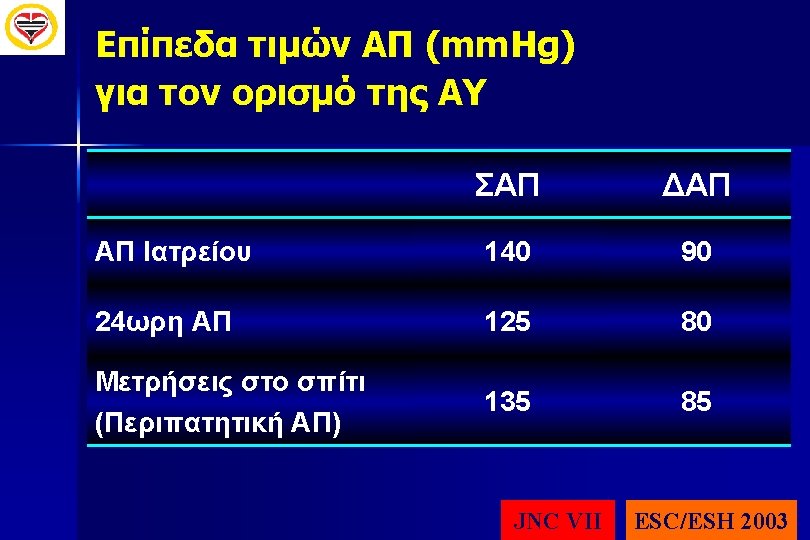
Borderline hypertension Hypertension only on first visits Hypertension


Borderline hypertension ΥΠΕΡΤΑΣΗ Hypertension only on first visits Hypertension at work Spurius Hypertension Nocturnal hypertension White Coat Hypertension Masked Hypertension ΦΥΣΙΟΛΟΓΙΚΗ ΑΠ Labile hypertension

MASKED HYPERTENSION SHEAF Study Bobrie G, et al. JAMA 2004; 291: 1342 -9 2, 5 1. 3 -3. 0 Hazard ratio P=0. 001 2, 0 1. 96 1. 2 -3. 5 P=0. 001 2. 06 0. 7 -2. 1 1, 5 P=0. 66 1 1, 0 Normotension 1. 18 White Coat Hypertension Masked Hypertension
-β(DBP) Ages 20 -79 years (5")
H ΣΑΠ είναι πιο σημαντικός παράγοντας καρδιαγγειακού κινδύνου β(SBP)-β(DBP) Ages 20 -79 years (5 groups: < 40, 40 -49, 50 -59, 60 -69, 70 -79) AGE (Years) Adjusted for age, sex and other risk factors Franklin SS et al. Circulation 2001; 103: 1245 -1249


ΣΡΑΑ, Υπέρταση και καρδιαγγειακός κίνδυνος. . . the RAAS appears to be the root of most evil D. G. Beevers, November 2003 Lip GYH, More evidence of blocking the renin-angiotensin-aldosterone system in cardiovascular disease and the long-term treatment of hypertension: data from recent clinical trials (CHARM, EUROPA, Val-HEFT, HOPE-TOO and EUR 2) J Hum Hypertens 2003; 17: 747 -750
 · · Vasoconstriction Cell growth")
Renin-Angiotensin Aldosterone System Non-ACE Pathways (e. g. , chymase) · · Vasoconstriction Cell growth Na/H 2 O retention Sympathetic activation Angiotensinogen renin AT 1 Angiotensin II ACE Aldosterone Cough, Angioedema Benefits? Bradykinin Inactive Fragments AT 2 · Vasodilation · Antiproliferation (kinins)

![Διάγνωση νεφρικής βλάβης στον υπερτασικό ασθενή n Formula Cockcroft-Gault [140 -age (yrs)] Χ [](http://slidetodoc.com/presentation_image_h/15d4449ee6fd9d4fa828639931bd3ddf/image-33.jpg "Διάγνωση νεφρικής βλάβης στον υπερτασικό ασθενή n Formula Cockcroft-Gault [140 -age (yrs)] Χ [")
Διάγνωση νεφρικής βλάβης στον υπερτασικό ασθενή n Formula Cockcroft-Gault [140 -age (yrs)] Χ [ 72 ή 85 [Weight (Kg)] ] Χ [S-Cr (mg%)] 22 ετών άνδρας 120 Kg 121 S-Cr= 1. 6 mg/d. L GFR= 123 ml/min 85 ετών γυναίκα 46 kg S-Cr= 1. 6 mg/d. L GFR=18. 6 ml/min

Progression of nephropathy in type 2 diabetes Incidence of macroalbuminuria 40 30 30 20 Incidence of ESRD (placebo) 30 20 20 10 10 10 0 0 3 6 (placebo) 40 (%) (%) Incidence of microalbuminuria 0 1 2 3 4 Time (years) Gall M-A, et al. BMJ 1997; 314: 783 -8. Parving H-H, et al. N Engl J Med 2001; 345: 870 -8. Brenner BM, et al. N Engl J Med 2001; 345: 861 -9. Normoalbuminuria UAE (µg/min) <20 Microalbuminuria 20 -199 Macroalbuminuria ESRD _ 200 > ADA. Diabetes Care 2004; 27(Suppl. 1): S 79 -S 83.

Γιατί είναι κλινικά χρήσιμη η Μικροαλβουμινουρία? mg/day CV Risk and Presence of Renal Dysfunction and Vascular Dysfunction CV Risk and Vascular Dysfunction Normal Microalbuminuria Albuminuria (Proteinuria)

Antihypertensive Treatments and Incidence of New Onset Diabetes % Higher Incidence in Patients Using Diuretics, b-Blockers Study CAPPP diuretics, b-blockers 13% vs. captopril CHARM placebo ± SOC 16% vs. candesartan ± SOC INVEST atenolol ± HCTZ or trandolapril 17% vs. verapamil ± HCTZ or trandolapril INSIGHT co-amiloride ± b-blocker 30% vs. nifedipine GITS LIFE atenolol 33% vs. losartan ALLHAT chlorthalidone 18% 43% vs. amlodipine vs. lisinopril HOPE placebo ± SOC 50% vs. ramipril ± SOC ALPINE HCTZ ± atenolol 720% vs. candesartan ± felodipine Lancet 1999; 353: 611 -16. Lancet 2003; 362: 759 -66. JAMA 2003; 290: 2805 -2816. Lancet 2000; 356: 366 -72. Lancet 2002; 359: 995 -1003. JAMA 2002; 288: 2981 -97. N Engl J Med 2000; 342: 145 -53. J Hypertension 2003; 21: 1563 -1574.

100 No Diabetes 90 80 4. 70 3. 90 A 5 4 p<0. 0001 70 3 Previously Known Diabetes C 60 50 New-Onset Diabetes 40 2 0. 97 1 B 0 30 0 3 6 9 Time to Event (years) 12 15 A Rate of Events (per 100 patient-years) Probability of Event-Free Survival (%) CV Events in Treated Hypertensives without DM, with New-Onset DM & Previously Known DM B C Groups Verdeccia et al 2004

β-Blockers: To use or not to use? DM “Lone” Hypertension + BB Use 0% CAD Sympathetic activity Congestive heart failure 100% Messerli FH, et al. In: Griffin BP, Topol EJ, eds. Manual of Cardiovascular Medicine 2 nd Ed. Cleveland. Ohio: Cleveland Clinic Foundation, 2004.

BP Reductions as Little as 2 mm Hg Reduce the Risk of CV Events by Up to 10% • Meta-analysis of 61 prospective, observational studies • 1 million adults • 12. 7 million person-years 2 mm Hg decrease in mean SBP 7% reduction in risk of ischemic heart disease mortality 10% reduction in risk of stroke mortality Lewington S et al. Lancet 2002; 360: 1903 -1913.
 and Reinforcements (+) • No CCB")
New Guidelines on Hypertension – Possible Changes (Δ) and Reinforcements (+) • No CCB in CAD patients • No CCB for CHD/CHF function • ARB and CHD • ARB and stroke prevention • Metabolic variables and choice of T • BP control (<140/90 mm. Hg) • BP threshold/target (high risk) • Combination T also as 1 st choice • Consistency of BP control • Control of out-of-office BP Δ? + Guidelines + Δ? • Total CV risk in screening/FU • TOD assessment in screening/FU • Emerging risk factors/TODs? Metabolic Syndrome New Onset Diabetes/Prediabetes Lipid variables • D as min 1 st choice • BB as 1 st choice • D/BB combination as priorital • ACEI/ARB combination as last priorital
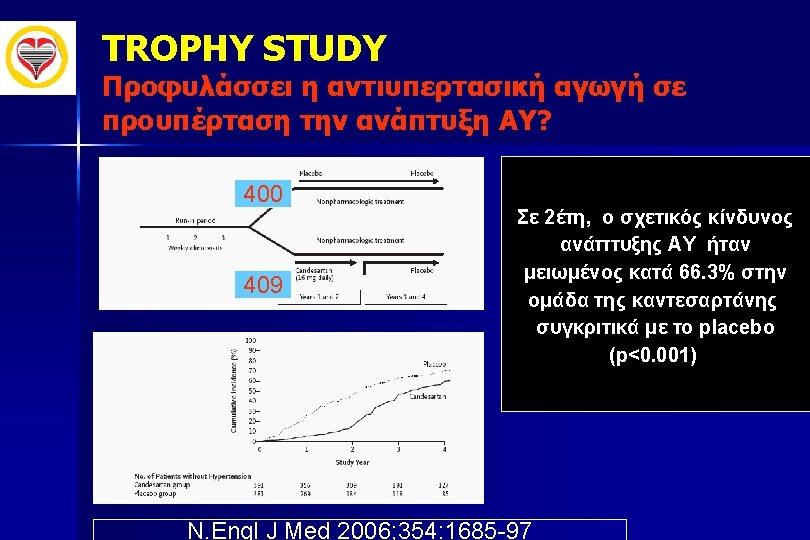
- Slides: 54