But I only drive to the shops Mr

“But I only drive to the shops…” Mr Javeed Khan Consultant Ophthalmologist St Mary’s Hospital Isle of Wight

Driving standards What is the evidence? Age and Driving Monocular drivers Dilated pupils


Do these patients need to notify DVLA? • 45 year old with ocular hypertension • 68 year old bilateral glaucomatous field loss • 75 year old with glaucoma, field defects in one eye only • Lorry driver on Latanoprost, mild field loss in one eye • Lorry driver with colour blindness • 42 year old with night blindness

Driving is a demanding activity PERCEPTION Central Peripheral Fixation Scanning INTERPRETATION Reaction Time DECISION ACTION Motoring Ability

Is Poor Visual acuity a contributory factor in road accidents?

Is poor visual acuity a contributory factor in road accidents? From 2005 – 2009 nearly 700, 000 accidents on UK roads • 0. 4 % of fatal accidents and 0. 2 % of all accidents due to ‘defective/uncorrected eyesight’

How important is poor vision as a contributory factor in road accidents? From 2005 – 2009 nearly 700, 000 accidents on UK roads • 0. 4 % of fatal accidents and 0. 2 % of all accidents due to ‘defective/uncorrected eyesight’ • Mobile phone use 0. 2 % of all accidents

How important is poor vision as a contributory factor in road accidents? From 2005 – 2009 nearly 700, 000 accidents on UK roads • 0. 4 % of fatal accidents and 0. 2 % of all accidents due to ‘defective/uncorrected eyesight’ • Mobile phone use 0. 2 % of all accidents • ‘Failed to look properly’ 20% of fatal and 35% of all accidents • Vision affected by sun/headlights/dirty windscreen 3. 5%

VISUAL STANDARDS FOR DRIVING With both eyes open and with the aid of glasses or contact lenses if worn: • Can read number plate at 20 metres in good daylight • Snellen visual acuity 6/12 or better
 Snellen visual acuity: • Better eye 6/7. 5 • Before")
Group 2 (Lorry, Bus) Snellen visual acuity: • Better eye 6/7. 5 • Before 2012: Worse eye to be at least 6/9 • Now 6/60 acceptable in worse eye • No minimum uncorrected visual acuity • But glasses no more than + 8 dioptres


Case • Lorry driver develops posterior sub-capsular cataract in left eye, Right eye pseudophakic • VA: • Right eye: 6/6 unaided • Left eye: 6/36 unaided no improvement • Both eyes open: 6/6 • Patient doesn’t complain of glare, has full fields Can he continue to drive his lorry while waiting for cataract surgery? Yes, as long as no other visual impairment

Evidence for visual acuity standard: Why 6/12 on Snellen? In 1937 standard introduced: Number plate at 75 feet (23 metres) Equal to stopping distance at 30 mph

Evidence for visual acuity standard • As number plate sizes changed distance changed: • 20. 5 metres pre-2001 • 20 metres Current

Evidence for visual acuity standard: Why 6/12 on Snellen? • Drasdo and Haggerty 1983: • Approximates to 6/9 -2 or 6/10 based on their statistical model • Charman 1997: • Calculated Snellen equivalent as 6/15 based on angular subtense (13. 4 minutes of arc) • Current standard 6/12

How reliable is the Snellen standard in predicting number plate test results? • Currie et al BJO 2000 • 100 patients with vision 6/9 or 6/12 • Ability to read number plate tested • 26 % of 6/9 FAILED and 34% of 6/12 PASSED

Number plate difficulty T 174 ILE P 610 VOH M 528 CBY Kiel et al 2003 Mc. Monnies 1999 (Chart construction and letter legibility)

Does poor visual acuity cause accidents?

Is there a link between poor visual acuity and accidents? The evidence is WEAK from studies of accidents Greater likelihood of involvement in more than 1 accident if VA poor (Hofstetter et al 1976) Weak correlation between driving and VA (Burg et al 1976)

Is there a link between poor visual acuity and accidents? Studies of accidents: Studies not big enough to pick up statistical difference • Motor accidents are rare Owens et al: not likely to fall victim to fatal accident if drive for 3738 years • Extremes of vision in drivers is rare • People exhibit adaptive behaviour • Confounding variable e. g. glare from cataract

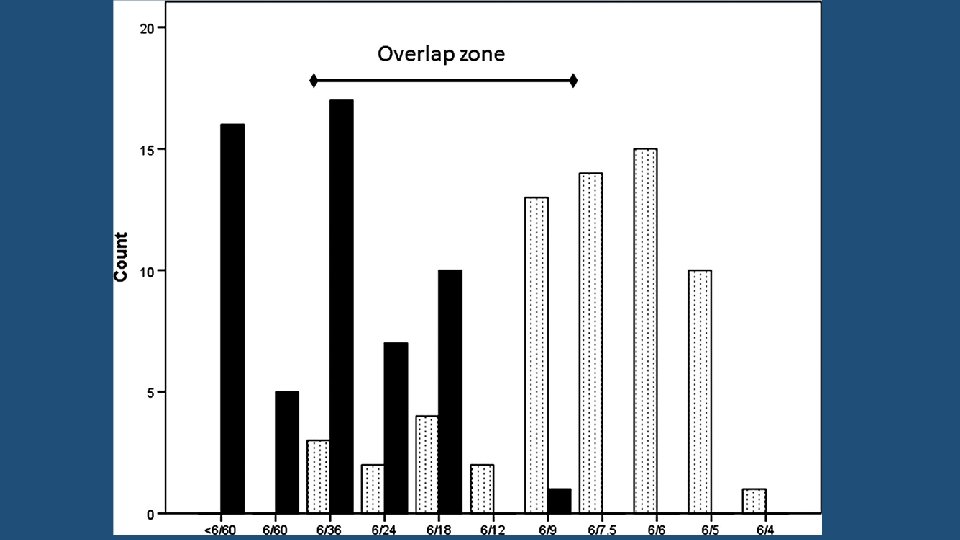
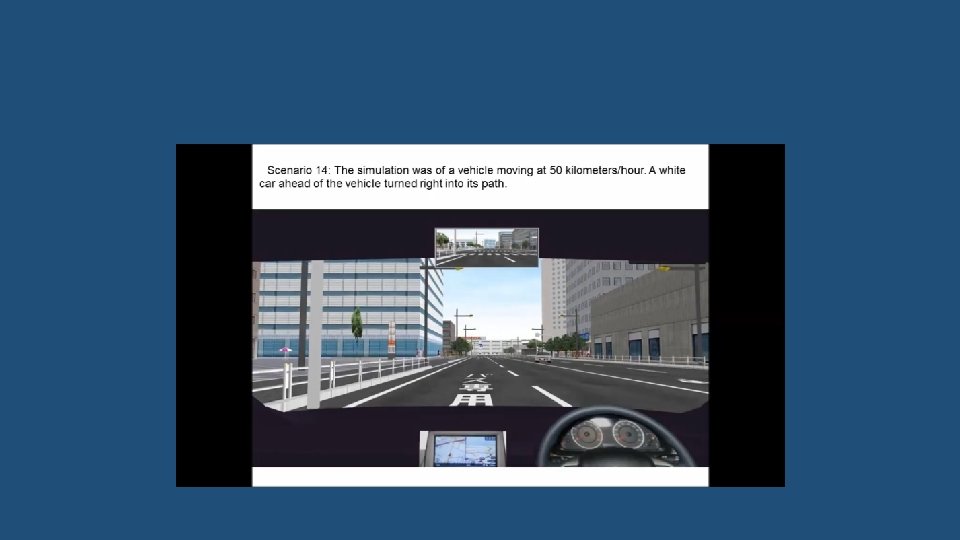
Is there a link between poor visual acuity and accidents? Studies on closed road circuits: • Poor acuity affected sign recognition and hazard avoidance • Increased time to complete circuit But • No impact on manoeuvring ability or maintaining lane position Studies on simulators • In different conditions: support the findings from closed circuit studies

Is there a link between poor visual acuity and accidents? Effect of Legislation: In Florida mandatory rescreening introduced for over 80 s Those that failed were given an opportunity to correct vision (glasses, cataract surgery etc. ) Most were able to go back to driving after correction After 3 years: Accident fatality rates in over 80 s fell by 17%

Case • Patient has cataracts • VA: • Right eye: 6/18, Left eye: 6/24 • Both eyes open: 6/12 -3 • Patient can read number plate in good light at 20 metres What must the patient do? Stop driving Offer to surrender license to DVLA Apply for restoration after successful cataract surgery

Is there a link between visual field loss and accidents?

Evidence for Visual Fields and accidents • People with visual field defects have DOUBLE the number of accidents/traffic violations • Half of the people with field loss were unaware of problems with peripheral vision • Johnson and Keltner (1983) in a study of 10, 000 drivers

Evidence for Visual Fields and accidents • Visual field size best predictor of real-world and simulator crashes and driving performance • Especially defects within 100 degrees • But actual cut-off value for standards is unclear

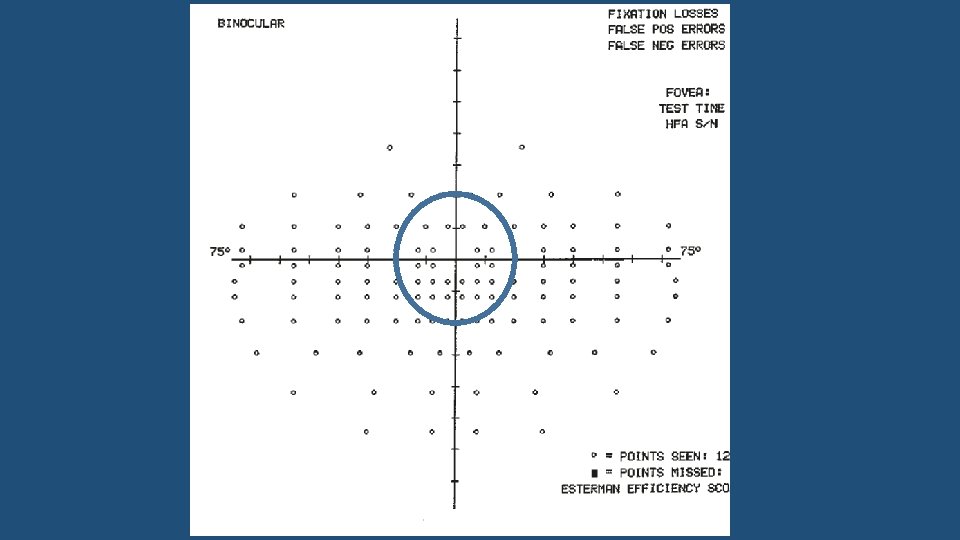
VISUAL FIELDS Tested with: • Target equivalent to white, Goldmann III 4 e settings • Esterman binocular field (sometimes Monocular fields exceptionally Goldmann) • False positive no more than 20%

Esterman Binocular Field 120 points Suprathreshold 10 d. B

Esterman Binocular Field 350 Horizontally +/- 75 degrees Superior 35 degrees Inferior 55 degrees 550

Esterman • Central +/- 20 degrees Sparse 12 points above and 22 below fixation

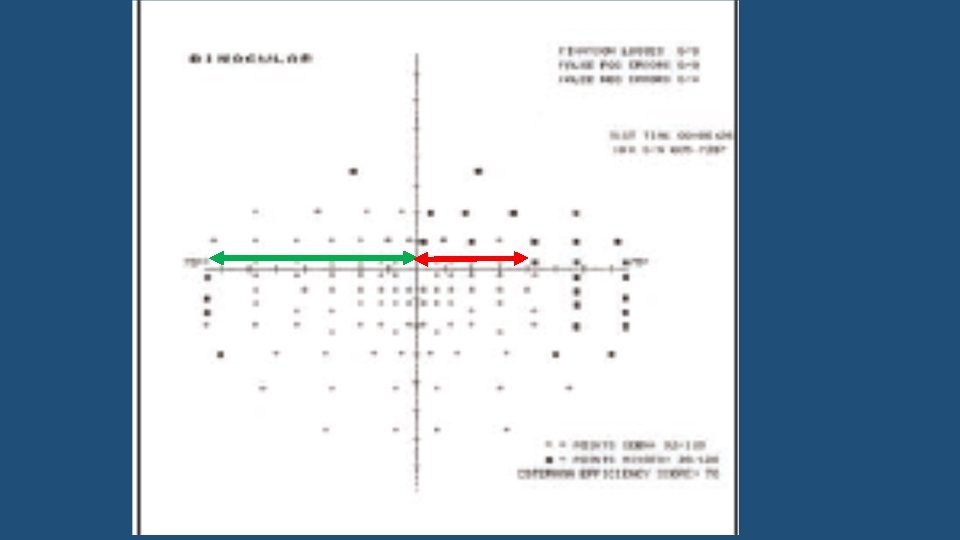
VISUAL FIELDS STANDARDS: • Field of at least 120 degrees on the horizontal • Minimum 50 degrees to left and right

750 450 600 500 700

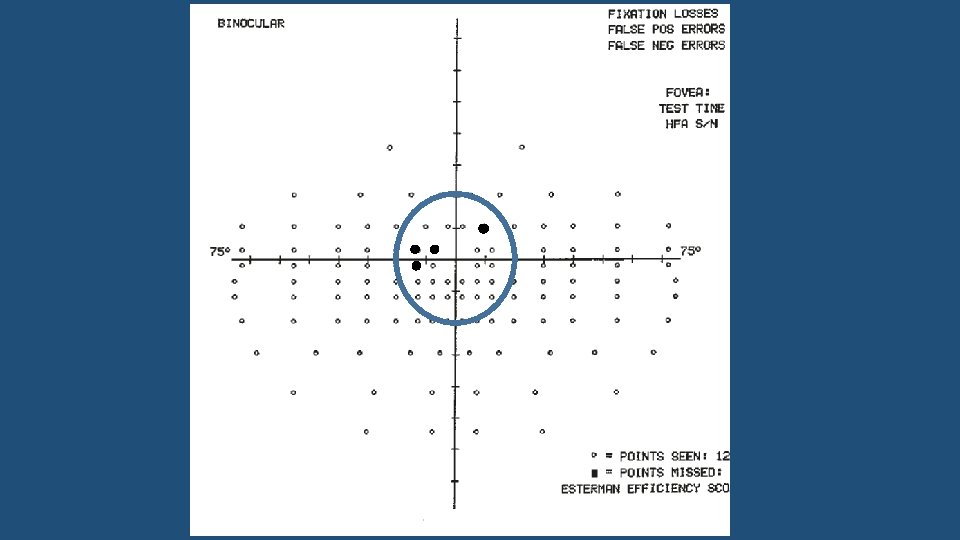
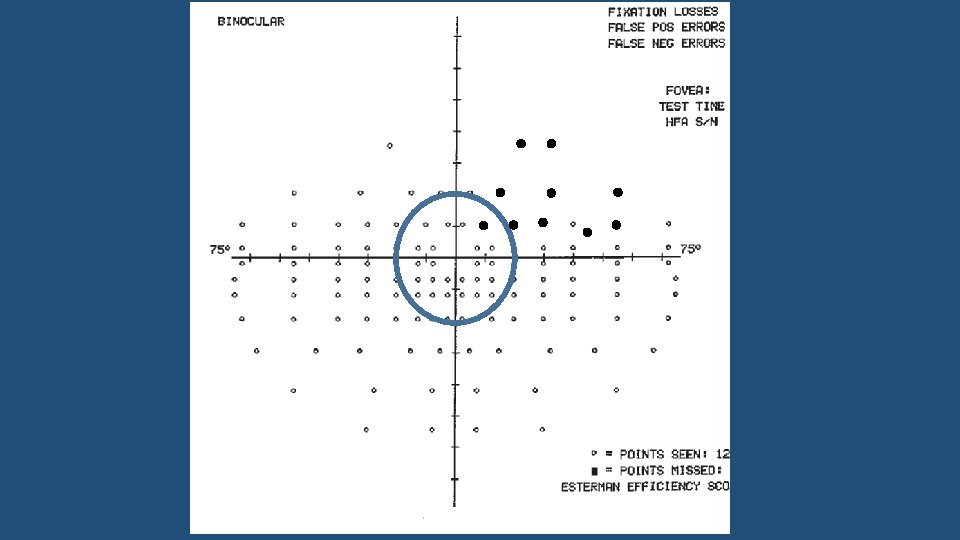
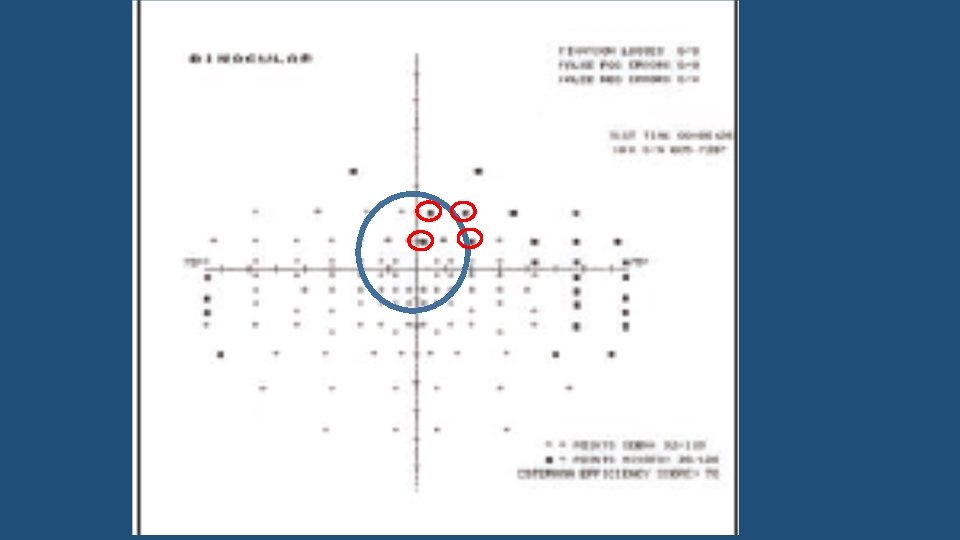
VISUAL FIELDS STANDARDS: • No significant defect in central 20 degrees of fixation above and below horizontal

Central defects • Allowed • Scattered single missed points • Single cluster of up to 3 adjoining points
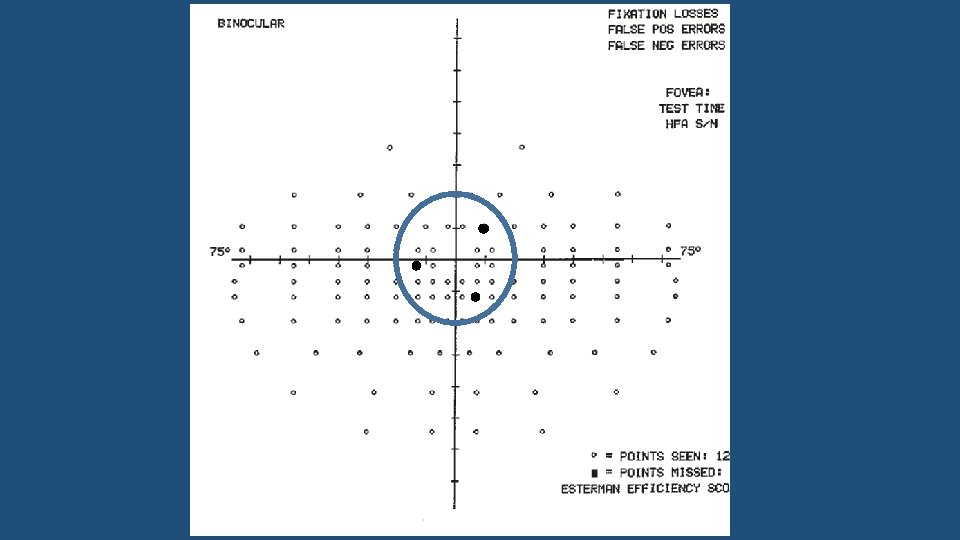
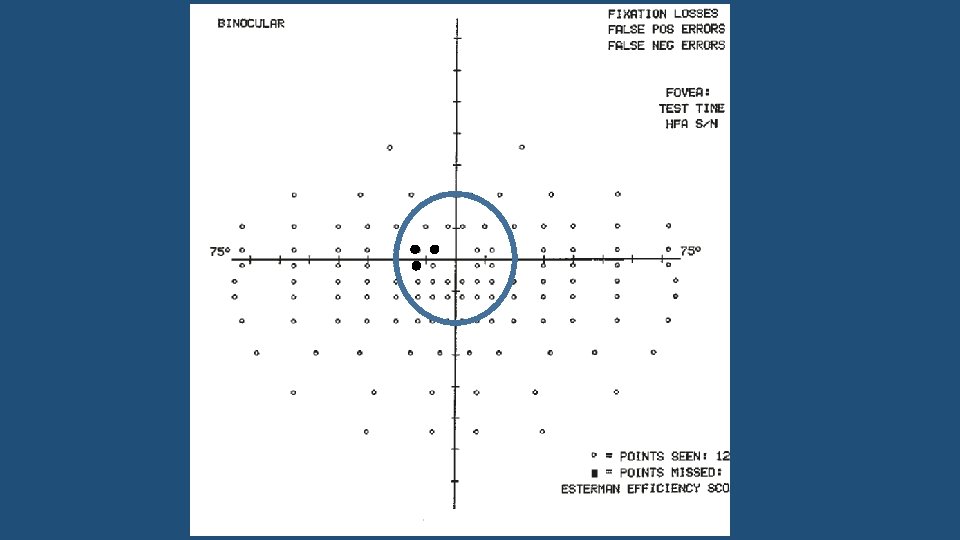

Central defects • Not Allowed • Cluster of 4 even partly within central 20 degrees • Cluster of 3 and additional single • Central extension of hemianopia/quadrantonopia greater than 3 points
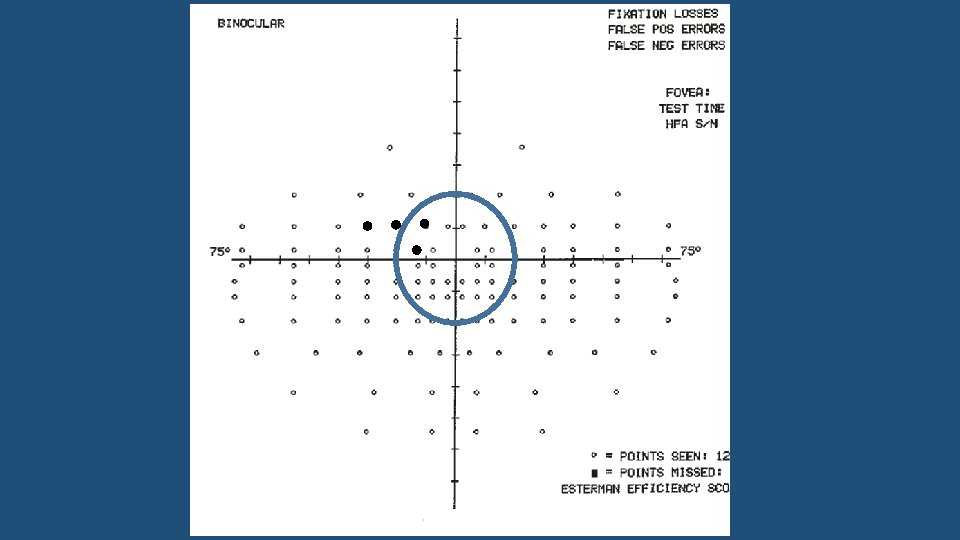

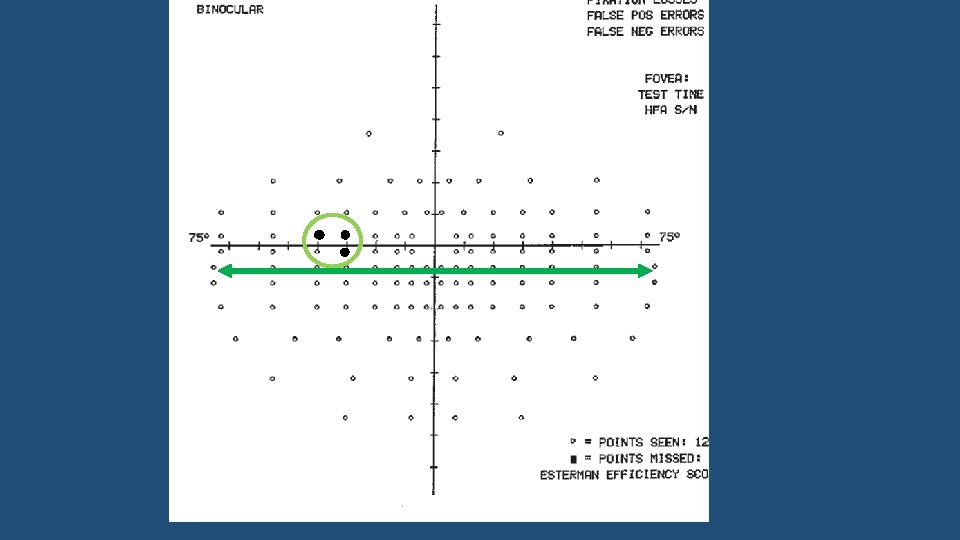
Peripheral defects Allowed Cluster of 3 on or across horizontal
 Limit of field measured at this")
Limit of field measured at this point (750) Limit of field measured at this point (500)

Peripheral defects Allowed Cluster of 3 on or across horizontal Vertical defect of any length but single point width cutting across horizontal
 Limit of field measured at this")
Limit of field measured at this point (750) Limit of field measured at this point (500)
 Limit of field measured at")
Pass? Limit of field measured at this point (750) Limit of field measured at this point (500)
 Limit of field measured at this")
Limit of field measured at this point (750) Limit of field measured at this point (500)


Case Patient must: Stop Driving Notify DVLA will arrange Esterman, license may be revoked After 12 months: May re-apply as an exceptional case if: Non-progressive, no other ocular pathology or impairment And Full functional adaptation And Satisfactory practical driving assessment

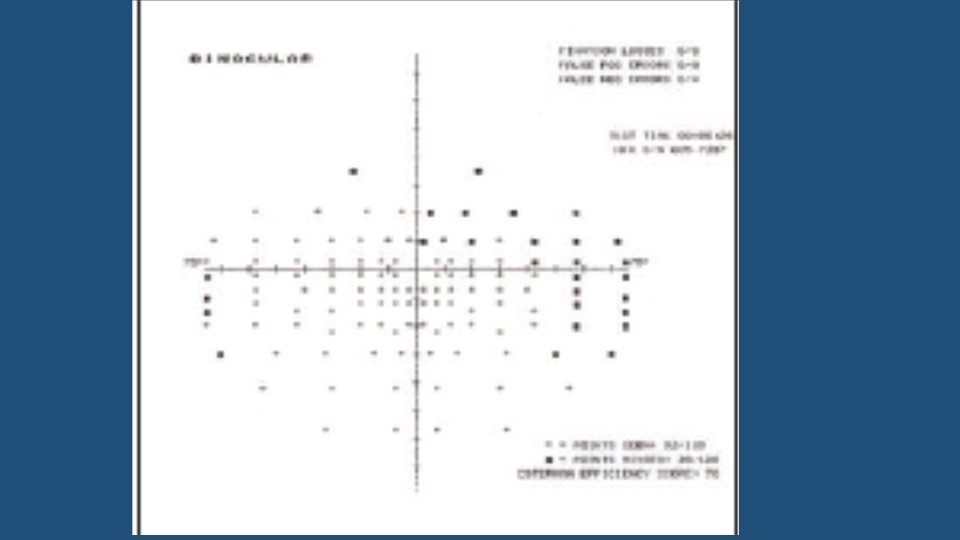
Problems with Esterman fields
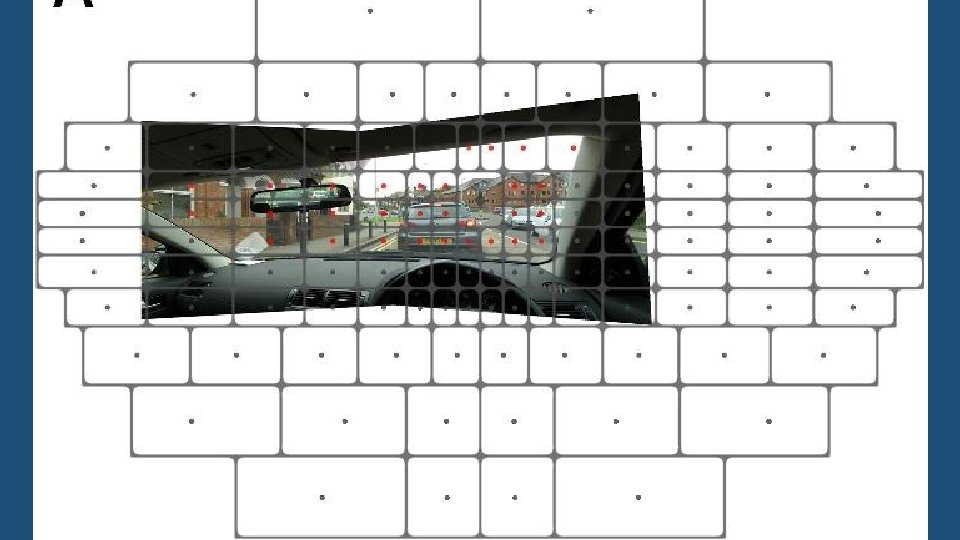

‘Only 25% of measured points fall within the most functionally relevant area’ Rauscher et al, UK department of transport 2007

Esterman field problems • Too many inferior points • Many points on right side periphery irrelevant for RHD cars
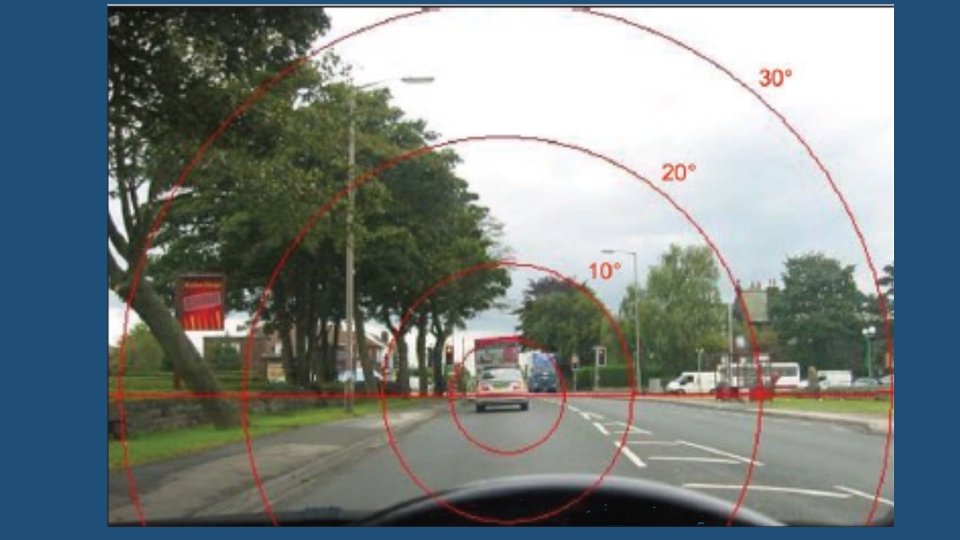

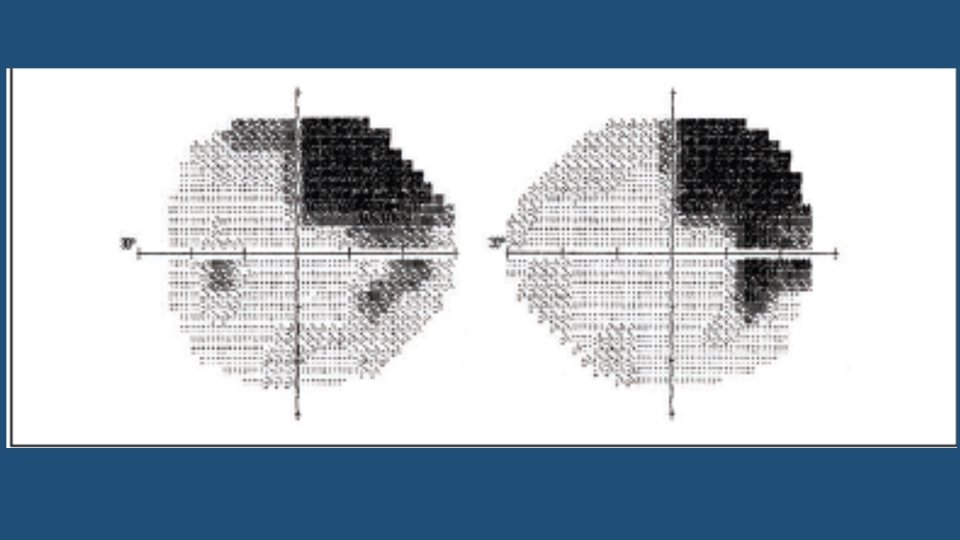
Superior v Inferior field defect simulation • Hazard perception test score: Significantly worse with superior defect than with inferior • Crabb et al in a study of 30 UK drivers

Esterman field problems • Stimulus too bright in centre • No points tested in central 7. 5 degrees

Esterman field problems • Difficulty with fixation monitoring • Too lenient? • Alternatives in the future: • Humphrey fields integration • Traffic algorithm

Other relevant tests for visual function • Contrast Sensitivity • Glare Sensitivity • Useful Field of View (UFOV)

Other relevant tests for visual function • Contrast Sensitivity • Grey letters against white background • Simulates night driving ( e. g. ‘detecting dark coated pedestrian at night’) • Stronger correlation with crashes than visual acuity Martoletti et al 1998, Dunne et al 1998 TWICE the risk

Other relevant tests for visual function • Contrast Sensitivity • Pelli Robson • But no normative database across centres • No accepted cut-off values

Other relevant tests for visual function • Glare Sensitivity • Sensitivity to glaring light sources (setting sun, headlights) • Increased relative risk of accidents (von Hebenstreit 1995, Lachenmayr 1998) • But no established methods (Straylight measurement being developed) or adequate cut-off values
 • Tests")
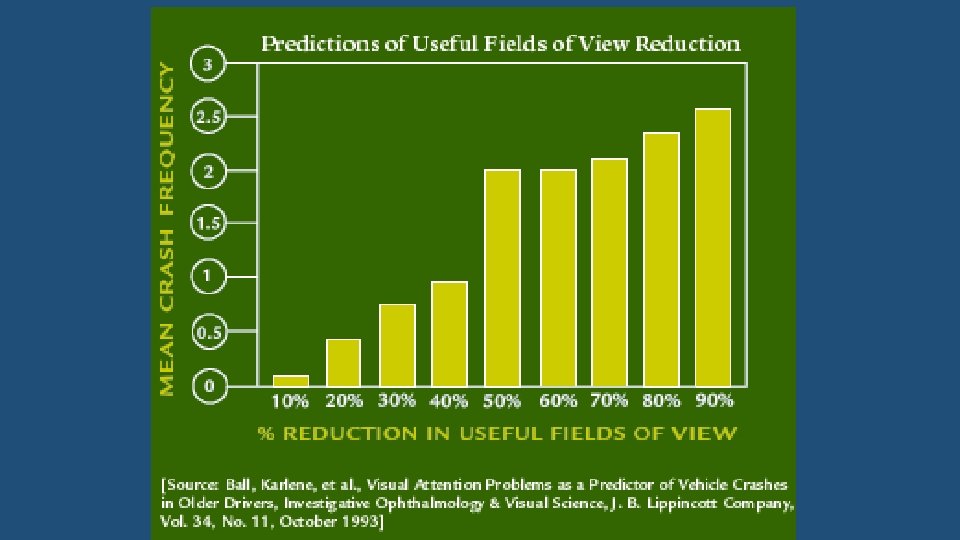
Other relevant tests for visual function • Useful Field of View (UFOV) • Tests ability to perform simultaneous detection tasks • Combines visual task with neuro-psychological task of attention • Predicts fitness to drive

Identify Central target Localize additional target With Distractors

Problems with UFOV May be difficult to interpret Expensive Performance may improve with practice

Age and Driving

Driving and the older driver • Decline in sensory, cognitive and motor function • Increased reaction time • Reduced motoring ability • Reduction in Contrast sensitivity • Difficulty seeing road signs • Visual acuity, Visual field sensitivity and stereoacuity • Problems at intersections • Increased glare sensitivity • Difficulty seeing road markings • Increased cataract, AMD and glaucoma • Personality: Increased hesitancy

Useful Tests in older drivers

Coping with reduced functions Self-imposed limits Advantage of experience: Diminishes with increasing impairment due to age

Advantage of experience: Age group 40 -60 Compensates for impairments but at the cost of increased stress

Accidents by age

Accidents by age Older drivers more likely to have: • Multi vehicle accidents • Fatal accidents • Accidents in inner city roads not on country roads • Accidents at junctions and intersections • Failure to give way • Right turns

If standards met but driver unsure • Self-regulation • Family and friends • Driving assessed in a confidential and objective test from Royal Society for the Prevention of Accidents (Ro. SPA)

Who needs to inform DVLA: (Failure to inform: £ 1000 fine and possible prosecution if accident) STOP DRIVING: • Any condition if fail to meet visual standards • Bilateral field defects e. g. hemianopia, quadrantonopia, glaucomatous • Diplopia

Who needs to inform DVLA: (Failure to inform: £ 1000 fine and possible prosecution if accident) • Bilateral conditions even if standards achieved • Glaucoma, Diabetic retinopathy, AMD, BRVO, cataract • If both eyes affected • Inform DVLA if: • Laser in both eyes • Vision problems in both eyes

Do these patients need to notify DVLA? • 45 year old with ocular hypertension No • 68 year old bilateral glaucomatous field loss Yes • 75 year old with glaucoma, field defects in one eye only No • Lorry driver on Latanoprost, mild field loss in one eye Yes • Lorry driver with colour blindness No • 42 year old with night blindness Yes

Who needs to inform DVLA: (Failure to inform: £ 1000 fine and possible prosecution if accident) • Blepharospasm: cannot drive if severe • Night blindness: considered on individual basis • Nystagmus • Optic Neuritis/atrophy • Tunnel Vision

DIPLOPIA • Cease driving at diagnosis • Inform DVLA • Resume driving after confirming to DVLA that diplopia controlled with glasses/patch If patch must satisfy conditions for monocularity • Exception: • Stable diplopia of 6 months or more: uncorrected If consultant support indicating satisfactory functional adaptation

QUAD BIKES

Anyone got a spanner?

Mobility Scooters • Class 3 can be driven on roads maximum speed 8 mph • Recommended that should be able to read number plate at 12. 3 metres (40 feet)

Monocular Drivers • Limited peripheral vision nasally 20 -40 degree deficit • Saccades and head rotation to compensate • Physiological blind spot: 2 metres size at 20 metres distance • Effect diminished by Ocular re-fixation (average 3 times/second) and • Head movements BUT • Small objects may remain unseen for longer • Lack of stereopsis • Uncertain relationship with crash rates • Risk of one eye temporarily losing sight due to FB, watery eye

Are monocular drivers unsafe? • Accidents • Johnson and Keltner: Same crash rates • Closed-course study of driving performance • Woods et al: Driving no worse • Simulator studies • Mc. Knight et al: No significant safety issues • However • Liesmaa: more dangerous behaviour at junctions and while overtaking
 or Two")
Monocular drivers: Formula One (eye) or Two

Case 5 • Patient diagnosed with choroidal melanoma • Right eye enucleated • Left eye: VA: 6/6, Full fields • Patient can read number plate in good light at 20 metres How does this affect driving? Must adapt Inform insurers? Does the patient need to notify DVLA? No need

DVLA requirements for monocular drivers • Visual Acuity Snellen 6/12 • Number plate at 20 metres • Same standard for visual fields • Can drive when ADAPTED to the condition • NO need to notify DVLA

Dilated Pupils • Cycloplegia • Reduced distance VA in high hypermetropes • Spherical Aberrations: • 9 times increased aberration • Glare, dazzle

Study of daytime driving in dilated patients on closed circuit: 1% Tropicamide • Vision measures • Visual Acuity reduced: average 2 letters maximum 1 line • Contrast Sensitivity worse: average 1 letter maximum 4 letters • Glare sensitivity worse: average 4 letters • Driving measures • Significantly worse for: potholes, road debris, speed bumps, pedestrians, other vehicles • No problems with: Road signs, traffic cones, gap perception

Dilated Pupils • Potamitis et al on driving simulator studies: • Reduced High Contrast Visual Acuity • Reduced Contrast Sensitivity BUT Driving not impaired • But remember: they used driving simulator, no glare, young patients, no ocular disease • Likely to be worse in older people, at night, foggy conditions, with cataract/AMD • Insurance Implications?

Electric cycle:

Segway


QUESTIONS?

Fields for class 2 drivers

Action to be taken if patient ignores your advice and continues driving • Explain to patient: • 1. Their eye condition may affect ability to drive • 2. They have a legal duty to inform DVLA • If patient refuses to accept advice: • Suggest second opinion, help to arrange and advise to STOP driving until then • If continues to drive: • Reasonable effort to persuade them to stop • Discuss with relatives/carers/friends with patients permission • If all fails: • Inform patient that you intend to write to DVLA • Inform DVLA confidentially on ‘Doctor Notification’ form • Let patient know you have informed DVLA

AREDS 2

AREDS 2: BACKGROUND AREDS 1 showed 25% reduction in risk of advanced AMD • AREDS 1 formula had • Carotenoid: beta carotene • Anti-oxidants: Vitamins C and E • Minerals: Zinc and copper But: • Concern about risk of beta carotene in smokers • Side effects of zinc at high doses • No lutein, zeaxanthin, omega 3 FA

AREDS 2: OBJECTIVES Effects of high supplemental doses of: • dietary xanthophylls (lutein and zeaxanthin) • and omega -3 fatty acids on • the development of advanced AMD • cataract and • moderate vision loss (the loss of 15 or more letters). Effects on the development and progression of AMD of: • eliminating beta-carotene in the original AREDS formulation • reducing zinc in the original AREDS formulation

AREDS 2: RESULTS Omega 3 Fatty Acids No benefit over AREDS original

AREDS 2: RESULTS Lutein and Zeaxanthin No benefit over AREDS original But: • If beta-carotene removed and replaced with Lutein + Zeaxanthin • Further 18% risk reduction Also: • If low dietary Lutein and Zeaxanthin • 25% risk reduction with supplement

AREDS 2: RESULTS Beta-Carotene • Removing beta-carotene did not compromise efficacy of formula • Better without beta-carotene if Lutein and Zeaxanthin added • Increased risk of lung cancer even in FORMER smokers

AREDS 2: RESULTS Zinc • Reducing zinc did not compromise efficacy of formula • But no certainty about what is the best dose

AREDS 2: Implications for clinical practice • Drop beta-carotene • Add Lutein and Zeaxanthin • No need for omega 3 • Reduce zinc to 25 mg • Keep the rest as before Same formulation for all (smokers included)

Vitamin C: 500 mg Vitamin E: 400 IU Lutein: 10 mg Zeaxanthin: 2 mg Zinc: 25 mg Copper: 2 mg

Serous PED: CSR

Serous PED: AMD

Vitelliform

Haemorrhagic PED
- Slides: 117