Rational Antibiotic Use Meral Snmezolu MD Infectous Diseases

Rational Antibiotic Use Meral Sönmezoğlu, MD Infectous Diseases Department YEDİTEPE UNIVERSITY HOSPITAL

Antibiotic Use • Antibiotics are among the most commonly used types of drugs • have had a significant impact to decrease morbidity and mortality in infectious diseases. • However, irrational use of antibiotics leads to : – – – resistance, treatment failure, waste of scarce resources.

Is an antibiotic necessary ? § Useful only for the treatment of bacterial infections § Not all fevers are due to infection § Not all infections are due to bacteria § There is no evidence that antibiotics will prevent secondary bacterial infection in patients with viral infection

Antibiotic Use • Generally 40 -50% misuse • Over 20% of yearly drug consumption is antibiotics • Problems is not only for developing countries • In USA, 50 -70% of URTI are prescribed antibiotics • Of the 20% all antibiotics are prescribed for RTI

Drug Purchases through the Private Sector • 50 -90% of all drug purchases are private – 25% to 75% illness episodes self-medicated – 1/2 consumers buy 1 -day supply at a time – 50% of people worldwide fail to take drugs correctly • Results not always therapeutic – – over-treatment of mild illness inadequate treatment of serious illness mis-use of anti-infective drugs over-use of injections WHO, Dept. Essential Drugs and Medicines Policy

ANTIBIOTICS in TURKEY • In Turkey 26. 3% of total drug expenditure in 1996 • 22. 4% of all drugs *. • Yearly 400 million USD *Turk. J. Hosp. Infect. 2000; 4: 144 -147 **IMS Türkiye 2002

Medicine in Turkey Türkiye İlaç Pazarında dağılım Dünya Kalp-Dolaşım Sistemi % 20 Merkez Sinir Sistemi % 17 Gastro-intestinal Sistem % 15 Solunum Sistemi % 10 Anti-enfektifler % 9 Lokomotor Sistem % 6 Ürogenital Sistem % 5. . . Türkiye % 15 % 11 % 12 % 9 % 22 % 11 % 4 SCRIP No: 2809/10 20 -25 Aralık 2002, s. 19 - IMS Türkiye, 2002
 557’si anti-enfektif,")
Antiinfectives in Turkey Türkiye pazarda bulunan toplam 3. 346 ilacın (form olarak) 557’si anti-enfektif, 355’i antibiyotik alanındadır. Antibiotics % 10, 5 IMS Türkiye, 2002

%14. 7

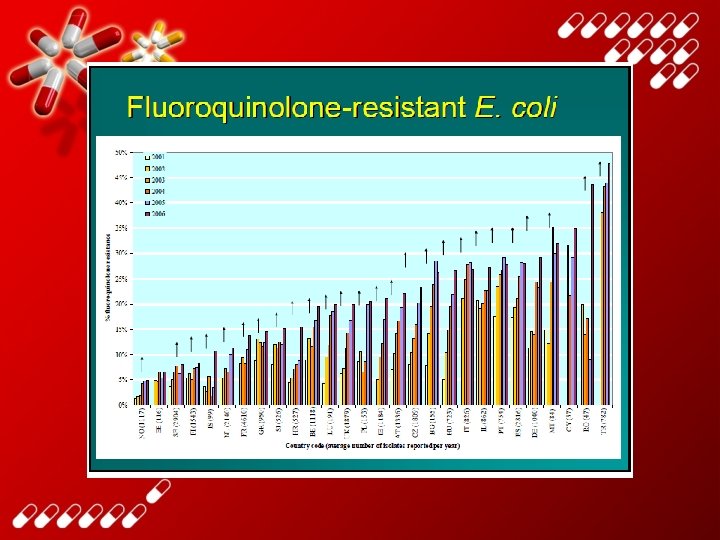
Antibiotic use in eastern Europe: a cross-national database study in coordination with the WHO Regional Office for Europe Lancet Infect Dis, 2014

C hi to ni nd s ly iu m Fr an ce G re ec e Tu rk ey lg All Ita DDDs per 1 000 population, per day Be Sw a ed en La tv ia H un ga Sl ry ov en ia Is ra el G er m an y N or w ay Ko re a Au st ria D en m ar k Fi nl an Li d th ua ni a C an ad C ze a ch R O EC ep. U ni te D (2 d 9) Ki ng do m Ic el an d ¹ Po rtu ga Au l st ra lia Po l Sl an ov d ak R ep Ire. la nd S Lu p xe ain m bo ur g Es le 45 rla he N et Europe 2 nd line (where reported) 40 35 30 25 20 15 10 5 0
")
Overall volume of antibiotics prescribed, 2013 (05 Oct 2015)

WHO • Almost ten years since the WHO global strategy for containment of antimicrobial resistance was published, • the World Health Organization has announced this topic as theme for World Health Day in 2011

Antimicrobial resistance is theme of WHO's World Health Day 2011. • WHO strongly recommends that governments focus control and prevention efforts in four main areas: – surveillance for antimicrobial resistance; – rational antibiotic use, including education of healthcare workers and the public in the appropriate use of antibiotics; – introducing or enforcing legislation related to stopping the selling of antibiotics without prescription; and – strict adherence to infection prevention and control measures, including the use of hand-washing measures, particularly in healthcare facilities.

• The global action plan sets out five strategic objectives: • to improve awareness and understanding of antimicrobial resistance; • to strengthen knowledge through surveillance and research; • to reduce the incidence of infection; • to optimize the use of antimicrobial agents; and • develop the economic case for sustainable investment that takes account of the needs of all countries, and increase investment in new medicines, diagnostic tools, vaccines and other interventions.

World Health Day – 7 April 2011 Antimicrobial resistance: no action today, no cure tomorrow

Avrupa Antibiyotik Farkındalık Günü hakkında: � 18 Kasım, Avrupa Antibiyotik Farkındalık Günü olarak kabul edilmiştir. � Avrupa Antibiyotik Farkındalık Günü hem toplumda hem de hastanelerde akılcı antibiyotik kullanımına yönelik ulusal kampanyalar için bir platform hazırlamakta ve destek sağlamaktadır. � Ülkemizde de bu amaçla bir kampanya yapılmaktadır. 19



1980 -2011 Infection Timeline • Your Text here • Lorem ipsum dolor sit amet, consectetuer adipiscing elit, sed diam nonummy nibh euismod tincidunt ut laoreet dolore magna aliquam erat volutpat. Ut wisi enim ad minim veniam, quis nostrud exerci tation ullamcorper suscipit lobortis nisl ut aliquip ex ea commodo consequat. • Duis autem vel eum iriure dolor in hendrerit in vulputate velit esse molestie consequat, vel illum dolore eu feugiat nulla facilisis at vero eros et accumsan et iusto odio dignissim qui blandit praesent luptatum zzril delenit augue duis dolore te feugait nulla facilisi.

 doi:")
Mortality due to infections DM Morens et al. Nature 463, 122 -122 (2010) doi: 10. 1038/nature 08554

3, 29 1, 67 1, 22 0, 43 0, 42 0, 2 2, 6 1, 75 0, 07 0, 02 4, 1 4, 29 37, 93 4, 76 6 9, 67 21, 58 D N o S e l E o a D n lp ş S id u lı Y iğ o n a m G a n e ku zs S e rim i P in a risa E e n ild n il K n rd ta u m sa o fin ye tr n e rü m u te jka ira m e stm izb i n ia e o h iyle h la to ris a n rzt lm a

Medical error—the third leading cause of death in the US BMJ 2016; 353 (Published 03 May 2016)

Mortality due to infections Total death rate worldwide 41% of all diseases are infections all over the world (WHO, 2002)

Mortality due to infections

Mortality effect of appropriateness

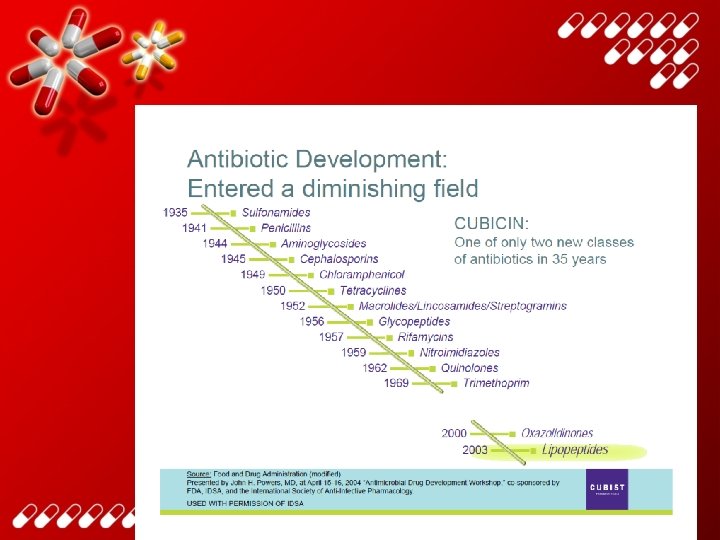
New antibiotic development

New antibiotic development

Why new antibiotic? • Bacteria more rapid than antibiotics R ta s i es b t n a i r te c a

Factors Contributing to Antibiotic Overuse • . Factor Prescriber Lack of education Suboptimal approach to diagnosis and treatment Expectations Economics Patient Belief that all infections require antibiotic treatment Patients expect antibiotics; Belief that antibiotics are pressure to maintain effective for viral relationship infections; "help" from physician represented by a prescription Lack of time in explaining Need to return to daily the lack of need for activities antibiotics Adapted from: Dickerson LM, Mainous AG, Carek PJ. The pharmacists's role in promoting optimal antimicrobial use. Pharmacotherapy. 2000; 20(6): 711 -723.

Rational use of drugs Requires that; • The patients receive medications appropriately • to their clinical needs, • in doses that meet • their own individual requirements for an adequate period of time, • at the lowest cost • to them and their community The conference of experts on the rational use of drugs, convened by the WHO

Rational use of drugs • correct drug • appropriate indication • appropriate drug considering efficacy, safety, suitability for the patient, and cost • appropriate dosage, administration, duration • no contraindications • correct dispensing, including appropriate information for patients • patient adherence to treatment

Rational antibiotic use • Hospital Antibiotic Policies • Hospital Antibiotic Committies

When Irrational use • • Increased treatment costs. Interference with patient’s normal flora. Selection of drug resistant organisms. Increased incidence of untoward side effects

Consequences of inappropriate antibiotic use • Antimicrobial resistance. • Adverse drug reactions and medication errors. • Lost resources. • Eroded patient confidence.
: 445 -458 •")
Adverse drug events Review by White et al, Pharmacoeconomics, 1999, 15(5): 445 -458 • 4 -6 th leading cause of death in the USA • Estimated costs from drug-related morbidity & mortality 30 million-130 billion US$ in the USA • 4 -6% of hospitalisations in the USA & Australia • commonest, costliest events include bleeding, cardiac arrhythmia, confusion, diarrhoea, fever, hypotension, itching, vomiting, rash, renal failure WHO, Dept. Essential Drugs and Medicines Policy



Overuse and misuse of antimicrobials contributes to antimicrobial resistance • Malaria – choroquine resistance in 81/92 countries • Tuberculosis – 2 - 40 % primary multi-drug resistance • Gonorrhoea – 5 - 98 % penicillin resistance in N. gonorrhoeae • Pneumonia and bacterial meningitis – 12 - 55 % penicillin resistance in S. pneumoniae • Diarrhoea: shigellosis – 10 -90+ % amp, 5 -95% TMP/SMZ resistance WHO, Dept. Essential Drugs and Medicines Policy Source: DAP, EMC, GTB, CHD (199

Resistant bacteria Resistant Gram-positive bacteria PRSP Penicillin resistant Streptococcus pneumoniae MDRSP Multi-resistant Streptococcus pneumoniae MRSA Metisilin resistant Staphylococcus aureus VRSA Vancomycin resistant Staphylococcus aureus VISA (GISA) Vancomycin (Glycopeptide) intermediate Staphylococcus aureus VRE (GRE) Vancomycin (Glycopeptide) resistant Enterococcus
 – EU most seen resistant bacteria")
Meticillin-resistant S. aureus (MRSA) – EU most seen resistant bacteria

VRE

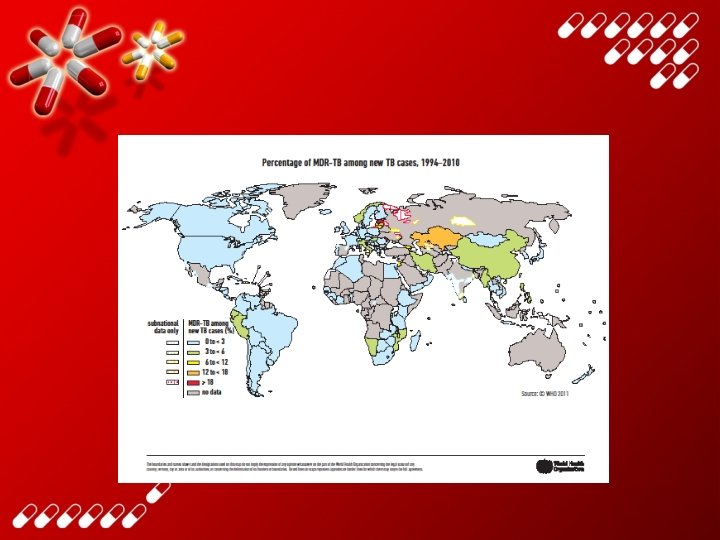
Prevalence of MDR Tuberculosis among New Cases of Tuberculosis, 2007, and Countries with at Least One Reported Case of XDR Tuberculosis as of December 2008 Donald P and van Helden P. N Engl J Med 2009; 360: 2393 -2395

YEDİTEPE MİKROORGANİZMALAR 2010 2011 2012 2013 2014 Staphylococcus aureus suşlarında MRSA 6, 1% 2, 9% 7, 7% 2, 8% 4, 7% Klebsiella pneumoniae suşlarında ESBL E. coli suşlarında ESBL 2, 2% 5, 0% 1, 7% 4, 8% 16, 7% 10, 9% 24, 5% 9, 3% 41, 6% 22, 8% Pseudomonas aeruginosa suşlarında karbapeneme dirençli Olanlar 33, 6% 20, 4% 51, 1% 35, 2% 54, 2% Acinetobacter baumannii suşlarında karbapeneme dirençli olanlar 78, 9% 62, 5% 83, 3% 61, 0% 72, 2% 9, 1% 6, 4% 6, 3% 10, 7% 7, 1% 1, 4% 6, 5% 20, 0% 5, 0% 1, 2% 14, 3% 9, 9% 13, 8% 25, 0% 83, 3% 51, 0% 74, 4% 73, 2% Tüm kan kültürleri arasında Candida spp. Vankomisin Dirençli Enterekoklar Penisilin Dirençli Pnömokoklar Metisilin Dirençli Koagüloz Negatif Stafilokoklar

Choice of antimicrobial agent Based on three main factors: • Etiological agent • Patient-related factors • Antibiotic-related factors

Antibiotic choice: Etiological agent It is the most effective, least toxicity and the narrowest selection Based on : * identification of bacteria * sensitivity test * interpretation in the content of the overall clinical picture * the AB of choice directed to M. O

Antibiotic choice: Patient-related factors • • Age Physiological factors Comorbidities Genetic factors Pregnancy Site and severity of infection Allergies
 profile – – • • • Absorption")
Antibiotic choice: Antibiotic-related factors • Pharmacokinetic/pharmacodynamic (PK/PD) profile – – • • • Absorption Excretion tissue levels, peak levels, AUC, Time above MIC Toxicity and other adverse effects Drug-drug interactions Cost

Introduction • Pharmacokinetics is the study of what an organism does with a dose of a drug – kinetics = motion – Absorbs, Distributes, Metabolizes, Excretes • Pharmacodynamics is the study of what the drug does to the body – dynamics = change 63

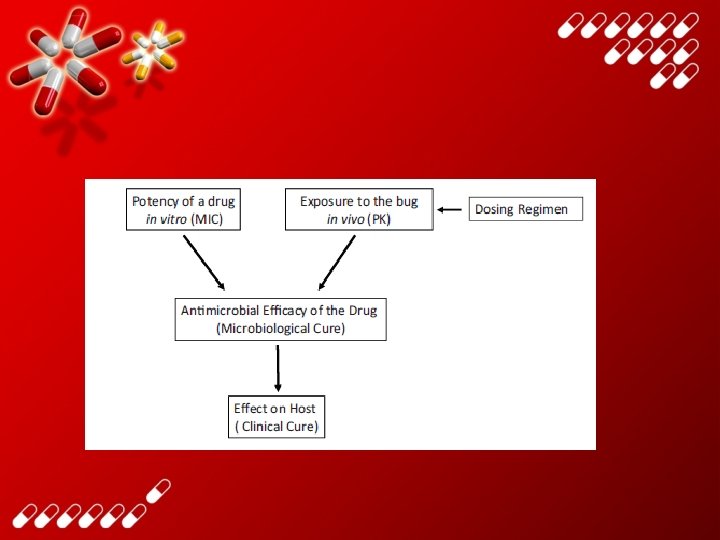
PK/PD • PK/PD of antimicrobial agents describes the triangular relationship between – the potency of a drug against a micro-organism, – subject exposure to a drug – and drug effects
, C_trough • The effect of")
Pharmacokinetics • Endpoints – AUC, Cmax, Tmax, half-life (terminal), C_trough • The effect of the drug is assumed to be related to some measure of exposure. (AUC, Cmax, C_trough) 65
 Area Under the Curve (AUC/MIC) MIC Time above")
Antimicrobial activity Drug Concentration Peak (Peak/MIC) Area Under the Curve (AUC/MIC) MIC Time above MIC Time overall amount of drug in the bloodstream after a dose.
 Area Under the Curve 30 20 10 Area under MIC 90")
Pharmacokinetics Concentration (mg/L) Area Under the Curve 30 20 10 Area under MIC 90 the curve Time (hours) AUC = Initial concentration / Elimination rate constant AUIC = AUC ( drug concentration) / MIC 90 AUIC Preferably 250 but usable if > 125

How to restrict antibiotic usage • • . Don’t use prophylactic antibiotics • Consider carefully whether antibiotics are needed • Avoid broad spectrum antibiotics • Always take a blood culture • Obtain blood culture report at 36 -48 hours • Shorten duration of treatment • Stop antibiotics when no infection evident at 36 -48 hours

Strategies to Improve Use of Drugs Educational: ü Inform or persuade – Health providers – Consumers Managerial: ü Guide clinical practice – Information systems/STGs – Drug supply / lab capacity Use of Medicines Economic: ü Offer incentives – Institutions – Providers and patients Regulatory: ü Restrict choices – Market or practice controls – Enforcement WHO, Dept. Essential Drugs and Medicines Policy

TUS 2015

TUS 2015

THANK YOU
- Slides: 74