Hypertension The silent killer Difinition High blood pressure

Hypertension The silent killer

Difinition • High blood pressure is defined as BP ≥ 140/90 millimeters of mercury (mm. Hg) as per JNC 8

Risk of hypertension • Hypertension is a major independent risk factor for coronary artery disease, stroke, heart failure, and renal failure

Etiology • For the majority of patients with high blood pressure, the cause is unknown. This is classified as primary or essential HTN. Over 90% of patients with high blood pressure have primary HTN. Primary HTN cannot be cured, but it can be controlled with appropriate therapy (including lifestyle modifications and medications). Genetic factors may play an important role in the development of primary HTN.

Secondary hypertension • A small portion of patients have a specific cause of their high blood pressure, which is classified as secondary HTN. Less than 10% of patients with high blood pressure have secondary HTN. • Secondary HTN is caused by an underlying medical condition or medication Controlling the underlying medical condition or removing the causative medication(s) will result in a decrease of blood pressure thereby resolving secondary HTN. • The most common cause of secondary HTN is associated with kidney impairment such as chronic kidney disease (CKD)

White-Coat Hypertension • White-coat hypertension refers to patients without target-organ disease who have consistently elevated BP values measured in a clinical environment (e. g. physician's office) that are significantly higher than those obtained by either a manual reading outside this environment (e. g. , home) or with 24 -hour ambulatory monitoring.

Symptom of hypertension • HTN is known as the “silent killer” because it typically has no warning signs or symptoms, and many people do not know they have it. Even when blood pressure levels are dangerously high, most people do not have any signs or symptoms. • A small amount of people may experience symptoms such as dull headaches, vomiting, dizzy spells, and more frequent nosebleeds. • These symptoms usually do not occur until blood pressure levels have reached a severe or life-threatening stage

Classification of hypertension

Recommended Technique for Auscultatory BP Measurement in Adults. • Patient should be seated for 5 minutes with arm bared, unrestricted by clothing, and supported at heart level. Smoking or food ingestion should not have occurred within 30 minutes before the measurement. • An appropriately sized cuff should be chosen. The internal inflatable bladder width should be at least 40% and the bladder length at least 80% of the upper arm circumference. • The cuff should be wrapped snugly around the arm with the center of the bladder over the brachial artery.

• Measurements should be taken with a mercury sphygmomanometer, a recently calibrated aneroid manometer, or a validated electronic device. • �The palpatory method should be used to estimate SBP. The cuff is inflated while simultaneously palpating the radial pulse on the cuffed arm and observing the manometer. The point at which the radial pulse is no longer palpable is the estimated SBP. The cuff is then deflated.

• The BP should be measured with a stethoscope positioned over the brachial artery and the cuff rapidly inflated to 20 to 30 mm Hg above the estimated SBP from the palpatory method. The cuff is deflated at a rate of 2 mm Hg per second while listening for Phase 1 (the first appearance of sounds) and Phase 5 (the disappearance of sounds) Korotkoff sounds and observing the manometer. • When 10 to 20 mm Hg below Phase 5, the cuff can be rapidly deflated.
 and Phase 5")
• The BP should be recorded. The Phase 1 (SBP) and Phase 5 (DBP) value should be recorded in even numbers (rounded up form an odd number) along with the patient's position, arm used, and cuff size documented. • �A second measurement should be taken after 1 to 2 minutes in the same arm. If the readings differ by more than 5 mm Hg, additional measurements should be obtained. The mean of these two values should be used to make clinical decisions. • BP should be taken in both arms at the initial visit with the BP taken in the arm with the higher reading at subsequent visits.

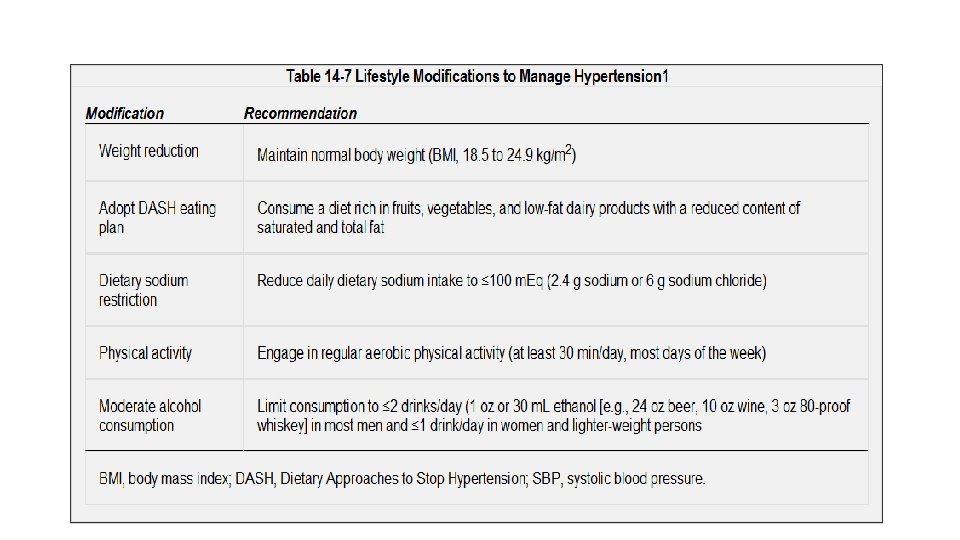
Principle of treatment • Principles of Treatment • Treatment for hypertensive patients includes both nonpharmacologic (lifestyle changes) and pharmacologic (medication) therapy to lower blood pressure and prevent cardiovascular (heart) events such as a heart attack. • DASH Diet • DASH (Dietary Approaches to Stop Hypertension) diet is rich in fruits, vegetables, and low-fat dairy foods, coupled with reduced saturated and total fat. This diet can substantially reduce BP (8 to 14 mm Hg in SBP for most patients) The low-fat component of this diet is important as weight loss is more readily achieved by a low-fat diet and it also reduces the risk of CVD by improving cholesterol.

Treatment option

Treatment goal
- Slides: 16