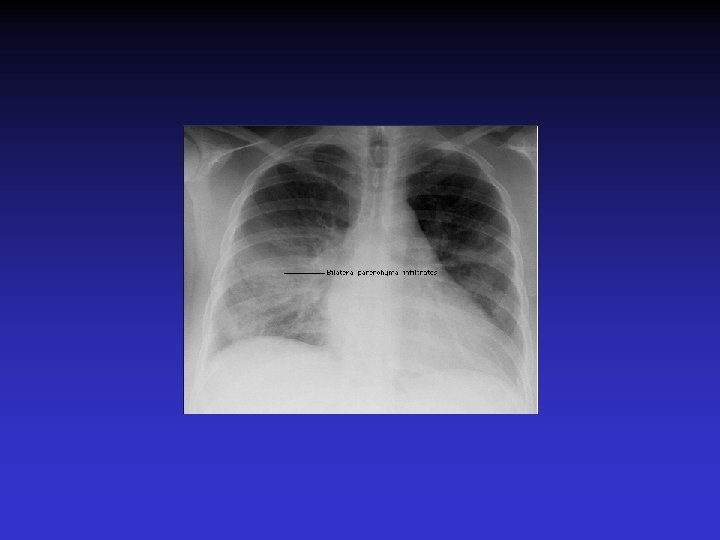
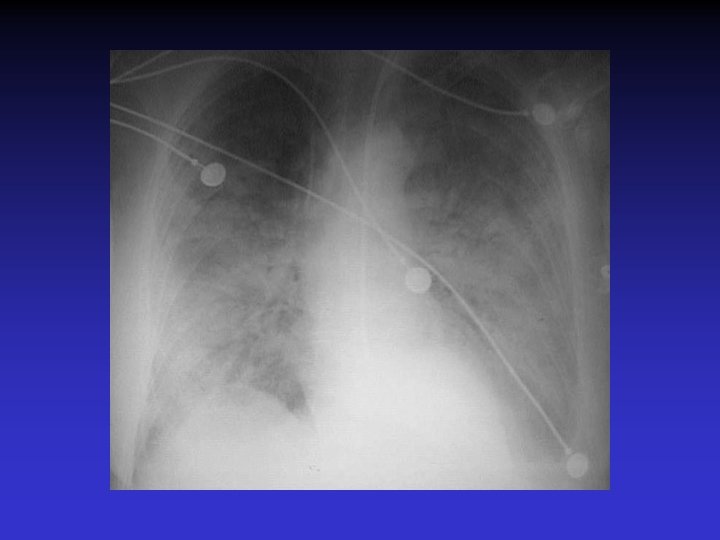
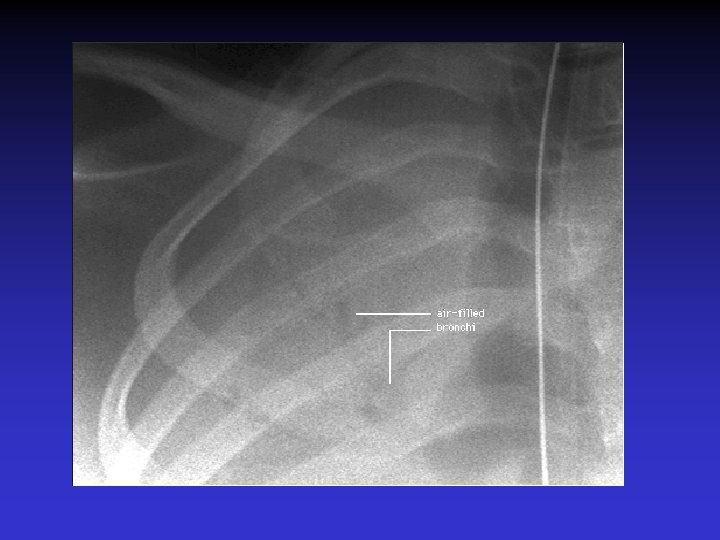
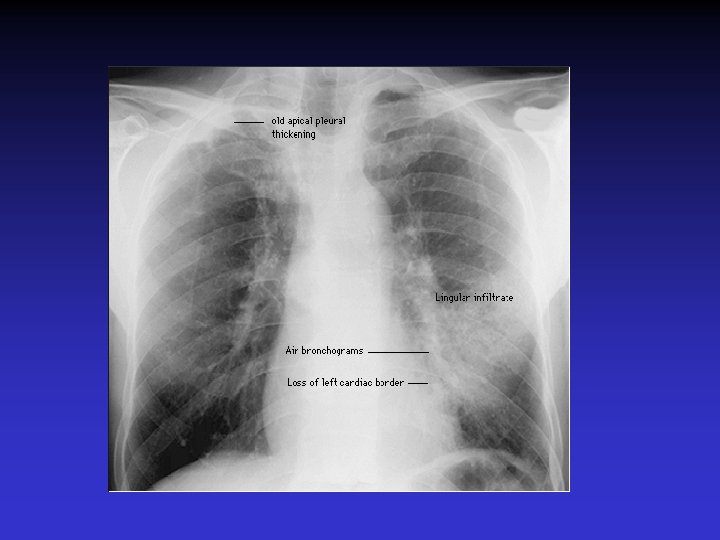
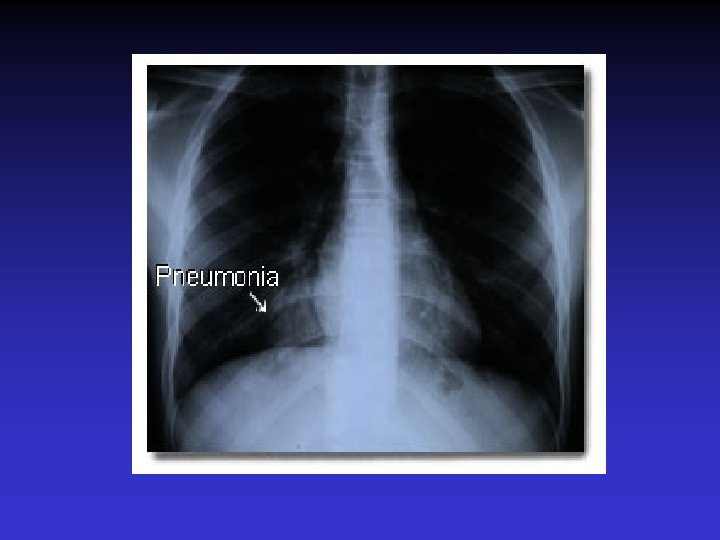
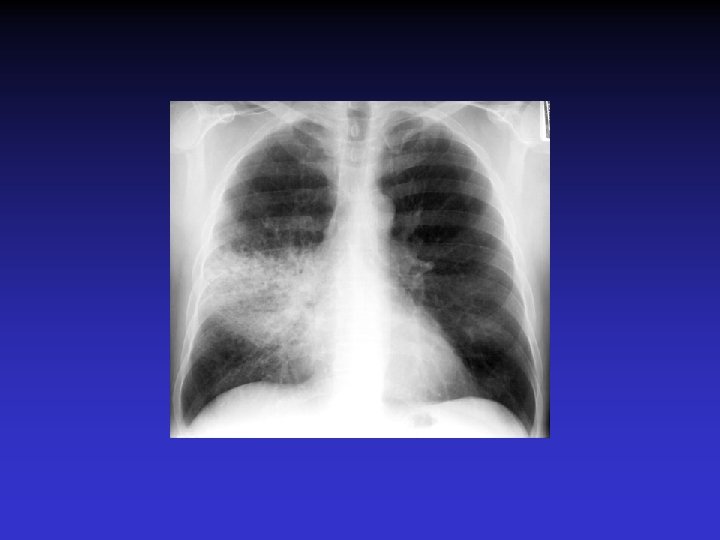
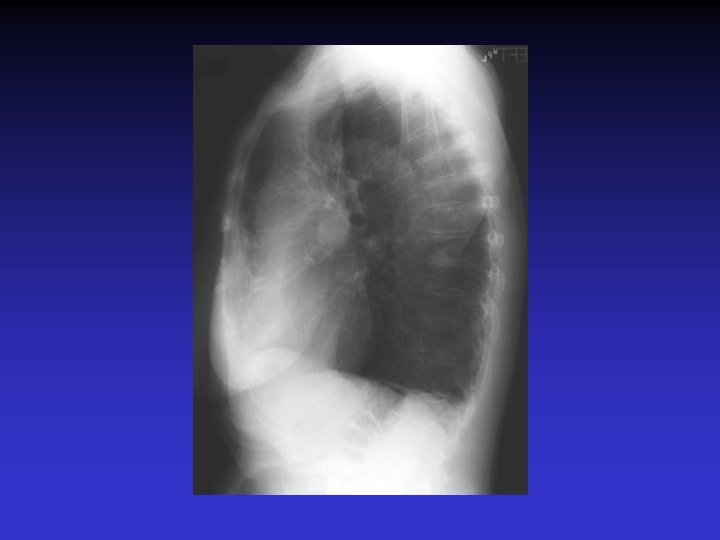
Pneumonia Diagnosis • Radiography: CXR – confirm the presence and location of the pulmonary infiltrate – assess the extent of the infection – detect pleural involvement, pulmonary cavitation, or lymphadenopathy • May be normal when the patient is unable to mount an inflammatory response (immunocompromised) or • is in the early stage of an infiltrative process (hematogenous S. aureus pneumonia)
Pneumonia Diagnosis • Sputum gram stain and culture: • Controversial: no rapid, easily done, accurate, cost-effective method to allow immediate results • Expectorated sputum is frequently contaminated by oropharyngeal flora – Low power magnification to assess squamous epithelial cells – Culture and sensitivity are only accurate if there are <10 epi’s per low power field – Best results if the specimen contains >25 WBCs per LPF • If patient has a productive cough, send sputum for gram stain and culture: could be of use in directing treatment if patient fails to respond to empiric therapy
Pneumonia Diagnosis • Blood cultures are positive in 11% of patients with CAP, more commonly in patients with severe illness • Urine antigen assays for L pneumophila serogroup 1 can be done easily and rapidly. Sensitivity 70% Specificity >90% • Assay for pneumococcal urinary antigen : sensitivity 50 -80% and specificity 90% • Responsible pathogen is not defined in as many as 50% of patients
Pneumonia Diagnosis • Routine laboratory tests: • (CBC, electrolytes, hepatic enzymes) are of little value in determining the etiology of pneumonia, but may have prognostic significance and influence the decision to hospitalization. • Should be considered in patients who may need hospitalization, >65 yr, or with coexisting illness. • All admitted patients should have oxygen saturation assessed by oximetry
Pneumonia Diagnosis • Invasive testing: percutaneous transthoracic needle aspiration or bronchoscopy are not routinely recommended. – May be helpful in: • immunocompromised hosts • suspected tuberculosis in the absence of productive cough • non-resolving pneumonia • pneumonia associated with suspected neoplasm or foreign body • suspected Pneumocystis jirovecii (carinii)
• Pneumonia • Severity • Index
Pneumonia Severity Index
PORT Score • • • Age 55 -10=45 CHF +10 RR +20 HR 124 +10 BUN +20 p. O 2 +10 115 Class IV Mortality 9%
Site of Treatment • Class I or II: Outpatient treatment • Class III: Potential outpatient or brief inpatient observation • Class IV and V: Inpatient • Physician decision making: medical and psychosocial comorbidities, ability to take po, substance abuse, ability to do ADLs
CURB 65 • • • Confusion Urea level (>19) Respiratory rate (>30) Blood Pressure SBP< 90 or DBP <60 Age • Excellent indicator for mortality
ICU Admission • Minor Criteria – – – RR>30/min Pa. O 2/Fi. O 2 <250 Multilobar pneumonia Systolic BP <90 Diastolic BP <60 • Major Criteria – Need for mechanical ventilation – Increase in the size of infiltrates by >50% within 48 hrs – Septic shock – Acute renal failure (uop <80 ml in 4 h or serum Cr>2. 0)
Modifying Factors that Increase the Risk of infection with Specific Pathogens • Penicillin-resistant pneumococci – – – Age >65 B-lactam therapy within the past 3 months Alcoholism Immune suppressive illness (including tx with corticosteroids) Multiple medical comorbidities: DM, CRI, CHF, CAD, malignancy, chronic liver disease – Exposure to a child in a day care center • Enteric gram negatives – – Residence in a nursing home Underlying cardiopulmonary disease Multiple medical comorbidities Recent antibiotic therapy • Pseudomonas aeruginosa – – Structural lung disease (bronchiectasis) Corticosteroid therapy (>10 mg prednisone/day) Broad spectrum antibiotic therapy for > 7 days in past month Malnutrition
Group I: Outpatients No cardiopulmonary disease No modifying factors Organism: Streptococcus pneumonia Mycoplasma pneumonia Chlamydia pneumonia Hemophilus influenzae Miscellaneous Legionella Mycobacterium Fungi Treatment: Advanced generation macrolide(azithromycin or clarithromycin) OR doxycycline
Group II: Outpatient, with cardiopulmonary disease, and/or other modifying factors • • • Organism: Strep pneumonia Mycoplasma Chlamydia Mixed infection Hemophilus influenzae Enteric gram-negatives Viruses Miscellaneous Moraxella, Legionella, anaerobes, TB, fungi • Therapy: • B -lactam (oral cefpodoxime, cefuroxime, high-dose amoxicillin, amoxicillin/clavulanate or parenteral ceftriaxone PLUS • Macrolide or doxycycline OR • Antipneumococcal fluoroquinolone
Group III: Inpatients • • • Organism Strep pneumonia Hemophilus influenzae Mycoplasma Chlamydia Mixed infection Enteric gram-negatives Aspiration Virus Miscellaneous • • • Therapy: 1. Intravenous B lactam: cefotaxime, ceftriaxone, ampicillin/sulbactam, high-dose amipicillin PLUS Intravenous or oral macrolide or doxycycline OR 2. Antipneumococcal fluoroquinolone
ICU Patients • • • Organisms: Strep pneumonia Legionella Hemophilus influenzae Enteric gram-negative bacilli Staphylococcus aureus Mycoplasma Respiratory Viruses Miscellaneous • Therapy: • 1. Intravenous B lactam: cefotaxime, ceftriaxone, ampicillin/sulbactam, high-dose amipicillin • PLUS either • Intravenous or oral macrolide or doxycycline • or • Antipneumococcal fluoroquinolone
ICU Patients with Risks for Pseudomonas aeruginosa • 1. Selected iv antipseudomonal B -lactam (cefepime, imipenem, meropenem, piperacillin/tazobactam) • PLUS iv antipseudomonal quinolone • OR • 2. Selected iv antipseudomonal B -lactam PLUS iv aminoglycoside PLUS either iv macrolide or iv nonpseudomonal fluoroquinolone
Hospital-Acquired Pneumonia • Enteric aerobic gram negative bacilli • Pseudomonas aeruginosa • Staphylococcus aureus • Oral anaerobes • Antipseudomonal cephalosporin (cefepime, ceftazidime) OR Antipseudomonal carbepenem OR B lactam/B -lactamase inhibitor • PLUS • Antipseudomonal fluoroquinolone OR aminoglycoside • PLUS Vancomycin or Linezolid
• Metastasis to skin and CNS • Hyponatremia, AMS, renal and hepatic dysfunction • Night sweats, weight loss • Erythema multiforme, hemolytic anemia, encephalitis, transverse myelitis • Erythema nodosum • Increased risk after Influenzae pneumonia • Staph aureus • Histoplasma • Legionella • Mycoplasma • Nocardia • TB
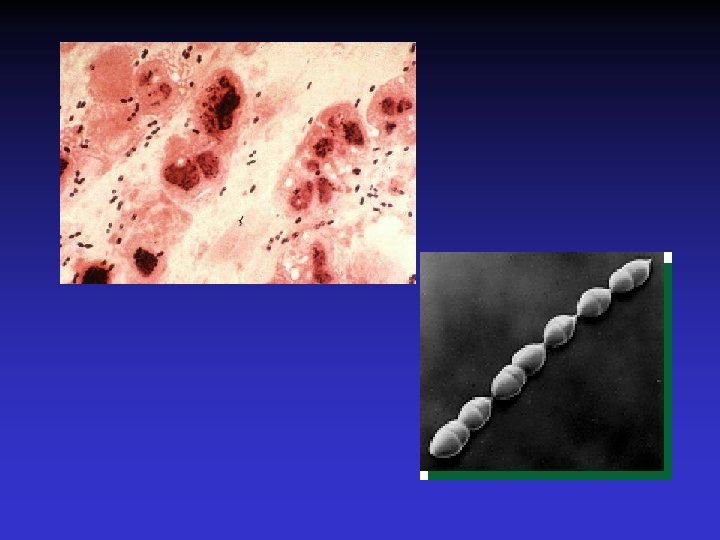
Selected Bacterial Infections Pharyngitis Group A Strep - Streptococcus pyogenes (Many viruses also cause this) Pneumonia Streptococcus pneumoniae Diphtheria Corynebacterium diphtheriae Tuberculosis Mycobacterium tuberculosis Whooping cough - Bordetella pertussis
Spectrum of Respiratory Illnesses in HIV-Infected Patients
Spectrum of Respiratory Illnesses in HIV-Infected Patients
CD 4 Cell Count Ranges for Selected HIV-Related and Non-HIV-Related Respiratory Illnesses Any CD 4 Cell Count Upper respiratory tract illness Upper respiratory tract infection Sinusitis Pharyngitis Acute bronchitis Obstructive airway disease Bacterial pneumonia Tuberculosis Non-Hodgkin lymphoma Pulmonary embolus Bronchogenic carcinoma CD 4 Count ≤ 500 Cells/µL Bacterial pneumonia (recurrent) Pulmonary mycobacterial pneumonia (nontuberculous)
CD 4 Cell Count Ranges for Selected HIV-Related and Non-HIV-Related Respiratory Illnesses CD 4 Count ≤ 200 Cells/µL Pneumocystis pneumonia Cryptococcus neoformans pneumonia/pneumonitis Bacterial pneumonia (associated with bacteremia/sepsis) Disseminated or extrapulmonary tuberculosis CD 4 Count ≤ 100 Cells/µL Pulmonary Kaposi sarcoma Bacterial pneumonia (gram-negative bacilli and Staphylococcus aureus increased) Toxoplasma pneumonitis CD 4 Count ≤ 50 Cells/µL Disseminated Histoplasma capsulatum Disseminated Coccidioides immitis Cytomegalovirus pneumonitis Disseminated Mycobacterium avium complex Disseminated mycobacterium (nontuberculous) Aspergillus spp pneumonia
Virus infections • Respiratory syncytial virus (“RSV”) • Influenza virus Fungal Infections • Coccidiodomycosis (Valley Fever) Coccidioides immitis
Respiratory Syncytial Virus • Enveloped (membrane) RNA virus • Spread by respiratory droplets • Community outbreaks in late fall to spring • Upper respiratory tract infection – epithelial cells • May be fatal in infants
Influenza Virus An enveloped RNA virus Structure
Influenza Virus New human strains every year • Mutations Pandemic strains Genetic Recombinant Viruses • 1957 Asian Flu H 2 N 2 • 1968 Hong Kong Flu H 3 N 2 • 1977 Russian Flu H 1 N 1 Bird Flu Directly from birds • ? ? H 5 N 1
‘H’ and ‘N’ Flu Glycoproteins H – Hemagglutinin • Specific parts bind to host cells of the respiratory mucosa • Different parts are recognized by the host antibodies • Subject to changes N - Neuraminidase • Breaks down protective mucous coating • Assist in viral release
Influenza • Epidemics and pandemics, mostly in winter • Upper respiratory tract infection – epithelial cells • Multivalent killed virus vaccine with strains from the previous year (Grown in embryonated eggs) • Bird flu (H 5 N 1) pandemic in birds
H 1 N 1 2009 (Swine Flu) 67
Influenza A/California/7/2009 (H 1 N 1) 68
Influenza Disease Burden in an Average Year Deaths 25, 000 - 72, 000 Hospitalizations 114, 000 - 257, 500 Physician visits ~ 25 million Infections and illnesses 50 - 60 million Thompson WW et al. JAMA. 2003; 289: 179 -86. Couch RB. Ann Intern Med. 2000; 133: 992 -8. Patriarca PA. JAMA. 1999; 282: 75 -7. ACIP. MMWR. 2004; 53(RR 06): 1 -40.
INFLUENZA: BIOLOGY & IMPACT • Single-stranded, enveloped, RNA virus (orthomyxoviridae family) • Influenza A – Potentially severe illness; epidemic and pandemics – Rapidly changing • Influenza B – Usually less severe illness; may cause epidemics – More uniform • Influenza C – Usually mild or asymptomatic illness
Differences among influenza A, B, and C Body_ID: None Influenza A Influenza B Influenza C Body_ID: T 162001. 50 Genetics 8 gene segments 7 gene segments 10 viral proteins 11 viral proteins 9 viral proteins M 2 unique NB unique HEF unique Body_ID: T 162001. 100 Structure Body_ID: T 162001. 150 Body_ID: T 162001. 200 Host range Table 162 -1. Differences among Influenza A, B, and C Viruses Humans, swine, equine, avian, marine mammals Humans only Humans and swine Antigenic shift and drift. Drift is generally linear Antigenic drift only. More than one variant may cocirculate Antigenic drift only. Multiple variants Body_ID: T 162001. 250 Epidemiology Body_ID: T 162001. 300 Clinical features Body_ID: T 162001. 350 May cause large Severe disease generally Mild disease without pandemics with significant confined to older adults or seasonality mortality in young persons at high risk; pandemics not seen
INFLUENZA: BIOLOGY & IMPACT • Impact – 25 -50 million people contract influenza annually representing and attack rate of 10 -20%. – ~115, 000 hospitalizations per year – ~35, 000 (20, 000 – 40, 000) deaths per year • Causes respiratory tract disease – Sudden onset – More severe pneumonia during pregnancy • No carrier state (but inapparent illness may occur)
INFLUENZA: EPIDEMIOLOGY • • Geographic distribution – global Reservoir: Humans, swine, birds Incubation - 1 to 5 days; usually 2 days Transmission – Droplet (airborne? ) route – Direct contact • Communicability 1. – 1 to 2 days before onset of symptoms to 4 to 5 days post-onset – Attack rates: Up to 60%
Influenza Activity Can Peak From December Through May Month of peak influenza activity during influenza seasons 11 6 4 3 1 www. cdc. gov/nip/publications/pink/flu. pdf. 1
Pandemi
Structure of the Influenza Virus Hemagglutinin (HA) Neuraminidase (NA) M 2 Nucleoprotein (NP) M 1 Polymerase (P) Proteins Adapted from: Hayden FG et al. Clin Virol. 1997: 911 -42.
Viral Nomenclature Type of Nuclear Material Hemagglutinin Neuraminidase A / Sydney / 184 / 93 (H 3 N 2) Virus Geograph Strain Year of subtyp ic origin numb isolatio eed. Department of Health and CDC. Atkinson W, et al. Chapter 13: Influenza. In: Epidemiology and Prevention Diseases, 4 th n er of Vaccine-Preventable Human Services, Public Health Service, 1998, 220 Virus type 1.
Incidence of clinically manifest influenza Mean level of population antibody vs A Hx. Nx Mean level of population antibody vs A Hy. Ny Disease Incidence Pandemic Interpandemic Period Epidemic 1 2 3 4 5 6 7 8 Time in Years 9 10 Introduction of. Significant minor variation A Hx. Nx may hypothetical occur at any of these points. Epidemics A Hx. Nx virus may or may not be associated with such variations 11 12 Mean Population Antibody Level Occurrence of Influenza Pandemics and Epidemics Introduction of hypothetical A Hy. Ny major (new subtype) variant A Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases, 5 th. Hx. Nx ed. 2000: 1829. disappears Modified from Kilbourne ED. Influenza. 1987: 274, with permission.
Pathogenesis of Influenza • Influenza can be transmitted through small or large particle • aerosols or through contact with contaminated surfaces • If not neutralized by mucosal antibodies, virus attacks respiratory tract epithelium • Infection of respiratory epithelial cells leads to cellular dysfunction, viral replication, and release of viral progeny • Release of inflammatory mediators contributes to systemic manifestations of disease Bridges CB et al. Clin Infect Dis. 2003; 37: 1094 -101. Heikkinen T et al. Lancet. 2003; 361: 51 -9.
Clinical Features of Influenza • Sudden onset of symptoms, persist for 7+ days • Incubation period: 1 -4 days, average 2 days • Infectious period of wild type virus: – Adults shed virus typically from 1 day before through 5 days after onset of symptoms – Children shed higher titers for a longer duration than adults ACIP. MMWR. 2004, 53(RR 06)1 -40. Kavet J. Am J Public Health. 1977; 67: 1063 -70. Frank AL et al. J Infect Dis. 1981; 144: 433 -441. Hayden FG et al. JAMA. 1999; 282: 1240 -6.
Clinical Manifestations by Age Group Influenza Sign/Symptom Cough (nonproductive) Fever Childre n Adults Elderl y ++ +++ +++ + Myalgia + + Headache ++ ++ Malaise + + Sore throat + ++ Rhinitis/nasal congestion ++ ++ Abdominal pain/diarrhea + – Nausea/vomiting – Monto AS et al. Arch Intern Med. 2000; 160: 3243 -47. Cox NJ et++ al. Lancet. 1999; 354: 1277 -82. ++++ Most frequent sign/symptom; + Least frequent; – Infrequent + + +++ + +
Influenza Manifestations & Complications Children Frequent Adults Sinusitis, bronchitis, Primary viral pneumonia, bronchiolitis, secondary bacterial pneumonia, croup, pneumonia, sinusitis, acute otitis media bronchitis Rare Encephalopathy, Myositis, rhabdomyolysis, myositis, myocarditis, pericarditis rhabdomyolysis, myocarditis, pericarditis, Reye syndrome, sepsis-like syndrome Exacerbation Cardiovascular, diabetes, Loughlin J et al. Pharmocoeconomics. 2003; 21: 273 -283. Treanor JJ. Influenza virus. In: Mandell GL, Bennett s JE, of Dolin R, eds. Mandell, diabetes, asthma, COPD Douglas, andasthma, Bennett’s Principles and Practice of Infectious Diseases. 5 th ed. Philadelphia, PA: Churchill Livingstone; 2000: 1823 -1849. ACIP. MMWR 2004; 53 (RR 06): 1 -40. underlying cystic fibrosis disease
Patient Groups at Risk for Complications • Increased risk of influenza complications among: – Children <2 years – Children and adolescents receiving long-term aspirin therapy – Children and adults with chronic conditions • Chronic pulmonary, metabolic, or CV disorders • Renal dysfunction • Hemoglobinopathies • Immunosuppression, including HIV infection – Pregnant women – Residents of chronic care facilities – Persons 65 years old ACIP. MMWR. 2004; 53(RR 06): 1 -40.
Complications Pulmonary: Non-Pulmonary: l Primary influenza viral pneumonia l Secondary bacterial pneumonia l Croup l Asthma, COPD, * bronchitis, cystic fibrosis exacerbation l Increased severity of influenza in HIV patients l l l l * Chronic obstructive pulmonary disease Myositis Cardiac complications Toxic shock syndrome Guillain-Barré syndrome Transverse myelitis Encephalitis Reye syndrome
Influenza Diagnostic Testing • Rapid Antigen (EIA) – NP aspirates and swabs only – Detects Influenza A/B nucleoproteins – 1 hour TAT, batched on the hour – Upper and lower respiratory specimens – Detects Influenza A/B, Parainfluenza 1/2/3, Adenovirus and RSV – 24 -72 hour TAT • Real-time RT-PCR – – Upper and lower respiratory specimens Detects Influenza A matrix gene Influenza B validation in progress 24 hour TAT Increase in Sensitivity • Viral Culture (Shell Vial)
INFLUENZA VACCINE: INDICATIONS • • • Healthcare providers Persons >65 years of age Residents of extended care facilities of any age Adults and children with chronic cardio-respiratory illnesses Adults and children with chronic metabolic disorders, immune deficiencies, or immunosuppression Children (6 mo– 18 yr) receiving aspirin (risk for Reye syndrome) Out-of-home caregivers and household contacts of children <6 mo Women who will be pregnant during influenza season Children aged 6 -23 months People who want to avoid influenza
INFLUENZA VACCINE (Inactivated): CONTRAINIDATIONS • Hypersensitivity to eggs or vaccine components • Acute febrile illness (postpone vaccine) • Active neurologic disorder characterized by changing neurologic findings. Previous Guillain-Barre or other neurologic illnesses related to previously administered vaccine • Pregnancy or breastfeeding NOT a contraindication
14 Aralık 2009 • Ülkemizde pandemik influenzadan 415 kişi öldü. • 27’si gebe/lohusa 89
Pandemik Gribe bağlı ölümlerin haftalara göre dağılımı, 19 Ekim-6 Aralık 2009, Türkiye (n = 320) 90
2010 -2011 Aşılaması Ağustos 2010 da başlandı Pandemic H 1 N 1 aşısı İlk dalga Mevsimsel Influenza aşısı 2. dalga 2009 İçerik A (H 1 N 1) 2009 A (H 3 N 2) Olası salgın B 2010 H 1 N 1 H 3 N 2 B
TUS 2012 • Üç hafta-4 yaş arasındaki çocuklarda, toplum kaynaklı pnömoninin en sık bakteriyal etkeni aşağıdakilerden hangisidir? • A) Mycoplasma pneumoniae • B) Haemophilus influenzae • C) Staphylococcus aureus • D) Streptococcus pneumoniae • E) Chlamydia trachomatis
TUS 2012 • Üç hafta-4 yaş arasındaki çocuklarda, toplum kaynaklı pnömoninin en sık bakteriyal etkeni aşağıdakilerden hangisidir? • A) Mycoplasma pneumoniae • B) Haemophilus influenzae • C) Staphylococcus aureus • D) Streptococcus pneumoniae • E) Chlamydia trachomatis
TUS 2012 • Okul çağındaki çocuklarda trakeobronşite ve pnömoniye en sık neden olan mikroorganizma aşağıdakilerden hangisidir? • A) Chlamydia pneumoniae B) Bordetella pertussis C) Mycoplasma pneumoniae D) Legionella pneumophila E) Haemophilus influenzae
TUS 2012 • Okul çağındaki çocuklarda trakeobronşite ve pnömoniye en sık neden olan mikroorganizma aşağıdakilerden hangisidir? • A) Chlamydia pneumoniae B) Bordetella pertussis C) Mycoplasma pneumoniae D) Legionella pneumophila E) Haemophilus influenzae
TUS 2010 • Aşağıdakilerden hangisi akut bronşiyolit tedavisinin ilkelerinden biri değildir? • • A) Bronşiyal obstrüksiyonun kaldırılması B) Asiklovir tedavisi C) Hipoksemi ve asidozun düzeltilmesi D) Potansiyel kardiyak komplikasyonların önlenmesi • E) İkincil bakteriyal enfeksiyonların tedavisi
TUS 2010 • Aşağıdakilerden hangisi akut bronşiyolit tedavisinin ilkelerinden biri değildir? • • A) Bronşiyal obstrüksiyonun kaldırılması B) Asiklovir tedavisi C) Hipoksemi ve asidozun düzeltilmesi D) Potansiyel kardiyak komplikasyonların önlenmesi • E) İkincil bakteriyal enfeksiyonların tedavisi
TUS 2013 • Aşağıdakilerden hangisi, influenza komplikasyonları için bir risk faktörü değildir? • A) Gebelik B) Diabetes mellitus C) HIV enfeksiyonu D) Splenektomi E) Astım
TUS 2013 • Aşağıdakilerden hangisi, influenza komplikasyonları için bir risk faktörü değildir? • A) Gebelik B) Diabetes mellitus C) HIV enfeksiyonu D) Splenektomi E) Astım
TUS 2013 • Bir aylık erkek bebek, doğumdan 3 hafta sonra başlayan öksürük yakınmasıyla getiriliyor. Ateşi olmayan bebeğin fizik muayenesinde takipne ve krepitan raller saptanıyor ve hemogramda lenfositoz ile eozinofili gözleniyor. Bu bebekteki tablodan sorumlu en olası etken aşağıdakilerden hangisidir? A) Streptococcus agalactiae B) Mycoplasma pneumoniae C) Chlamydia trachomatis D) Solunum sinsityal virus E) Staphylococcus aureus
TUS 2013 • Bir aylık erkek bebek, doğumdan 3 hafta sonra başlayan öksürük yakınmasıyla getiriliyor. Ateşi olmayan bebeğin fizik muayenesinde takipne ve krepitan raller saptanıyor ve hemogramda lenfositoz ile eozinofili gözleniyor. Bu bebekteki tablodan sorumlu en olası etken aşağıdakilerden hangisidir? A) Streptococcus agalactiae B) Mycoplasma pneumoniae C) Chlamydia trachomatis D) Solunum sinsityal virus E) Staphylococcus aureus
TUS 2013 • Aşağıdaki mikroorganizmalardan hangisi, fagolizozom füzyonunu engelleyerek konak savunmasından kaçabilecek bir mekanizmaya sahiptir? • A) Mycobacterium tuberculosis B) Staphylococcus aureus C) Haemophilus influenzae D) Bacillus anthracis E) Streptococcus pneumoniae
TUS 2013 • Aşağıdaki mikroorganizmalardan hangisi, fagolizozom füzyonunu engelleyerek konak savunmasından kaçabilecek bir mekanizmaya sahiptir? • A) Mycobacterium tuberculosis B) Staphylococcus aureus C) Haemophilus influenzae D) Bacillus anthracis E) Streptococcus pneumoniae
TUS 2013 • Pnömoni tablosuyla getirilen 1 yaşındaki bebekten alınan nazofarengeal sürüntü örneğinin direkt immünofloresan incelemesinde çok nükleuslu dev hücreler görülmüştür. Bu bebekteki en olası etken aşağıdakilerden hangisidir? A) Coronavirus B) Adenovirus C) İnfluenza virus tip A D) Solunum sinsityal virus E) Rhinovirus
TUS 2013 • Pnömoni tablosuyla getirilen 1 yaşındaki bebekten alınan nazofarengeal sürüntü örneğinin direkt immünofloresan incelemesinde çok nükleuslu dev hücreler görülmüştür. Bu bebekteki en olası etken aşağıdakilerden hangisidir? A) Coronavirus B) Adenovirus C) İnfluenza virus tip A D) Solunum sinsityal virus E) Rhinovirus
TUS 2014 • Öksürük, ateş, balgam, plevral ağrısı olan hastada balgam incelemesinde alfa hemolitik streptokok görüldü. Tanıya yönelik hangi test yapılmalı? a) optokin, b) basitrasin, c) dnaz, d) üreaz
TUS 2014 • Öksürük, ateş, balgam, plevral ağrısı olan hastada balgam incelemesinde alfa hemolitik streptokok görüldü. Tanıya yönelik hangi test yapılmalı? a) optokin, b) basitrasin, c) dnaz, d) üreaz
TUS 2015
TUS 2015
QUESTIONS