Pulmonary Hypertension Kazemi toba M D Birjand University

Pulmonary Hypertension Kazemi. toba, M. D. Birjand University of Medical Sciences 24 th Ordibeheshte 1390

Outline Introduction, definition n Pathophysiology n Diagnosis n Laboratory Findings n Idiopathic Pulmonary Arterial Hypertension n Natural History n Treatment n

Introduction n Pulmonary hypertension: Ø an abnormal elevation in pulmonary artery pressure result of left heart failure, pulmonary parenchymal or vascular disease, thromboembolism, or a combination of these factors. Regardless the etiology of pul. htn, it is a feature of advanced disease. it is essential that the etiology underlying the pulmonary hypertension be clearly determined before treatment. Ø Ø Ø n Cor pulmonale : ü RV enlargement secondary to any underlying cardiac or pulmonary disease. Pulmonary hypertension is the most common cause of cor pulmonale. Advanced cor pulmonale is associated with the development of RV failure. ü

Cor pulmonale
 is based upon right heart catheterization measurements.")
DEFINITION The definition of pulmonary hypertension (PH) is based upon right heart catheterization measurements. n PH is defined as a mean pulmonary artery pressure greater than 25 mm. Hg at rest. n A mean pulmonary artery pressure of 8 to 20 mm. Hg at rest is considered normal, . n
 LV transmural filling pressure=")
Pathophysiology Dilated RV- Intact pericardium RAP Intrapericardial pressure (IPP) LV transmural filling pressure= LVEDP-IPP + Shift of IV septum toward LV preload and LV distensibility Systemic Cardiac Output

Pathophysiology n n n The ability of the RV to adapt to increased vascular resistance is influenced by several factors, including age and the rapidity of the development of pulmonary hypertension Acute: RV afterload, EDV, EF, SV of RV Chronic: progressive systolic pressure overload of RV that dilates and hypertrophies, gradual RV dysfunction venous return compromises RV preload and pulm blood flow Coexisting hypoxemia can impair the ability of the ventricle to compensate

Pathogenesis of Pulmonary Arterial Hypertension NORMAL REVERSIBLE DISEASE IRREVERSIBLE DISEASE


Symptoms of PH Dyspnea n Fatigue 19% n Near syncope/syncope n Chest pain n Palpitations n Leg edema n 60% 13% 7% 5% 3%
 n Left parasternal lift (RV")
Physical Exam JVD n Loud P 2 (increases PAP) n Left parasternal lift (RV heave=R sided overload) n murmur of TR n S 3 gallop (advanced RV failure) n CLEAR lungs n

Signs of Disease Severity n n n Dyspnea at rest Low cardiac output with metabolic acidosis Hypoxemia Signs of right heart failure (large V wave on jugularis vein, periph edema, hepatomegaly) Syncope (poor prognosis) Chest pain (2 to RV ischemia)

Diagnosis u CXR: Enlarged proximal u ECG: RAD, RAE, RVH most u Echo : Estimate PA pressure pulmonary vessels, ” common Assess for shunts and valvular disease; ventricular function

ECG Findings n Often suggest ive of RVH and RAE

RAE, RVH

Chest X-ray Findings n central Pul arterial and/or RV enlargement , distal “pruning”


. Note the dilated proximal pulmonary arteries with a relative lack of pulmonary vasculature in the periphery. No cardiomegaly is noted.

Chest roentgenogram from a patient with primary pulmonary hypertension showing the marked dilation of the main pulmonary arteries and right ventricular enlargement.

Pulmonary hypertension. Chest radiograph in a patient with secondary pulmonary hypertension reveals enlarged pulmonary arteries. This patient was found to have an atrial septal defect.

Severe right chamber dilation üEstimate PA pressure üAssess for shunts üand valvular disease ü ventricula r function

secondary pulmonary hypertension
 u")
Severity of Pulmonary Hypertension n Degree of disease n Mean PAP (mm. Hg) u Mild u 25 - 40 u Moderate u 41 - 55 u Severe u >55

Right Heart Cath n Essential for firm diagnosis: u Helps to not dx people with PAH that do not have it! u Vasoreactivity testing t NO, Adenosine—drop in m. PAP by 10 mm. Hg to value < 40 mm. Hg t Predicts CCB response u Evaluate for septal defects u Shed light on the issue of diastolic dysfunction u Interpret data in context of patient’s volume status

Lab Exam n Selected labs u ANA, RF, ESR u LFTs, hepatitis serologies u HIV antibody u Drugs (cocaine)

Algorithm for investigation of suspected PH

. n Blood clots. n Arrhythmia.")
Complications of PH n Right-sided heart failure (cor pulmonale). n Blood clots. n Arrhythmia. Irregular heartbeats from the upper or lower chambers of the heart are complications of pulmonary hypertension. These can lead to palpitations, dizziness or fainting and can be fatal. n Bleeding. Pulmonary hypertension can lead to bleeding into the lungs and hemoptysis.
")
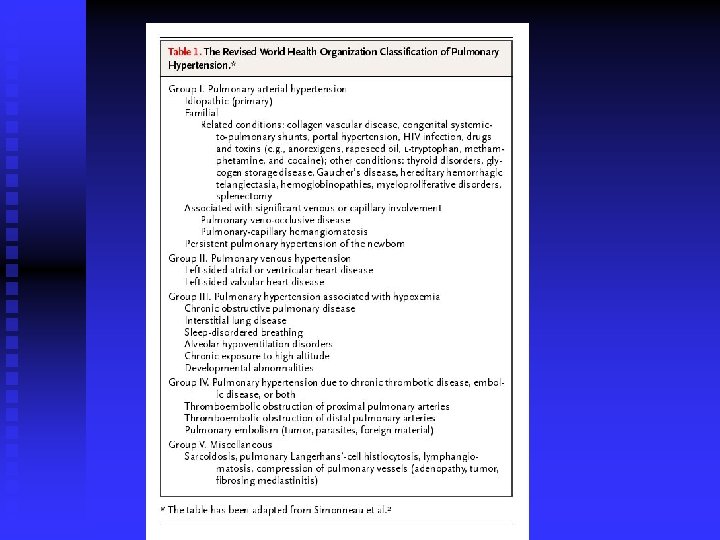
Classification Group 1 "Pulmonary arterial hypertension". u u u 1. 2. 3. Idiopathic (IPAH) Familial (FPAH) Associated with (APAH): t Collagen vascular disease t Congenital systemic-to-pulmonary shunts t Portal hypertension t HIV infection t Drugs and toxins t Other (thyroid disorders, glycogen storage disease, Gaucher disease, hereditary hemorrhagic telangiectasia, hemoglobinopathies, myeloproliferative disorders, splenectomy) 4. Associated with significant venous or capillary involvement t Pulmonary veno-occlusive disease (PVOD) t Pulmonary capillary hemangiomatosis (PCH) 5. Persistent pulmonary hypertension of the newborn

Classification n Group 2 : "Pulmonary venous hypertension". Examples: t t n 1. Left-sided atrial or ventricular heart disease 2. Left-sided valvular heart disease Group 3 PH — "Pulmonary hypertension associated with disorders of the respiratory system or hypoxemia". Examples: t t t 1. Chronic obstructive pulmonary disease 2. Interstitial lung disease 3. Sleep-disordered breathing 4. Alveolar hypoventilation disorders 5. Chronic exposure to high altitude 6. Development abnormalities

Classification n Group 4 PH — "Pulmonary hypertension caused by chronic thrombotic or embolic disease". Examples: t t t n 1. Thromboembolic obstruction of proximal pulmonary arteries 2. Thromboembolic obstruction of distal pulmonary arteries 3. Non-thrombotic pulmonary embolism (tumor, parasites, foreign material) Group 5 PH — These patients have PH caused by inflammation, mechanical obstruction, or extrinsic compression of the pulmonary vasculature (eg, sarcoidosis, histiocytosis X, lymphangiomatosis, compression of pulmonary vessels by adenopathy, and fibrosing mediastinitis).
 PAH Respiratory")
Pulmonary Hypertension: Define Lesion Post-Capillary PH (PCWP>15 mm. Hg; PVR nl) PAH Respiratory Diseases PE VC RA RV PA Pre-capillary PH PCWP<15 mm. Hg PVR > 3 Wu Atrial Myxoma Cor Triatum MV Disease PC PV LA LV LVEDP PV compression PVOD Ao Systemic HTN Ao. V Disease Myocardial Disea DCM, HCM, ischemic CM RCM, Obesity , others

Idiopathic PH PPH n uncommon, n incidence : 2 cases per million. n female predominance n presenting in the 4 th and 5 th decades n although the age range is from infancy to >60 years. n Familial PAH : 20% of cases of IPAH n autosomal dominant inheritance n

Natural History of PPH n n n The natural history of IPAH is uncertain the disease is typically diagnosed late Prior to current therapies, a survival of 2– 3 years from the time of diagnosis Functional class remains a strong predictor of survival, patients who are in NYHAfunctional class IV having a mean survival of <6 months. The cause of death is usually RV failure, which is manifest by progressive hypoxemia, tachycardia, hypotension, and edema

")
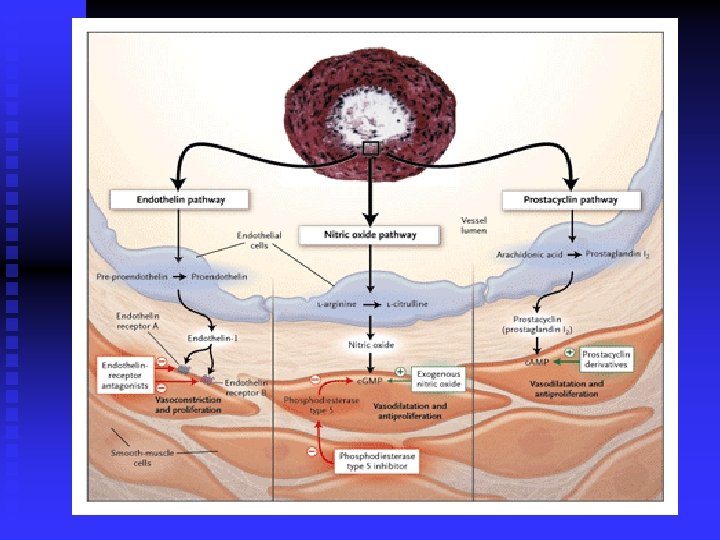
Mediators of PH Prostacycline n Thromboxane A 2 n Endothelin-1 n Nitric Oxide (NO) n Serotonin n Adrenomedullin n Vasoactive Intestinal Peptide (VIP) n Vascular Endothelial Growth Factor (VEGF) n

Prostacycline & Thromboxane A 2 Prostacycline u Vasodilator u Inhibits platelet activation u Antiproliferative properties n Thromboxane A 2 u Vasoconstrictor u Platelet agonist n in PH balance shifted to Thromboxane A 2 n

ENDOTHELIN-1 Potent vasoconstrictor n Stimulates proliferation of smooth muscle cells in PA n Plasma levels increased in PHT n Level inversely proportional to pulmonary blood flow & CO - ? Direct effect n

NO & serotonin NO u Vasodilator & inhibitor of platelet activation & vascular SM proliferation n Serotonin u Vasoconstrictor promoting SM hyperplasia & hypertrophy u Elevated plasma levels/ reduced platelet levels in PHT n

Goals of Therapy Alleviate symptoms, improve exercise capacity and quality of life n Improve cardiopulmonary hemodynamics and prevent right heart failure n Delay time to clinical worsening n Reduce morbidity and mortality n
 n Oxygen n PAH")
Classes of therapy Medical n Diuretics n Coumadin (IPAH, Anorexigen) n Oxygen n PAH specific therapy n Surgical therapy n Atrial septostomy n Lung transplantation n

PAH Therapy: Life style considerations n Sodium restriction n Abstinence from smoking n Avoid high altitude t <4, 000 feet above sea level n Avoid physical exertion in setting of pre- or frank syncope sx n Avoid pregnancy

Mainstay of treatment

ANTICOAGULANTS n Warfarin u Anticoagulant therapy is advocated for all patients with PAH. u warfarin increases survival of patients with PAH. u The dose of warfarin is generally titrated to achieve an INR of 2– 3 times control.

Algorithm for Assessment of Vasoreactivity in Patients with PAH Right Heart Catheterization With Acute Vasoreactivity Testing (i. NO, epoprostenol, adenosine) m. PA 10 mm. Hg m. PA < 40 mm. Hg Non - responder Consider p. o. Bosentan Consider p. o. Sildenafil Consider Inhaled Iloprost Consider s. q. Treprostinil Consider Continuously. Infused Epoprostenol Responder (<15%) and candidate for CCB (no RHF) Hemodynamically-Monitored Trial of Calcium Channel Blocker Therapy

Calcium Channel Blockers n n n Patients who have substantial reductions in PAP in response to vasodilators at the time of cardiac catheterization (a fall of 10 mm. Hg in mean PAP and a final mean pressure <40 mm. Hg) should be treated with CCB. dramatic reductions in PAP, PVR, improved symptoms, regression of RV hypertrophy improved survival documented to exceed 20 years patients require high doses (e. g. , nifedipine, 240 mg/d, or amlodipine, 20 mg/d). <20% of patients respond to CCB in the long term. should not be given to patients who are unresponsive, as they can result in hypotension, hypoxemia, tachycardia, and worsening right heart failure

Endothelin Receptor Antagonists n n n Bosentan : nonselective endothelin receptor antagonist approved treatment of PAH for patients who are NYHA functional classes III and IV. bosentan improved symptoms and exercise tolerance Therapy is initiated at 62. 5 mg bid for 1 month, then increased to 125 mg bid. Because of the high frequency of abnormal hepatic function tests associated with drug use, primarily an increase in transaminases, it is recommended that liver function be monitored monthly throughout the duration of use. Bosentan is also contraindicated in patients who are on cyclosporine or glyburide concurrently.

PHOSPHODIESTERASE INHIBITORS n n n Sildenafil u PDE type 5 inhibitor u Reduce metabolism of c. GMP Sildenafil should not be given to patients who are taking nitrate compounds lowers pulmonary artery pressure and inhibits pulmonary vascular growth sildenafil improves symptoms and exercise tolerance in PAH The recommended dose is 20 mg tid. The most common side effect is headache

Prostacyclins n 1 -Iloprost u IV or Inhaled u is approved via inhalation for PAH patients who are NYHA functional classes III and IV. u improve symptoms and exercise tolerance u Therapy can be given at either 2. 5 or 5 mcg per inhalation treatment. u inhaler must be given by a dedicated nebulizer u The most common side effects are flushing and cough u Because of the very short half-life (<30 min) it

Prostacyclins n 2 -Treprostinol u is approved for the treatment of PAH patients who are NYHA functional class III or IV u improvement in symptoms, exercise tolerance, and survival u drug is administered iv u requires placement of a permanent central venous catheter and infusion through an ambulatory infusion pump system. u Side effects include flushing, jaw pain, and diarrhea,
 • SQ administration • Longer half-life than epoprostenol • Pre-mixed")
Subcutaneous Treprostinil (Remodulin ) • SQ administration • Longer half-life than epoprostenol • Pre-mixed • Stable at room temperature
")
IV epoprostenol (flolan)

Prostacyclins n 3 - Treprostinil n an analogue of epoprostenol, for patients with PAH &NYHA classes II–IV. Treprostinil has longer half-life than epoprostenol (4 h) is stable at room temperature, may be given iv or sc through a small infusion pump that was originally developed for insulin. improvement in symptoms and exercise capacity. The major problem has been local pain at the infusion site, which has caused many patients to discontinue therapy. Side effects are similar to those seen with epoprostenol. Ø Ø Ø Ø

Surgical Therapy n Transplantation - lung / heart-lung t t t Lung transplantation is considered for patients who, while on an intravenous prostacyclin, continue to manifest right heart failure. Acceptable results have been achieved with heart -lung, bilateral lung, and single-lung transplant. The availability of donor organs often influences the choice of procedure

Functional classes

Good luck
- Slides: 58