Agents to Treat Hypertension What is Hypertension A



 Diastolic (mm Hg)")











 Centrally acting: - Clonidine, Methyl dopa b) Ganglionic blocking agents; -")
 Mixed α and β adrenergic blockers: - Labetolol, Carvediol. Diuretics : -")


 inhibitors Alpha blockers Alpha-2 -agonists")
 Inhibitor")


; Hydrochlorothizide (Hydro. DIURIL) Beta blockers Atenolol")

 Betaxolol (Kerlone) Bisoprolol (Zabeta)")









 u. Used in the treatment")
 Phenyliminoimidazolidine derivative Antihypertensive effect followed by long lasting hypotensive")
 Methyldopa (Aldomet) Guanabenz (")
-4, 5 -dihydro-1 H-imidazol-2 amine CLONIDINE R=H 4 -HYDROXYCLONIDINE R=OH")

![Guanethidine(Ismelin) [2 - (hexahydro-1 H-azocinyl)ethyl]guanidine Guanidine act by interfering with adrenergic transmission. Attached to](https://slidetodoc.com/presentation_image/47e8eacf04c2a6f8ac7504f8f6effdd7/image-41.jpg "Guanethidine(Ismelin) [2 - (hexahydro-1 H-azocinyl)ethyl]guanidine Guanidine act by interfering with adrenergic transmission. Attached to")







; 2, 4 -diamino-6 piperidinopyramidine-3 oxide.")





![O C (CH 2)n----- [Zn binding grp] NRin g](https://slidetodoc.com/presentation_image/47e8eacf04c2a6f8ac7504f8f6effdd7/image-55.jpg "O C (CH 2)n----- [Zn binding grp] NRin g")



 Angiotensin-II - Vasoconstriction")






![ACE-Inhibitors [1]](https://slidetodoc.com/presentation_image/47e8eacf04c2a6f8ac7504f8f6effdd7/image-67.jpg "ACE-Inhibitors [1]")











- Slides: 78
Agents to Treat Hypertension:
What is Hypertension? A serious disease affecting 1 in 3 adults in the United States More commonly known as High Blood Pressure Occurs when blood is forced through the heart and arteries under excessive pressure
What is Blood Pressure? Blood pressure readings have two components: Systolic pressure Heart muscles contracted Diastolic pressure Heart muscles relaxed With hypertension: Arteries narrow thereby increasing blood pressure Fluid volume in arteries increases which can increase pressure
Classifying Blood Pressure by Readings Blood Pressure Category Systolic (mm Hg) Diastolic (mm Hg) Normal <120 <80 Prehypertension 120 -139 80 -89 High: Stage 1 140 -159 90 -99 High: Stage 2 160 + 100 + High Blood Pressure = Elevated systolic pressure and/or elevated diastolic pressure. The highest reading dictates classification. Elevated readings must occur on multiple occasions to be diagnosed.
Classifying Hypertension by Causes Primary or Essential Hypertension Causes are unknown, but linked to risk factors, etiology is unknown. Secondary Hypertension 5 -10% of hypertension cases Caused by disease states
Some causes include: kidney disease, atherosclerosis, hormone imbalances, pregnancy, and some medications, renal, endocrinal or vascular disorder.
Who is Affected by Hypertension? Affects 1 billion people worldwide Affects 40 million Americans (15%) 30% of people with hypertension don’t know they have it Race and Gender Prevalence White Female 19. 3% White Male 24. 4% African-American Female 34. 2% African-American Male 35. 0% Hispanic Female 22. 0% Hispanic Male 25. 2% Race and Gender Death Rate White Males 14. 4% African-American Males 49. 6% White Females 13. 7% African-American Females 40. 5% (Death rates per 100, 000 people)
Why Should I Care? Hypertension can elevate your risk for: Stroke Blood clots Bleeding Heart attacks Heart enlargement Heart failure Kidney failure Atherosclerosis
Treatment Options for Hypertension Prevention is the best treatment strategy The goal of treatment: Lower blood pressure to prevent associated complications Typically <140/90 mm. Hg
It is a syndrome affecting arterial blood vessels, caused largely by the accumulation of macrophage white blood cells and promoted by low-density lipoproteins (plasma proteins that carry cholesterol and triglycerides) without adequate removal of fats and cholesterol from the macrophages by functional high density lipoproteins (HDL), It is commonly referred to as a hardening or furring of the arteries. It is caused by the formation of multiple plaques within the arteries.
Treatment of HTN There are following steps in treating HTN 1. Lifestyle modification 2. First line treatment 3. Second line treatment 4. Third line treatment
Treatment Options for Hypertension Then first drugs used to produce symptamatic relief of hypertension were αadrenergic blocking agents. Limitations- duration of action too short. Side effects precluded long term therapy. Adrenergic drugs exert their effects by direct action on adrenergic receptors. α andβ receptors NE activates α receptors Epinephrine activates β receptors.
α receptors fall into two groups α 1 found in smooth muscles of iris, arteries, arterioles, veins. α 2 - mediate the inhibition of adrenergic neurotransmitter release. β adrenergic receptors 3 types β 1, β 2, β 3.
β 1 - found in myocardium, stimulation increases the force and rate of myocardial contraction. β 2 - found in bronchial and vascular smooth muscles, stimulation causes Smooth muscle dilation or relaxation. β 3 - on fat cells and their stimulation causes lipolysis
Symptathomimetic agents Drugs stimulate the adrenergic nerve, directly by mimicing the action of NE.
Classification: a) Centrally acting: - Clonidine, Methyl dopa b) Ganglionic blocking agents; - Pempidine, hexamethonium, Pentolinium c) Adrenergic neuron blockers: - Guanethidine, reserpine, bethanidine, bretylium. d) β- adrenergic blockers : -propanolol, atenolol. e) α- adrenergic blockers : - Phenoxybenzamine, phentolamine, indoramine.
F) Mixed α and β adrenergic blockers: - Labetolol, Carvediol. Diuretics : - Chlorthiazide. Vasodilaors: eg: hydralazine, minoxidil, diazoxide, Na nitroprusside. Calcium channel blockers; Verapamil, Nefidipine, Diltiazem, Beridil, Amlodipine. Drugs acting on renin- angiotensin aldosterone axis: a)Angiotensin converting enzyme inhibitors:
Sulfhydryl containing inhibitor: - captopril Dicarboxylate containing inhibitor: - enalapril, lisinopril, quinapril, ramipril, trandopril, spirap ril etc. Phosphonate containing inhibitor: fosinopril Angiotensin II receptor antagonist : - losartan, valsartan, candesartan, telmisartan etc.
First Line Treatment Continue with lifestyle modification Initial drug selection: Diuretic Beta-blocker If inadequate, continue to second line treatment
Available Drug Therapies Drug therapies available: ACE (angiotensin-converting enzyme) inhibitors Alpha blockers Alpha-2 -agonists Angiotensin II receptor blockers Beta blockers Calcium channel blockers Combined alpha and beta blockers Combined ACE inhibitors and diuretics Diuretics
Second Line Treatment Adding drugs from the following categories Angiotensin Converting Enzyme (ACE) Inhibitor Calcium Channel Blocker Angiotensin II Receptor Blocker (ARB) α- blocker, α- and β-blocker If inadequate, continue to third line treatment
Third Line Treatment Increase drug dose, or Substitute another drug, or Add a second drug from another class If inadequate, may need to do further studies Serious organ damage may be present
Drug Therapies Options for Individualizing Antihypertensive Drug Therapy If you have hypertension and the following: Then your doctor may prescribe one of the following: Diabetes mellitus ACE Inhibitors, ARBs, Diuretics, Beta Blockers, Calcium Channel Blockers Heart failure Diuretics, Beta Blockers, ACE Inhibitors, ARBs, spironolactone Heart attack Beta Blockers, ACE Inhibitors, spironolactone Isolated systolic hypertension (elevated systolic only) Diuretics, certain Long-acting Calcium Channel Blockers Kidney Disease ACE Inhibitors, ARBs Recurrent Stroke Prevention Diuretics, ACE Inhibitors
Drugs Used to Treat HTN Diuretics Furosemide (Lasix); Hydrochlorothizide (Hydro. DIURIL) Beta blockers Atenolol (Tenormin); Propranolol (Inderal) ACE inhibitors Captopril (Capoten); Enalapril (Vasotec) ARB’s Irbesartan (Avapro); Losartan (Cozaar) Calcium channel blockers Amlodipine (Norvasc); Diltiazem (Cardizem)
Site Of Action of Antihypertensive Drugs Action of Beta-Blockers Block vasoconstriction Decrease heart rate Decrease cardiac muscle contraction Tend to increase blood flow to the kidneys -> leading to a decrease in the release of renin
Classification of Beta Blockers β 1 receptors blockers Atenolol (Tenormin) Betaxolol (Kerlone) Bisoprolol (Zabeta) Metoprolol (Lopressor, Toprol-XL) β 1, β 2 receptor blockers Nadolol (Corgard) Propranolol (Inderal) β 1, β 2, α receptor blockers Labetolol (Normodyne, Trandate)
Commonalities: -One chiral center -Aromatic ring -Side alkyl chain -Secondary hydroxyl group -Amine
DRUG AFFECTING CATECHOLAMINE STORAGE AND RELEASE Reserpine is a prototypical drug affecting vesicle storage of NE in sympathetic neurons and neurons of the CNS. Also of epinephrine of the adrenal medulla. It also affect the storage of serotonin and dopamine in their respective neurons in the brain.
Agents that block adrenergic neurotransmitter synthesis and / or release. Reserpine, guanethidine, pargyline.
Mechanism of action: Interferes with the Mg 2+- and ATP-dependent uptake of biogenic amines, depleting NE, dopamine, and serotonin. Reserpine decreases both cardiac output and PVR.
Rawolfia is an indole alkaloid obtained from the root of Rawolfia serpentina. Other alkaloids possessing the same activity are deserpidine and rescinnamine.
Reserpine extremely binds tightly with the ATPdriven MOA transporter that transports NE and other biogenic amines from the cytoplasm to the storage vesicles. This binding leads to a blockade of the transporter.
NE transported into the storage vesicle is metabolized by mitochondrial MAO in the cytoplasm. There is a gradual loss of vesicle stored NE as it is used up by release resulting from sympathetic nerve activity.
Storage vesicles eventually become dysfunctional. The end result is depletion of NE in the sympathetic neuron.
CATECHOLAMINE DEPLETORS-RESERPINE
u. Slow onset of action u. Sustained effect (weeks) u. Used in the treatment of hypertension u. May precipitate depression u. Both orally and parenterally.
Selective α 2 AGONIST CLONIDINE(CATAPRESS) Phenyliminoimidazolidine derivative Antihypertensive effect followed by long lasting hypotensive effect. Stimulate α 2 receptors in brain. Decrease in peripheral resistance and B. P
Direct acting adrenergic receptor agonists: α 2 receptors Clonidine (Catapres) Methyldopa (Aldomet) Guanabenz ( Wytensinr R Guanfacine (Tenex) Tizanidine (Zanaflex)
Chemical name: N-(2, 6 -dichlorophenyl)-4, 5 -dihydro-1 H-imidazol-2 amine CLONIDINE R=H 4 -HYDROXYCLONIDINE R=OH Phenyl imino imidazoline derivtive that possess selective α 2 adrenergic receptor Antihypertensive agent.
v Phenyliminoimidazolidine v Selective a 2 receptor agonist v The basicity of the guanidine group (p. Ka = 13. 6) is decreased (to p. Ka = 8. 0) because of the attachment to the dichlorophenyl ring v Administration: Oral, parenteral, transdermal
Guanethidine(Ismelin) [2 - (hexahydro-1 H-azocinyl)ethyl]guanidine Guanidine act by interfering with adrenergic transmission. Attached to either an alicyclic or aromatic lipophilic ring
Uses: Hypertension, Vasodilation, increases venous capacitance. u. Possess guanidino moiety (p. Ka > 12) They are essentially completely protonated. Do not get into the CNS. u. Prevents NE release from sympathetic nerve terminals.
VASODILATORS Drugs that act directly on the vascular smooth muscle, decreases vascular resistance and arterial B. P. Hydralazine: Relax smooth muscle (SM) of arterioles (and sometimes veins).
Vasodilators Types of vasodilators Arteriodilators reduce afterload Venodilators reduce preload Mixed vasodilators
Moderate to severe hypertension. Used in conjugation with hypertension and β blocker 1 -hydrazino-pthalazine.
Therapeutic use: Hydralazine: Dilates arterioles but not veins. Effect does not last long when used alone(tachyphylaxis); but combination therapy can be very effective for even severe hypertension.
Best effect is achieved when used together with βblockers and loop diuretics.
USES: Mild to moderate hypertension. Topical use in baldness Adverse Effects: Due to vasodilatation: Reflex tachychardia, palpitation, may ↑ angina. Compensatory increase in fluid and electrolytes, edema (Better combine with β-blocker & diuretic)
Minoxidil (Loniten); 2, 4 -diamino-6 piperidinopyramidine-3 oxide.
Minoxidil: Opens K+ channels in SM by its active metabolite, minoxidil sulfate, and stabilizes membrane at its resting potential. Patients with renal failure and severe hypertension, who do not respond well to hydralazine, may be given minoxidil.
It isinactive and biotranformed in liver by sulfotransferase into Minoxidil sulfate N-SO-3 called K+channel opener.
Mechanism: Like diazoxide, opens K+ channels, relaxes smooth muscle of BV & Cause arterial & venous dilatation, PR, BP Intracellular Ca++, ses the excitability smooth muscles.
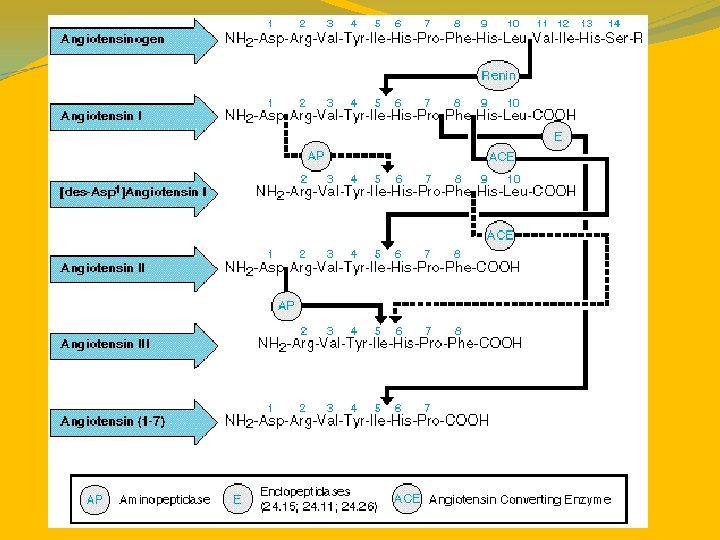
ACE-Inhibitors ACE is a zinc metalloproteinase It catalyses the hydrolysis of a dipeptide fragment, His-Leu, from a decapeptide, angiotensin ACE Angiotensin II Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu → Asp-Arg-Val-Tyr-Ile-His- Pro-Phe + His-Leu The reaction produces angiotensin II, an octapeptide
ACE is membrane-bound enzyme anchored to the cell membrane thru a single transmembrane domain located near the carboxy-terminal extremity. Zinc containing glycoprotein with a MW of 1, 30, 000. Nonspecific peptidyldipeptidrolase hydrolase widely distributed in mammalian tissues. It cleaves dipeptides from the carboxy terminus of a no of endogenous peptides. The impt binding points at the active site of ACE is a cationic site to attract a COO- ion and a zinc that can polarize a carbonyl grp of an amide function to hydrolysis
O C (CH 2)n----- [Zn binding grp] NRin g
Renin produced a potent vasopressor response when injected in a host. The angiotensin was used as a cofactor for renin to produce vasoconstriction. Identified as a decapeptide called angiotensin. Angiotensin existed in two forms--- biologically inactive decapeptide angiotensin I and the active decapeptide angiotensin II.
The precursor of angiotensin, angiotensinogen is a glycoprotein of molecular weight 58, 000 – 61, 000. 1. Renin, an aspartyl protease(MW 35, 000 -40, 000) cleaves Leu-Val bond from the aspartic acid end of the angiotensin polypeptide to release the decapeptide angiotensin I. 2. Cleavage of dipeptide(His-Leuminal) frm the carboxy terminal of angiotensin. I by ACE to form the octapeptide angiotensin. II , potent vasoconstrictor.
The N-terminal aspartate residue of angiotensin II is removed to form angiotensin III , a reaction catalyzed by glutamyl aminopeptidase. AIII has a less potent but significant regulatory effect on Na excretion by the renal tubules. Na and K balance and arterial B. P is modified by vasodilators called kinins. Callidin tissue enzymes Bradykinin PGrelease ACE Inactive pdts vasodilatation
Angiotensisn Inhibitors Angiotensin-I Angiotensin Receptor Blockers Bradykinin Angiotensin Converting Enzyme (ACE) Angiotensin-II - Vasoconstriction - Aldosterone BP ACE Inhibitors Inactived Vasodilatation BP 61
History Highlights: ACE-Inhibitors Discovered in 1960’s Venom of pit vipers intensified the response to bradykinin, a vasodilator Response was caused by peptides that inhibited kininase II, an enzyme that inactivated bradykinin Later found that kininase II = ACE (angiotensin-converting enzyme) http: //www. szgdocent. org/resource/rr/c-viper. htm First Drug- Teprotide Nonapeptide that lowered blood pressure caused by primary hypertension Not orally active
Carboxypeptidase is a zinc metalloproteinase that could be isolated Carboxypeptidase splits a terminal amino acid from a peptide chain In the presence of L-benzylsuccinic acid the reaction is inhibited [2]
Carboxypeptidase Key features of the carboxypeptidase active site: Charged arginine Forms an ionic bond with the terminal carboxylic acid Zinc ion Binds to carbonyl of terminal peptide S 1’ pocket Allows for the side chain of the terminal amino acid [2]
L-Benzylsuccinic Acid Inhibits carboxypeptidase Key features: Benzyl group to fill the S 1’ pocket Carboxylate anion for ionic interactions with arginine Second carboxylate to act as a ligand for the zinc ion Lack of a peptide bonds prevents it from being hydrolyzed and removed from the active site [2]
ACE-Inhibitors From the carboxypeptidase the ACE active site contains Arginine Zinc ion S pockets Inhibitor used = Succinyl proline Proline is located on the terminus of teprotide Distance between the dipeptide and peptide were thought to be greater than the distance between the amino acid and peptide chain Analogous to benzylsuccinic acid [2]
ACE-Inhibitors Next developments increased binding affinity Captopril Methyl group to fill S 1’ Thiol added to interact with zinc Enalaprilat Glutarylproline replaced succinyl proline to better fit the S 1 pocket Lisinopril Similar to enalaprilat with a aminobutyl substitutent replacing methyl substitutent [2]
ACE-Inhibitors [1]
Sulfhydryl-containing ACE-Inhibitors Captopril Active compound 75% bioavailability, which can be reduced by food Take 1 hour prior to food consumption Eliminated in the urine Captopril, captopril disulfide dimmers, and captoprilcysteine disulfide http: //home. caregroup. org/clinical/altmed/interactions/Drugs/Captopril. htm
Dicarboxyl-containing ACE-Inhibitors Enalapril Prodrug, activated in vivo to enalaprilat C 2 H 5 group is hydrolyzed by esterases in the liver Eliminated by the kidneys Enalapril and enalaprilat Bioavailability of 60%, not reduced by food Enalaprilat Active dicarboxylic acid Not orally stable IV administration only
Dicarboxyl-containing ACE-Inhibitors Lisinopril Active molecule Lysine analogue of enalaprilat Characterized by: Slow, variable, & incomplete absorption (30%- not reduced by food) Eliminated intact by the kidneys Benazepril Prodrug, activated to be benazeprilat Eliminated by kidney and liver via urine and bile High potency in vitro with a low uptake, 37%- can be reduced when food is present
Dicarboxyl-containing ACE-Inhibitors Trandolapril Prodrug, activated to trandolaprilat Active form has 70% bioavailability, slowed by food Eliminated in urine (33%) and feces (66%) Quinapril Prodrug, activated to quinaprilat 60% absorption, slowed by food Two half-lives in the body Initial ~2 hours Prolonged ~25 hours Due strong binding with tissue ACE
Dicarboxyl-containing ACE-Inhibitors Ramipril Prodrug, active form ramiprilat Created via cleavage of ester moiety Rapidly absorbed, slowed by food Triphasic elimination half-life: Initial 2 -4 hours Intermediate 9 -18 hours Extensive tissue distribution Clearance of free ramiprilat from plasma Terminal 50+ hours Dissociation from tissue ACE
Dicarboxyl-containing ACE-Inhibitors Moexipril Prodrug, active form is moexiprilat 13% bioavailability for moexiprilat due to incomplete absorption of moexipril Take 1 hour prior to food consumption http: //www. geocities. com/lubolahchev/Moexipril. html Perindopril Prodrug, active form is perindoprilat 75% bioavailability for the prodrug 35% bioavailability for the active form, reduced in the presence of food Eliminated by the kidneys http: //www. fortunecity. com/roswell/spells/260/c 9900109. gif
Phosphorous-containing ACE-Inhibitors Fosinopril Prodrug converted to fosinoprilat Slow absorption, slowed further by food 36% uptake Eliminated by kidneys and liver Dual elimination allows for use despite the presence of renal disease http: //en. wikipedia. org/wiki/Monopril
Side Effects of ACE-Inhibitors http: //www. beauregard. org/bldpress. htm Hypotension with the first dose Dry cough 5 -20% of people Hyperkalemia (High K+ levels) Acute renal failure Fetopathic effects in pregnant women Skin rash Dysgeusia, loss of taste
The Future of ACE-Inhibitors In 2003 X-ray crystallography revealed the structure of ACE joined with lisinopril. Indicated that the arginine is actually a lysine residue Possibility of new inhibitors with greater binding capabilities and greater selectivity http: //www. cbi. cnptia. embrapa. br/~jorgehf/index 2. html
Print Sources: Sources 1. Brunton, Laurence L. , John S. Lazo, and Keith L. Parker, eds. The Pharmacological Basis of Therapeutics. 11 ed. New York: Mc. Graw-Hill, 2006. 2. Patrick, Graham L. An Introduction to Medicinal Chemistry. 3 ed. New York: Oxford University Press, 2005. Online Sources: 3. www. aurorahealthcare. org 4. www. healthatoz. com 5. www. americanheart. org 6. www. drugdigest. org 7. http: //www. beauregard. org/bldpress. htm 8. http: //www. everybody. co. nz/page-3 f 71418 a-d 1 e 1 -43 d 7 -9 ac 0 -fdcb 4 a 79 a 3 e 3. aspx 9. http: //www. merck. com/media/mmhe 2/figures/fg 022_2. gif 10. http: //member. rivernet. com. au/balehirs/dr. Ht 2. jpg 11. http: //www. physicaltherapy. ca/cardio/Hypertension 1. html 12. http: //www. szgdocent. org/resource/rr/c-viper. htm 13. http: //home. caregroup. org/clinical/altmed/interactions/Drugs/Captopril. htm 14. http: //en. wikipedia. org/wiki/Enalapril 15. http: //www. medsafe. govt. nz/profs/Datasheet/p/prinzidepic 1. gif 16. http: //www. alchemchina. com/products/apis_b. files/Benazepril. gif 17. http: //www. drugs. com/pdr/images/10/04044002. jpg 18. http: //www. medicinescomplete. com/mc/clarke/current/images/clk 1438 c 001. gif 19. http: //www. smspharma. com/images/ramipril_img. gif 20. http: //www. geocities. com/lubolahchev/Moexipril. html 21. http: //www. fortunecity. com/roswell/spells/260/c 9900109. gif 22. http: //en. wikipedia. org/wiki/Monopril 23. http: //www. beauregard. org/bldpress. htm 24. http: //www. cbi. cnptia. embrapa. br/~jorgehf/index 2. html For more detailed citations, please see accompanying paper.