Chronic Liver Disease CLD is characterized by varying

Chronic Liver Disease. CLD: is characterized by varying degree of hepatocellular necrosis, inflammation and fibrosis. Decompensated liver disease: CLD with encephalopathy, coagulopathy, ascites, fetor hepaticus.

STRUCTURE OF LIVER.

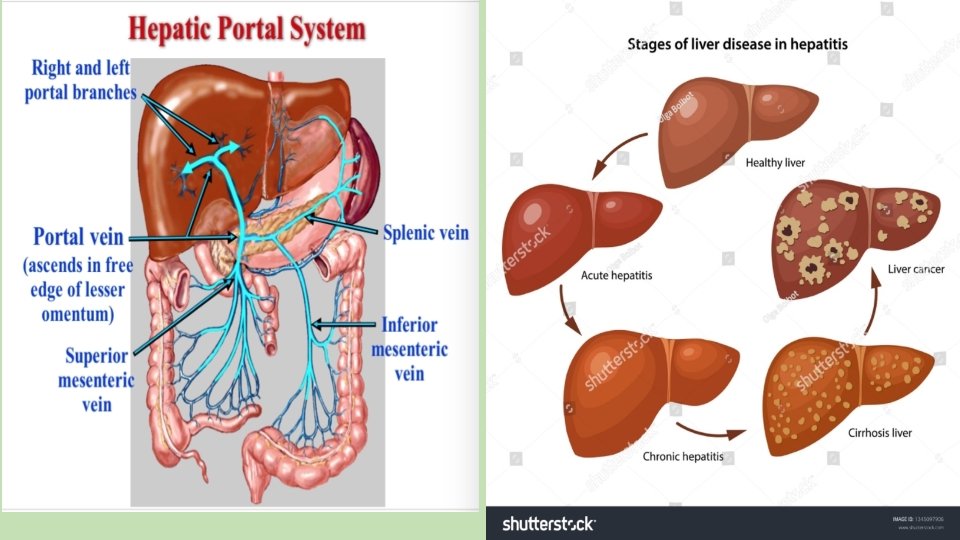
ETIOLOGY: A. Chronic viral hepatitis: Hepatitis B, C, D. B. Metabolic disorders: Wilson disease, alpha 1 antitrypsin deficiency, galactosemia, C. Autoimmune hepatitis: Anti-liver-kidney microsomal antibody, Antiactin antibody positive A. Drug induced hepatitis: INH, methyldopa. B. unknown

PRESENTATION OF CLD: • ASYMPTOMATIC: No any sign and symptoms of CLD, only raised ALT. • ACUTE HEPATITIS: CLD may present with acute hepatitis like features. • MILD OR NO JAUNDICE ONLY HEPATOSPLENOMEGALY. • STIGMATA OF CLD.
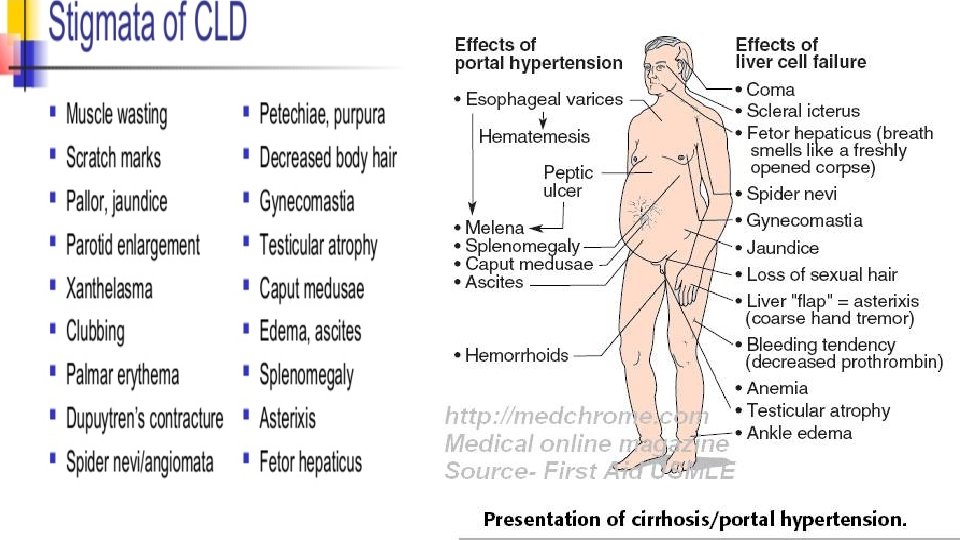
,")
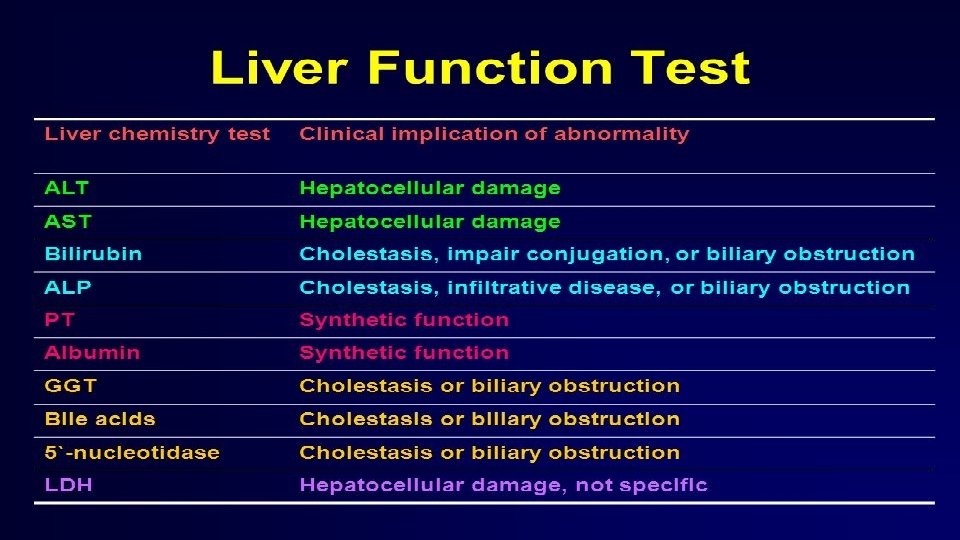
INVESTIGATIONS: A. To reach the diagnosis of disease # Liver function tests: Serum bilirubin(direct/indirect), ALT, AST, Alkaline phosphatase, prothrombin time, Serum albumin. # Ultrasonography of abdomen. #Liver biopsy is need for confirmation. B. To see the etiology of disease: *Viral markers: HBs. Ag, HBe. Ag, Anti-HCV , *24 hour urinary copper-penicillamine challenge test(Wilson disease). *Serum ceruloplasmin (Wilson disease). *Auto-antibody— ANA, Anti liver kidney antibody, Anti SMA antibody(Autoimmune disease) *Urinary reducing sugar(Galactosemia)
To see complication of disease * Endoscopy of upper GIT: to rule out")
INVESTIGATIONS C)To see complication of disease * Endoscopy of upper GIT: to rule out Portal hypertension. * Electrolytes: Hypokalemia, hyperkalemia, hyponatremia, metabolic acidosis. * Blood ammonia level increased(Hepatic encephalopathy). * Ascitic fluid analysis: if CLD with ascites.
 Asymptomatic: Treatment of etiology like,")
MANAGEMENT • Management depends on presentation of CLD: A) Asymptomatic: Treatment of etiology like, If Chronic Hepatitis B infaction with HBe. Ag and high HBV DNA level treated with lamivudine, Interferon alfa 2 b, Adefovir. • Wilson disease: Copper chelating agent Penicillamine(10 mg/kg/d). • Autoimmune hepatitis: Prednisolone at 1 -2 mg/kg. • B) CLD with complection: Ascitis-Bed rest, Minimum cocking salt, Fluid restriction- Previous day output plus 400 ml/sqm of body surface area/day, Diuretics : Spironolactone(1 mg/kg day), if not control add furosemide(1 -2 mg/kg/day). Ascites not response to high dose of diuretic is called Refractory ascites, treated with 20% albumin and paracentesis.

Encephalopathy: üAvoidance of precipitating factors, protein restricted , üLactulose 10 -50 ml 4 hourly , Neomycin, to prevent ammonia production. üCerebral edema: Corticosteroid, Osmotic diuretics-Mannitol. üH 2 blocker, correction of electrolytes, üTREATMENT OF COAGULOPATHY: Parental vit k, infusion of FPP, Plasmapheresis. üTreatment of portal hypertension.

Precipitating factors for Hepatic encephalopathy: § High protein diet, GI Bleeding, constipation, § Hypoglycemia, hypokalemia, hypoxia, acidosis, § CNS depressant : Benzodiazepine, phenobarbitone, diuretics.
- Slides: 14