HYPERTENSION HYPERTENSION o The commonest cardiovascular disorder o


 < 120 or DBP (mm Hg)")


 Observer error. Hearing acuity Interpretation of")



 – •")







 POPULATION STRATEGY Directed at whole of population irrespective of individual risk levels Goal")
 POPULATION STRATEGY 1. Nutrition Salt intake Less than 2. 4 gm sodium or")
 Developed by the National Heart, Lung & Blood")
 POPULATION STRATEGY 2. 3. Weight reduction : BMI< 25 kg/m 2 Exercise promotion")
 HIGH RISK STRATEGY Directed towards people at-risk of having hypertension Aim- to prevent")




- Slides: 28
HYPERTENSION
HYPERTENSION o The commonest cardio-vascular disorder o Major public health challenge to population in socio- economic and epidemiological transition o Major risk factor for cardiovascular mortality
BLOOD PRESSURE CLASSIFICATION Category Normal SBP (mm Hg) < 120 or DBP (mm Hg) < 80 Prehypertension 120– 139 or 80– 89 Stage 1 hypertension 140– 159 or 90– 99 Stage 2 hypertension > 160 or > 100 In case of different categories of SBP and DBP— Higher category should be selected to classify the individual’s blood pressure.
CONSEQUENCE S OF HYPERTENSION ORGAN DAMAGE Although extent of organ damage often correlates with level of blood pressure, it may not always be the case. Blood pressure and organ damage should be evaluated separately. The presence of signs of organ damage confers higher CV risk to any level of blood pressure.
BLOOD PRESSURE MEASUREMENT Preferably in sitting position An appropriately sized cuff (cuff bladder encircling at least 80 percent of the arm) should be used. At least two measurements should be made and the average recorded. The cuff deflation rate for auscultatory readings should be 2 mm. Hg per second. SBP is the point at which the Korotkoff sounds is first heard (onset of phase 1), and the disappearance of Korotkoff sound (onset of phase 5) is used to define DBP.
SOURCES OF ERROR IN BLOOD PRESSURE MEASUREMENT a) Observer error. Hearing acuity Interpretation of Korotkoff’s sound b) Instrumental error. Leaking valve Inappropriate cuffs c) Subject error Circumstances of examination like physical environment, position of subject, external stimuli like fear, anxiety etc.
CLASSIFICATION Primary HTN Essential HTN o Elevated BP without an identified cause o 90% to 95% of all cases o Secondary HTN Elevated BP with a specific cause 5% to 10% of adult cases Causes Renal disorder Drug induced Endocrinal disorders Coarctation of aorta
CAUSES OF SECONDARY HYPERTENSION Chronic kidney disease Coarctation of the aorta Cushing’s syndrome and other glucocorticoid excess states including chronic steroid therapy Drug induced or drug related Obstructive uropathy Pheochromocytoma Primary aldosteronism and other mineralocorticoid excess states Renovascular hypertension Sleep apnea Thyroid or parathyroid disease
MAGNITUDE OF PROBLEM Raised BP causes 7. 5 million deaths – 12. 8% of total annual deaths Major risk factor for CVD- risk doubles for each incremental increase of 20/10 mm Hg of BP. Prevalence in adults aged 25 years and more was 40% in 2008.
Prevalence of hypertension in India According to ICMR survey (during 2007 -08) – • Prevalence ranges from 17 -21 % in all states • with marginal urban-rural differences
“RULE OF HALVES” Hypertension is an “iceberg disease” 1. 2. 3. Community • 1. Normotensive • 2. Hypertensives • 3. Undiagnosed • 4. Diagnosed 4. Diagnosed 5. 6. 7. 8. Treated • 5. Untreated • 6. Treated • 7. Inadequately treated • 8. Adequately treated
“TRACKING” OF BLOOD PRESSURE The phenomenon of persistence of rank order of blood pressure on follow up over a period of years from early childhood to adulthood. Helps in identifying children and adolescents “at risk” of developing HTN at a future date.
RISK FACTORS FOR HYPERTENSION Non-modifiable Age – Increases with age Sex – M>F in young and middle age, more risk in menopausal females Genetic factors 45% higher risk in children with two hypertensive parents Ethnicity Higher in black communities Modifiable Obesity Salt intake Saturated fat Dietary fibre Alcohol Stress Physical activity Socio-economic status
MODIFIABLE RISK FACTORS OBESITY Increases volume of blood Increases pressure/resistance that heart has to pump against---enlarged heart muscle “central obesity” is more positively correlated. INACTIVITY Heart is not used to “work” = heart beats harder/faster = more force on arteries = uses more oxygen per beat = higher heart rate at rest Physical activity – indirectly reduces BP by reducing body weight
MODIFIABLE RISK FACTORS Tobacco use Can lead to damage of artery wall, increases heart rate, encourages narrowing of arteries Stress Causes unpredictable blood pressure and pulse increases along with potential inflammation in the vessel walls.
MODIFIABLE RISK FACTORS Sodium intake Leads to more fluid/water in the vessels = increased blood pressure Low potassium intake Potassium helps balance sodium in cells and control heart rhythm Excessive Long alcohol term: damages liver and pressure within our circulation and heart.
PREVENTION OF HYPERTENSION 1. Primary prevention – all measures to reduce the incidence of hypertension in a population by reducing the risk of onset. Population strategy b) High-risk strategy a) 2. Secondary prevention
A) POPULATION STRATEGY Directed at whole of population irrespective of individual risk levels Goal -to shift the community distribution of BP towards lower levels or “biological normality” Involves multi-factorial approach Nutrition Weight reduction Exercise promotion Behavioral changes Health education
A) POPULATION STRATEGY 1. Nutrition Salt intake Less than 2. 4 gm sodium or 6 gm Na. Cl Moderate Restrict 2 fat intake alcohol intake drinks /day for men 1 drink/day for women
DASH (DIETARY APPROACHES TO STOP HYPERTENSION) Developed by the National Heart, Lung & Blood Institute Eating Low plan that is… in saturated fat Low in cholesterol Low in total fat Emphasizes Fruits Vegetables Low fat and fat free milk Potassium, calcium and magnesium
A) POPULATION STRATEGY 2. 3. Weight reduction : BMI< 25 kg/m 2 Exercise promotion : 4. ≥ 150 min/week of moderate physical activity (30 min per day for at least 5 day a week) Behavioral change stress reduction smoking cessation 5. 6. Health education Self care
B) HIGH RISK STRATEGY Directed towards people at-risk of having hypertension Aim- to prevent attainment of levels of blood pressure at which institution of treatment would be considered This approach is appropriate if risk factors occur with very low prevalence in community Since “clustering” of hypertension occurs in family, individuals at risk can be identified with family history of hypertension tracking of blood pressure from childhood
SECONDARY PREVENTION i. ii. Goal- to detect and control high BP in affected individuals Early case detection: by screening (as HTN is a silent disease) Treatment iii. Only control is possible To prevent complication Other risk factors (smoking, high cholesterol levels) are also addressed Patient compliance Ensured through education directed to patients, families and the community
Antihypertensive drugs Diuretics Beta-Blockers Ace inhibitors Calcium channel blockers Angiotensin II Receptor Blockers Goal of BP <140/90 mm. Hg, <130/80 mm. Hg for patients with diabetes and chronic kidney disease
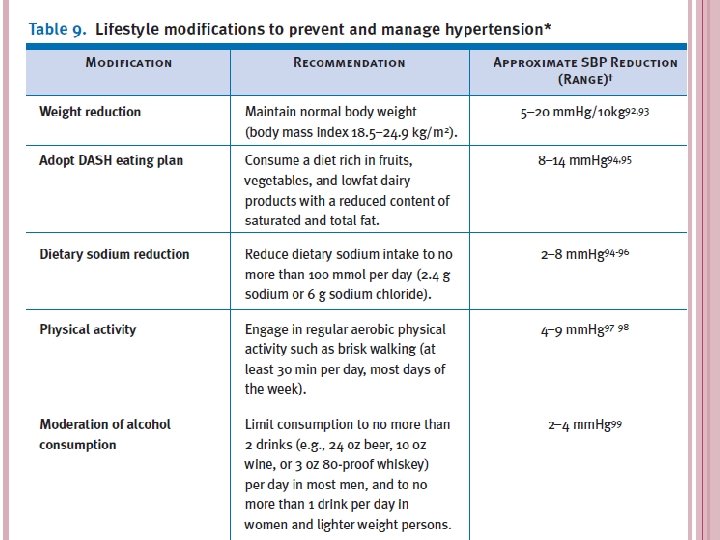
LIFESTYLE MODIFICATIONS ‘Lifestyle’- first coined by Austrian psychologist Alfred Adler in 1929 - which means the way a person lives. Essential for both primary and secondary prevention reduce BP, prevent or delay the incidence of hypertension, enhance antihypertensive drug efficacy, and decrease cardiovascular risk.
THANK YOU!