Hypertension Karolina Narbska Oddzia Kliniczny Pediatrii i Nefrologii

Hypertension Karolina Narębska Oddział Kliniczny Pediatrii i Nefrologii Wojewódzki Szpital Specjalistyczny dla Dzieci i Dorosłych w Toruniu

Hypertension - general informations - One of the most common disease in population ~30% of adult people. - In children ~ 1 -3% young population and mainly it has secondary character ( secondary hypertension ). - Main causes of hypertension in pediatrics are acquired and congenital renal diseases. The younger hypertensive child is, the bigger likelihood of secondary hypertension is!!!

Hypertension- general information continued - Primary hypertension refers to older children ( over 10 yrs) and it is strongly connected with obesity and lifestyles risk factors. It has unknown origin ( genetic and environmental factors ) There also known 9 types of monogenic hypertension, like e. g. Liddle’a syndrome, Gordon syndrome, etc.

Hypertension - etiopathogenesis Blood pressure depends on CO and TPR according to the following formula: RR = CO ( cardiac output) x TPR ( total peripheral resistance ) CO depends on the left ventricular contractility and volemia. TPR depends on contraction vessels factors and the main is RAAS ( renineangiotensine-aldosterone system ).

RAAS Angiotensinogen RENINE Angiotensin I Angiotensinase ANGIOTENSIN II Angiotensin receptors Vessels contraction Symphaticotony Angiotensin III Aldosterone release Na+ retention Fluid retension Increase of the TPR Increase of the fluid volume Increase of the blood pressure

Hypertension - definition Hypertension is defined as average systolic and/or diastolic blood pressure greater than the 95 th percentile for: - gender - age - hight percentile measured on at least 3 separate occasions.

Normal blood pressure is defined as systolic and/or diastolic blood pressure lower than the 90 th percentile for age, gender, height percentile.

Prehypertension is defined as systolic and/or diastolic blood pressure between the 90 th and 95 th percentile for age, gender and height percentile, but also as in adults, children and adolescents whose blood pressure is greater than 120 mm. Hg ( systolic ) and/or 80 mm. Hg ( diastolic ) are also classified as prehypertensive

„White-coat” hypertension White-coat hypertension refers to the patients, whose blood pressure is greater than the 95 th percentile in the physicians office, but less than the 90 th percentile outside a clinical setting.

Stages of hypertension • • • Stage 1 hypertension Stage 2 hypertension Severe hypertension Hypertensive urgency Hypertensive emergency

Stage 1 hypertension is defined as blood pressure levels ranging from the 95 th to 5 mm. Hg above the 99 th percentile. Asymptomatic patients with stage 1 hypertension may undergo a diagnostic evaluation before initiation of treatment

Stage 2 hypertension is defined as blood pressure levels greater than 5 mm. Hg above the 99 th percentile. Patients with stage 2 hypertension should undergo more timely evaluation and initiation of hypotensive therapy. Symptomatic patients with stage 2 hypertension require immediate pharmacologic treatment and consultation with an expert.

Severe hypertension is defined as blood pressure levels greater than 30 mm. Hg above the 99 th percentile for age, gender and hight percentile.

Hypertension urgency Impending organ failure during hypertension, usually with unspecific symptoms like headaches and vomiting.

Hypertension emergency • Done or ongoing organ damage during hypertension, most often leading to organ failures, with the symptoms of encephalopathy. • Those hypertension emergency stages require immediate intervention.
 measurement: -")
Hypertension - measurement • The rules of blood pressure ( BP ) measurement: - Child shouldn’t eat or drink for at least 30 min before measurement - Child should rest in a sitting position for at least 5 minutes with feet on the floor and arm supported on the heart level - The cuff bladder should cover 80% to 100% of the arm circumference and two thirds of length of the upper arm - Remember: smaller cuff sizes result in an increase of blood pressure and bigger cuff sizes result in a decrease of blood pressure!!! - The cuff should be inflated to a pressure 20 to 30 mm. Hg higher than the patient’s systolic blood pressure and then deflated at 2 to 3 mm. Hg each second - Measurement should be done on the right arm

Measurement - continued Systolic pressure - occurs when the first sound is heard during cuff deflation ( the first Korotkoff sound ) Diastolic pressure - occurs at the point before disappearance of sounds ( the second Korotkoff sound )


Measurement - continued • During the first examination the blood pressure should be measured on four limbs • In babies and infants untill they reach vertical position the blood pressure levels on lower limbs are lower than on upper limbs • In babies while they are sleeping the systolic blood pressure levels are lower by 5 -7 mm. Hg. • In a 2 -year-old child, who can stand vertically, the blood pressure levels on lower limbs become about 20 mm. Hg greater than on upper limbs; in adolescents about 30 -40 mm. Hg greater.

Measurement - continued • Next measures should be taken on the abducted right arm laying on the level of the heart. • Every measurement should be repeated 2 or 3 times per an examination. • The difference of measurement between two arms greater than 5 mm. Hg must be notified in patient’s card.
? • In children aged of")
When to start to measure blood pressure ( BP)? • In children aged of three or more the BP should be measured at least once a year and during routine examination • In children under the age of three the BP should be measured in the following situations: - When a perinatal history is affected: prematurity, LBW, intensive therapy during perinatal period - Congenital anomalies - Recurrent urinary tract infections, chronic kidney disease - Tumors - When drugs effecting BP are used - Diseases connected with hypertension ( neurofibromatosis, hyperthyroidism )

ABPM - ambulatory blood pressure monitoring ABPM method assesses: - 24 -hour blood pressure measurement - variability of 24 -hour blood pressure referring to different periods of day and night, during some activities ABPM results have the meaning in diagnosis, prognosis and monitoring of the treatment. The norms of ABPM are published for children from 120 cm height.
 systolic")
ABPM - assessment • MSBP - stands for mean ( 24 -hour ) systolic blood pressure • MDBP - stands for mean ( 24 -hour ) diastolic blood pressure • Loads of BP ( percent of blood pressure levels greater than the 95 th percentile ) during the day and night ( norm less than 20% ). • Dipping of BP in the night (norm is minimum 10%) • The lack of night dipping of BP is an extra risk factor of cardiovascular incidents, especially in patients with diabetes.

ABPM – indications - Suspicion of the „white coat” hypertension Organ changes in patients with prehypertension Paroxysmal hypertension Resistance to drugs hypertension Assessment of night blood pressure or suspicion of high blood pressure in the night - Assessment of effectiveness hypotensive treatment in patients with too big reduction of blood pressure - Assessment of indications for hypotensive treatment

Hypertension in ABPM • Mean 24 -hour systolic and/or diastolic blood pressure greater than the 95 th percentile for age, gender and height. ( We use special ABMP percentile charts )

MAP – mean arterial pressure MAP is defined as hypothetic mean blood pressure during one cycle of the heart MAP= DP+1/3 ( SP-DP ) Norma: 75 -100 mm. Hg A normal MAP has clinical meaning in supporting organ perfusion ( good blood flowing ). MAP under 60 mm. Hg results bed perfusion and hypoxia.

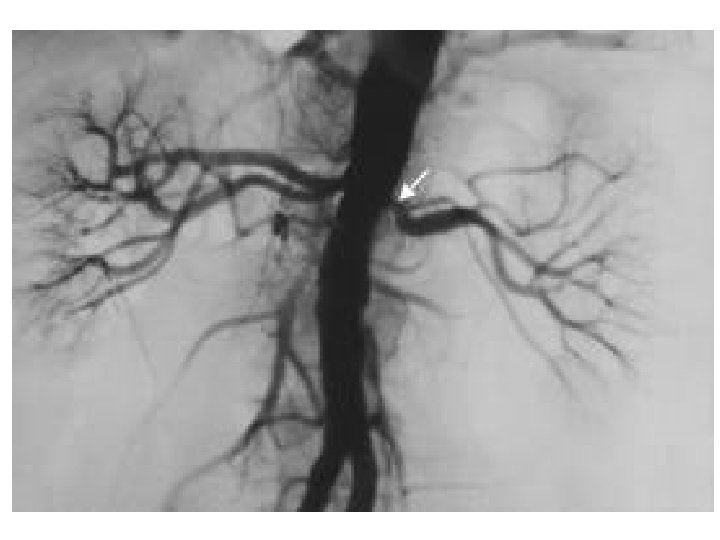
Causes of secondary hypertension whatever the age 1. Hypertension in kidney diseases: - renal parenchymal diseases secondary to reflux nephropathy, obstructive uropathy, chronic renal infections ( pyelonephritis! ) - primary and secondary glomerulonephritis, - polycystic kidney diseases, - Wilm’s tumour - chronic kidney diseases 2. Renovascular hypertension – eg. bilateral renal artery stenosis ( often with Co. A )

Causes of secondary hypertension whatever the age 3. Endocrine-origin hypertension: - pheochromocytoma - primary hyperaldosteronism ( Conn syndrome ) – hypernatremia with hypokaliemia - Cushing syndrome - Congenital adrenal cortex steroidogenesis abnormalities ( like eg congenital adrenal cortex hypertrophy ) - hyperthyroidism, hypothyroidism - Hyperparathyroidism ( with high calcium serum level, PTH and vit. D 3 )

Causes of secondary hypertension whatever the age 4. Others: - coarctation of the aorta - Turner syndrome - obstructive sleep apnea ( OSA ) - multiple neuritis - neurofibromatosis ( NF ) - drug-induced hypertension - and many more…

Most common causes of hypertension by age Newborns: - renal artery or venous thrombosis - renal artery stenosis - congenital renal abnormalities (e. g. congenital renal dysplasia ) - coarctation of the aorta - bronchopulmonary dysplasia

Most common causes of hypertension by age First year: - coarctation of the aorta - renovascular diseases - renal parenchymal disease - iatrogenic ( medication, volume overload ) - tumour

Most common causes of hypertension by age Infancy to 6 year: - renal parenchymal diseases secondary to reflux nephropathy, obstructive uropathy, chronic renal infections ( pyelonephritis! ) and nephrotic syndrome, HUS, glomerulonephritis, polycystic kidney disease - renovascular disease ( stenosis of renal artery ) - coarctation of the aorta - endocrine causes ( hyperthyroidism, hypercalcemia, mineralocorticoids excess) - iatrogenic

Most common causes of hypertension by age 6 -10 yrs: - renovascular diseases ( stenosis of renal artery ) - essential/idiopathic/primary hypertension - renal parenchymal disease - thyroid diseases - pheochromocytoma - neurofibromatosis

Most common causes of hypertension by age Over 10 yrs: - primary hypertension!!! - renal parenchymal diseases - and others
 2. Assessment")
Diagnostic evaluation 1. Finding the cause of hypertension ( medical history ) 2. Assessment of organ changes and risk factors ( medical history and physical examination )
 - lifestyle factors")
Medical history - family history of hypertension ( primary hypertension ) - lifestyle factors ( diet, sport, salt intake ) - cardiovascular risk factors ( in patients and in their families like eg. premature atherosclerosis, cardiovascular disease ) - concomitant diseases that could affect prognosis and guide treatment ( especially diabetes ) - medications - renal diseases ( in patients and their families ) - substance abuse
 –")
Physical examination 1. Inspection: - skin: cafe au lait stains ( marks ) – NF - exophthalmia, goiter – hyperthyroidism - bisexual organs, gynekomastia, the lack of secondary sexual features in girls, hirsutism – failure of biosynthesis of adrenal cortex hormones ( eg CAH ) - hypertrophy of the tonsils – disorders of night respiratory

Examination - continued 2. Palpable exam: - big, pulsing fontanel – hydrocephalus - goiter – hyperthyroidism - Abnormal abdominal masses – Wilm’s tumor, hydronephrosis, polycystic kidney disease 3. Auscultation: - Systolic murmur above aorta and between blade bones – coarctation of the aorta - systo-diastolic murmur in abdominal and/or lumbar area – reno-vascular hypertension

Examination - continued 4. Neurological exam: - Chwostek and Trousseau syndrome, weakened tendinous reflex – hyperaldosteronism ( low Ca, K, high Na ) 5. Pulses examination: - decreased – possibility of intracranial hypertension - increased – hyperthyroidism - normal in the upper limbs and poor or none in the lower limbs – coarctation of the aorta
 and WHR (")
Physical examination - calculation of BMI ( body mass index ) and WHR ( waist-hip ratio ) - ophthalmogical examination - fundus of the eye
")
Diagnostic tests 1. Serum tests: -creatinine, BUN, ionogram ( sodium, kalium and calcium ) -lipidogram -renine serum activity with sodium and aldosterone urine elimination 2. Urine analysis

Lab test - continued 3. 24 -hour urine collection of : - microalbumines ( to assess glomerulus damage ) - VMA ( vaniline-mandelic acid ), catecholamines to exclude pheochromocytoma/neuroblastoma ( an excess release of catecholamines to the blood system ) - 17 -KS, 17 -OHCS - markers of adrenal cortex ( to assess aderenal cortex abnormality like e. g. Cushing syndrome ), - steroid profile ( to exclude steroidogenesis abnormalities)
 - TSH, T 3")
Lab test continued - cortisol profile ( Cushing syndrome ) - TSH, T 3 and T 4 ( thyroid abnormalities ) - OGTT in every obese child with BMI over the 85 percentile !!! - drug screen – when substance abuse is suspected
 is susspected when there is hypertension with: -")
Primary hyperaldosteronism ( Conn syndrome ) is susspected when there is hypertension with: - Hypokaliemia ( <3, 5 m. Eg/l ) - Increased kalium urine eliminations is confirmed when: - Aldosteron activity in urine and blood is high - Renine Serum Activity is low.

Primary hyperaldosteronism continued • Primary hyperaldosteronism – Conn syndrome can be caused by: - hypertrophy, - adenoma, - carcinoma of adrenal cortex

Primary hyperaldosteronism continued Symptoms: - polidypsia, poliuria, weakness of the muscles, cramps ( follow from hypokaliemia) - Hypertension ( retension of sodium ) Diagnosis: - scyntygraphy with scintadren Treatment: - Spironolacton ( blocker of mineralocorticoids receptors ) - Triamteren, Amilorid – diuretics-severs of kalium - Ace-inhibitors; rarely Ca-blockers

Hypertension with hyperkaliemia • Very rare diagnosis of e. g. monogenic Gordon’s syndrome or it can occure in polycystic kidney disease.

Additional tests - Abdominal US with renal assessment and renal doppler ( the assessment of renal arteries ) This test should be done in every patient before initiation of ACE-inhibitor treatment!!! Bilateral renal artery stenosis is contraindication for ACE inhibitors !!!

Additional tests continued - Renoscyntygraphy ( sometimes with captopril test when renovascular hypertension is suspected ) - Miction cystoureterography especially in young children with history of urinary tract infections or kidney scars occurring in renoscyntygraphy. - Echo with assessment of the left ventricular mass and aortic arch. - Angio. CT, renal arteriography and angio. MR of renal arteries are done when the diseases of renal vessels are suspected. - Scyntygraphy with MIBG ( when pheochromocytoma is suspected ) or with scintadren ( when adrenal cortex tumour is suspected )

Complications of hypertension Refers to: - The heart - Vessels - The Brain - Kidneys
 - acute")
Complications continued • Heart: - left ventricular hypertrophy ( IVS hypertrophy ) - acute heart failure - systolic heart failure - chronic heart failure - myocardial ischemia

Complications - continued • Vessels: - increase of peripheral resistance - remodeling of vessels, - atherosclerosis - thrombo-embolic incidents

Complications - continued Brain: - acute hypertensive encephalopaty and oedema of the brain - TIA ( transient ischemical attacks ) - ischemic and/or haemorrhagic brain strokes

Complications - continued Kidney: - hyperfiltration - proteinuria - parenchymal kidney hypertension which leads to polyuria and metabolic alkalosis - vascular sclerosis - increase of uric acid - chronic kidney disease

Assessment of hypertension complications - echo: assessment of the left ventricular mass - ophtamologic examination: assessment of the fundus of the eye ( vessels )-hypertensive retinopathy - assessment of the kidney’s function: BUN, creatinine, GFR, microalbuminuria ( damage of glomerulus vessels and hyperfiltration ) - US doppler: assessment of the thickness of arteries

Assessment of hypertension complications Remember ! The assessment of hypertensive complications and the risk of cardiovascular changes is the main criteria of initiation of the pharmacological treatment.

Management algorythm of primary hypertension 1. Measure BP and height and calculate BMI A - normotensive – educate on healthy lifestyle B - prehypertensive : - therapeutic lifestyle changes ( diet, sport etc ) - repeat BP in 6 months - consider diagnosis workup and evaluation for organ damage - if overweight exists – weight reduction - if no overweight – monitor BP every 6 months

Management algorithm continued C - stage 1 hypertension - repeat BP over 3 visits – assess organ damages: - if primary hypertension - therapeutic lifestyle changes - weight reduction - if secondary hypertension - specific diagnostic for the cause

Management algorithm continued D - stage 2 hypertension - diagnosis procedure include assessment of organ changes - consider referral to provider with expertise in pediatric hypertension: - if normal BMI- drug treatment - if overweight – weight reduction and drug treatment

Hypertension- treatment At the begining, in every child with hypertension or RR high normal- non farmacological treatment is recomanded!

Treatment When hypotensive treatment is necessary: 1. In conditions with temporary hypertension 2. In secondary hypertension with ineffective or impossible causal treatment 3. In primary hypertension when ineffective nonpharmacological treatment Goal of treatment - Blood pressure level less than the 95 th percentile! In case of coincidence of diabetes and renal diseases – less than the 90 th percentile.

Treatment There are two methods of treatment: - non-pharmacological - pharmacological Non-pharmacological treatment has particular meaning in primary hypertension and it is based on changing lifestyle: -loss of weight -physical activity -modification of a diet ( including limiting of salt intake ) There is only one contraindication of practice sport – bad controlled stage 2 hypertension!!

vs.

When to start pharmacological treatment in primary hypertension 1. In primary hypertension after 6 months ineffective non-pharmacological treatment ( stage 1 ) 2. In stage 2 primary hypertension ( always ) 1. In primary hypertension stage 1 with complications ( eg IVS hypertrophy, changes on the fundus of the eye ) or/and concomitant diseases like diabetes , hyperlipidemia 4. In prehypertensive patients with complications and risk factors like diabetes ( also )

Treatment - continued Pharmacological: In children we use almost every kind of hypotensive drugs, but ACE-inhibitors and Ca-blockers are the drugs from the choice!!! We start treating from monotherapy. In case of severe and symptomatological hypertension polytherapy is recommended ( including i. v. intake either )
 -Lizynopril ( Lisinoratio )")
Hypotensive drugs using in pediatrics ACE-inhibitors: -Enalapril ( Enarenal ) -Lizynopril ( Lisinoratio ) -Ramipril ( Polpril, Ramicor ) -Captopril s. l. Mechanism of ACE-inhibitors activity: - Inhibition of RAAS ( with dicrease aldosterone and increase sodium and dicrease kalium elimination ) Ace inhibitor are contraindicated in biltateral stenosis of renal artery!!!
 -Valsartan ( Valzek )")
Hypotensive drugs continued AT 1 blockers: -Lozartan ( Lorista ) -Valsartan ( Valzek ) Alfa and beta blockers: -Labetalol Beta blockers: -Atenolol -Metoprolol ( Metocard, Beatloc ZOK ) -Propranolol
 Diuretics: -Hydrochlorothiazidum -Furosemid -Spironolactone")
Hypotensive drugs continued Ca-blockers: -Amlodipine ( Amlozek ) Diuretics: -Hydrochlorothiazidum -Furosemid -Spironolactone
: -Klonidine ( central")
Hypotensive drugs continued And also ( rare using in pediatrics ): -Klonidine ( central alfa-agonist ) -Alfa-blockers: Doksazosyna, prazosyna -Wasodilatators: Hydralazine, Minoksydil -Metyldopa

Treatment in urgency and emergency hypertension • Hypertensive urgency ( the risk of organ failure ): The normalization of the blood pressure in 36 -96 hrs is needed Hypertension emergency ( impending organ failures ) The normalization of the blood pressure in 48 -72 hrs is needed

Hypertensive urgency-treatment First 6 hrs – decrease of the blood pressure for about 30% Next 36 -96 hrs – gradually normalization of the blood pressure

Hypertensive emergency • Firs 1 -2 hrs – decreasment the bllod pressure for about 30% • Next 24 -36 hrs – decresement the blood pressure for another 30% • Then normallization of the pressure till 7296 hrs

Hypotensive drugs using in urgency and emergency stages • • Nifedypina – s. l. Labetalol – i. v. Sodium Nitroprusyde- i. v Diazoksyd – i. v. Hydralazyna – i. v. Klonidyna – i. v. Esmolol – i. v.

Treatment of severe hypertensioncontinued It must be done in the intensive care unit, with ecg-monitoring, RR-monitoring, pulsoxymetre monitoring, water balance and intarvenious access Monitoring blood pressure in every 15 min until it’s decreased for 30% Later in every 30 -60 min In every patient the fundus of the eye and neurological state should be assessed.

Healthy lifestyle = no primary hypertension Thanks for your attention

What you should know after presentation 1. 2. 3. 4. 5. Definition of hypertension and its stages What is „white-coat” hypertension When to start checking bp and how often Main rules of measurement of bp in children Most common causes of secondary hypertension by age ( newborns, infants and teenagers ) 6. Which tests ( blood, urine, additional ) are necessary to diagnose hypertension and its complications 7. When to start pharmacological treatment and goals of treatment 8. Which medications are from the choice in pediatrics and what is the contraindications of ACE-inhibitors. 9. Non-pharmacological methods of hypotensive treatment 10. What is primary hyperaldosteronism (serum markers)
- Slides: 77