Understanding and Working with Hoarding Disorder Helping the










 n Obsessive Compulsive Disorder n")


































- Slides: 48
+ Understanding and Working with Hoarding Disorder: Helping the Person Behind the Diagnosis Eileen Dacey, LCSW North Shore Center for Hoarding and Cluttering North Shore Elder Services edacey@nselder. org
Agenda n Diagnostic features and variables that maintain hoarding disorder: Defining various terms n Hoarding disorder vs. hoarding behavior n Motivation to Change n Harm Reduction n Assessment Tools n Q&A
What is hoarding?
We cannot effectively resolve what we do not fundamentally understand.
+ Object Hoarding
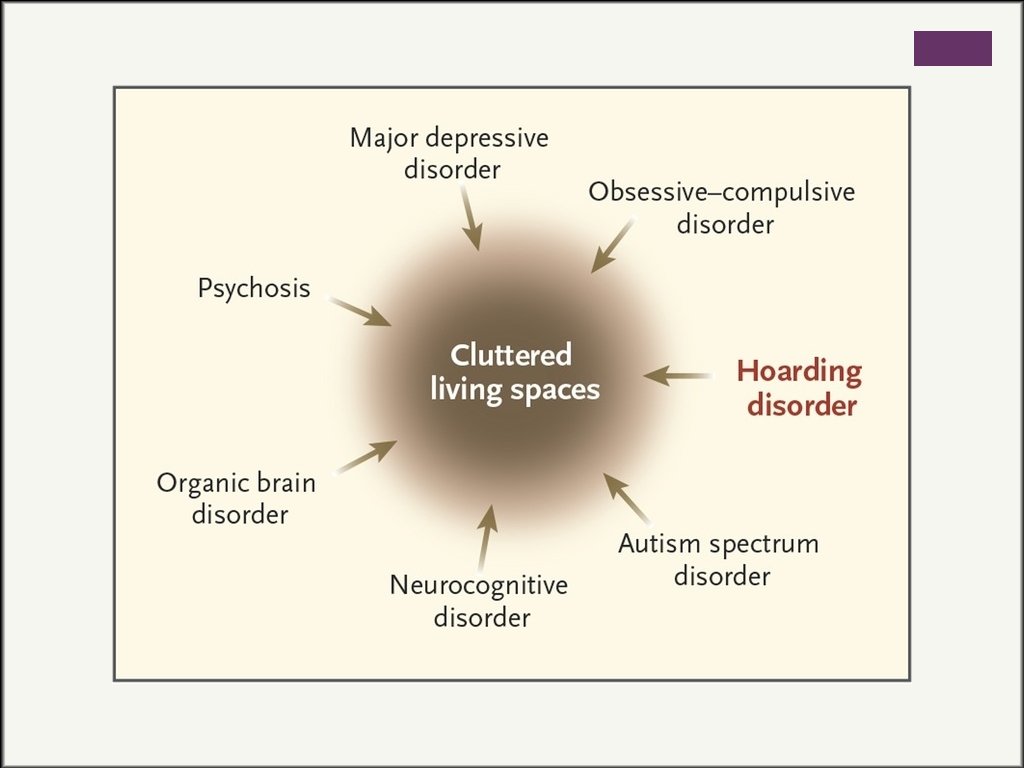
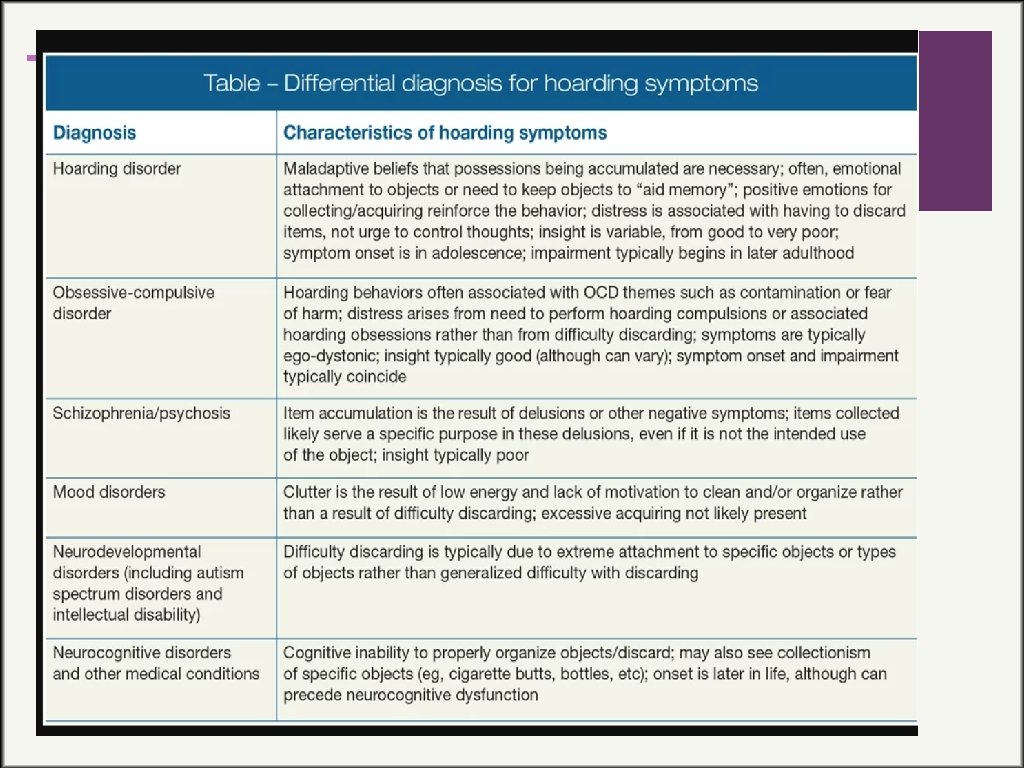
DSM-5 Diagnostic Criteria A. Persistent difficulty discarding or parting with personal possessions, even those of apparently useless or limited value, due to strong urges to save items, distress, and/or indecision associated with discarding. B. The symptoms result in the accumulation of a large number of possessions that fill up and clutter the active living areas of the home, workplace, or other personal surroundings (e. g. , office, vehicle, yard) and prevent normal use of the space. If all living areas are uncluttered, it is only because of others’ efforts (e. g. , family members, authorities) to keep these areas free of possessions. C. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning (including maintaining a safe environment for self and others). D. The hoarding symptoms are not due to a general medical condition (e. g. , brain injury, cerebrovascular disease). E. The hoarding symptoms are not restricted to the symptoms of another mental disorder (e. g. , hoarding due to obsessions in Obsessive-Compulsive Disorder, lack of motivation in Major Depressive Disorder, delusions in Schizophrenia or another Psychotic Disorder, cognitive deficits in Dementia, restricted interests in Autistic Disorder, food storing in Prader-Willi Syndrome).
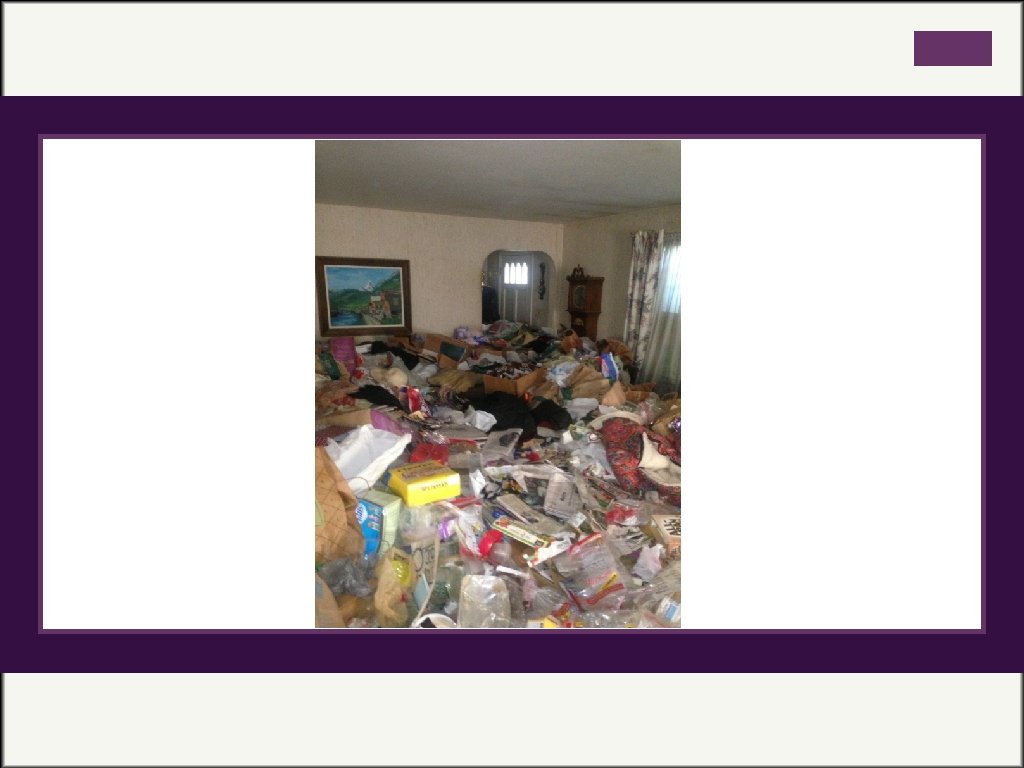
+ Understanding the symptoms of hoarding disorder § Difficulty Discarding: Reluctance to discard personal possessions, including objects that might be considered worthless or have little intrinsic value. Beliefs for saving items are more intense and rigid, and applied to a greater number of possessions. Attempts to discard usually cause substantial emotional distress. § Excessive Clutter: Most visible component of hoarding. Can create significant difficulty using living spaces. Clutter can cover beds, chairs, tables—rendering them unusable. In severe cases can prohibit movement throughout the house. § Excessive Acquiring: Compulsive buying, collection of free items, rummaging through trash bins, and inheritance. Distress related to overspending/debt. (Tolin, Wooton, Worden, Gilliam, 2017)
Specifiers of Insight Specify if: Good or fair insight: The individual recognizes that hoardingrelated beliefs and behaviors are problematic. n Poor insight: The individual is mostly convinced that hoarding-related beliefs and behaviors are not problematic despite evidence to the contrary. n Absent insight: (i. e. delusional beliefs about hoarding): The individual is completely convinced that hoarding-related beliefs and behaviors are not problematic despite evidence to the contrary. n Excessive Acquisition: n Excessively collecting, buying, or stealing items that are not needed or for which there is no available space n ~80 -90% n Stealing is less common ~10 -15% n Active vs. passive acquisition n n
Onset, Prevalence, and Course n Affects approximately 3 -6 % of the population n Roughly 1 out of every 20 people n Scholars believe this is an underrepresented amount of actual percentage n Chronic and progressive course n Hoarding behavior emerges in childhood or early adolescence n Does not meet full criteria until late in life because diagnosis linked to cluttered living spaces. n Most hoarded items and prevalent careers (Tompkins, 2018)
Other Factors and FAQs n Genetic Factors and Learned Behaviors n No link to material deprivation n Hoarding Behaviors triggered by traumatic life events n Higher IQ levels, Education, and Creativity n Perfectionism (cognitive distortions) n Average Age of Treatment seekers ~55 years of age n More Men than Women (Tompkins, 2018)
Common Co-Morbid Disorders n Major Depressive Disorder (over 53%) n Obsessive Compulsive Disorder n Attention Deficit Hyperactivity Disorder n Generalized Anxiety Co-morbid disorders & hoarding 60% Hoarding Frequency 50% 40% 30% 20% 10% 0% ADHD OCD MDD Anxiety (Frost, Steketee, & Tolin 2011)
What are hoarding behaviors? Acquisitio n Excessive Saving Difficulty Discardin g Hoarding Behaviors
Cognitive-Behavioral Model of Hoarding Disorder Beliefs and Attachments to Possessions Vulnerabilities Hoarding Disorder Information Processing Deficits Emotional Reactions
Cognitive-Behavioral Model of Hoarding Disorder Continued n Information Processing n Perception, Attention Span, Memory n Categorization, Decision Making Deficits n Vulnerabilities n Trauma n Beliefs/Attachments n Beliefs about Possessions n Sentimental, intrinsic, instrumental n Beliefs about Vulnerability n Maladaptive thoughts n Beliefs about Responsibility-waste n Beliefs about Memory and Control n Emotional Reactions n Positive and Negative Emotions Clutter Saving Difficulty Acquisition Discarding All Contribute to hoarding behaviors
Information Processing: Notion of Underinclusivity
Anthropomorphizing n Attributing human-like qualities/personalities to inanimate objects n The desire to hold onto an object because no one else will give the item a better home n “If I let go of this item, the item would be sad. ” n Another possible mechanism contributing to emotional attachments n High desires for control, need for social contact n “I want the item to go to a good home” n Emotional attachments-objects associated with fond memories (Timpano & Shaw, 2013) (Neave, Jackson, Saxton, & Honekopp, 2015)
Hoarding Behaviors n Hoarding Disorder as a disorder of behavior n Reward and Relief Model: n Behaviors are reinforced by both reward (positive reinforcement) and relief (negative reinforcement) factors n Example: Acquisition is exciting, makes me feel good, purchased something new (reward). The purchase relieved anxiety and calmed me down (relief). Clutter Saving Difficulty Discarding Acquisition Animal Hoarding
Emotional Highs and Lows Need to selfsoothe Discomfort Feels Guilt/Shame Prompts Acquisition Experiences Relief/High n Emotional Reactions towards discarding as sadness, grief, anxiety
Hoarding Behaviors n Internal Influences of the behavior n Level of insight and co-occurring illnesses n Stress and pressures n Processing deficits and other vulnerabilities n History of Trauma n Motivation n Environmental Influences on Behavior n Social Supports n Conditioned Cues (Environmental and Internal Contexts can elicit impulsive behaviors when faced with discomfort—coping)
+ n Poor Emotion Regulation Can show: A. Lack of awareness, understanding, and acceptance of emotions B. Lack of access to adaptive strategies for modulating the intensity and/or duration of emotional responses C. An unwillingness to experience emotional distress as part of pursuing desired goals D. The inability to engage in goal-directed behaviors when experiencing distress n All highly common in hoarding disorder (Tolin, Wooton, Worden, Gilliam, 2017)
Habituation Curve
+ What about motivation? n Think of a behavior you tried to change n Success? n What about the first you recognized the negative consequences from the behavior? n Behavior change takes time n Motivation to change varies n Relapse is common and must be normalized n Motivation and compliance are not the same (Tolin, Wooton, Worden, & Gilliam, 2017)
Motivational Enhancement Change Stay the Same
What about Motivation?
+ Focus on Internal Motivation n n What make people motivated to change? n Confidence n Level of importance Factors influencing motivation n Social Supports n Co-morbid disorders n Ability to tolerate discomfort
Challenging Questions Enhancing Insight n How many do you already have? Is that enough? n Do you have enough time to use, review, or read it? n Have you used this during the past year? n Do you have a specific plan for this item? By when? What is the likelihood that you will use this item again? n Does this fit with your values and needs? Is it important because you’re looking at it now? n Is it current, of good quality, accurate, reliable? n Would you buy it again if you didn’t already own it? n Do you really need it? Could you get it again if you really needed it? Do you have enough space for this?
Sorting Practice Exercise n Empty your purse or wallet n Place contents in front of you n Divide items into three categories: n n Impossible to let go of n Moderately impossible to let go of n Minimal difficulty letting go How did you formulate your decisions? What rules did you create? What did you notice about yourself during the process? (Sorting exercise developed by Dr. Michael Tompkins, 2018)
Guidelines for Initial Assessment n Provide Rationale for Home Visit. n Do not touch anything without EXPLICIT permission. n Each decision must be the client’s decision. Can be guided by therapist, not decided by therapist. n Try to keep the home visit as short as possible. n Decide where to begin treatment. n Photograph all rooms of the home. n Use assessment tools. n Involve family members who live in the home. (Tompkins, 2018)
Guidelines for Treatment Imagine yourself in the client’ s position Model positive, adaptive behaviors Provide encouragement and emotional support DON’T Do Any of the Following: Use judgmental language Touch belongings without explicit permission Share your opinions when asked, emphasizing transparency Declutter behind the client’ s back, or say you will donate something and throw it away instead Believe in the client’ s ability Minimize the challenges faced Highlight strengths, always provide positive. Make decisions validation Equate the clutter with the person Stay calm… even when it is tough Argue or try to persuade Take care of yourself (Bell, 2012)
+ What about now? We have a crisis on our hands!
Harm Reduction n. Works to minimize risks without changing behavior entirely n. Objective stance vs. subjective approaches n. Less confrontation n. Involves the person from the start n. Creates a universal approach despite vast differences in hoarding cases n. Think about insight n. Comprehensive, interdisciplinary, & focus on safety of the person and well-being of animals (Thompkins, 2015)
Clutter’s Interference with Basic Functioning n Cooking n Cleaning n Moving throughout the home n Sleeping n Strong likelihood of: Fire n Fall Risks n Poor Sanitation n Pest Infestation n Risk to those who live in the home and neighbors n Hoarding accounts for 24% of preventable fire fatalities n Skin wounds n High concentrations of ammonia n Contaminate food and water supply n Animal behavior n Spread of zoonotic diseases n Air quality n (Thompkins, 2015) (Tolin, Worden, Wootton, & Gilliam, 2017)
Application of Harm Reduction for Hoarding § § § § Involve the individual from the very beginning of the process Identify objective and specific safety risks Develop objective plan to reduce risks Do not focus on eliminating risk Avoid subjective, personal value-based, goals Remember self-determination! Harm reduction approach assumes that the client can and will make his or her own decisions, fosters relatedness through empathy, mutual respect, and understanding, and enhances competence through realistic goal setting. § Motivation enhanced through a trusting, supportive relationship.
+ When to make a mandated report Ø Mandated reporters must report when they observed or suspect abuse or evidence of neglect Ø Many people who hoard are not accurate reporters to the degree and extent of their hoarding problem Ø First, visit the residence Ø Focus on imminent risk Ø Ø Presence of animal/human excrement (sensory blunting) Consuming spoiled foods Significant structural damage Discuss the report with the resident
+ L. E. A. R. N. to Clear Targets • Listen – to client’s ideas and plans for belongings; explore client’s solutions to the problem, both realistic and unrealistic, and accommodate client if possible. • Empathize – let client know you have similar feelings about possessions and sometimes it is difficult for you to part with them too. • Affirm – let client know you understand how attached they are to their belongings and how much the possessions mean to them. • Redirect –client back to harm reduction target and agreement, be gentle but clear. • Negotiate – be creative and negotiate, generally around adherence to the harm reduction contract. (Tompkins, 2016)
Assessment Tools Clutter Image Rating Assessing ‘volume’ http: //www. ocfoundation. org/hoarding/cir. pdf H. O. M. E. S. – Multi-disciplinary Hoarding Risk Assessment Assessing risk http: //www. masshousing. com/hoarding Uniform Inspection Checklist – Hoarding / Excessive Clutter Minimum safety and sanitation standards http: //www. masshousing. com/hoarding
Clutter Image Rating
Uniform Inspection Checklist
So…what about clean-outs? n Just eliminate the problem and throw everything out! n Why can’t you just make someone throw stuff away? n DOES NOT SOLVE THE PROBLEM n They are NOT sustainable and NOT effective n They yield the highest rate of recidivism n Creates psychological impact on the resident and can be traumatizing for the client. n Once hoarding cases gain public attention, they are likely: n Severe and require intensive, lengthy, costly, and strategic planning/responses n They are emotionally taxing to the homeowner, community and resident n Yield enormous public health implications
+ Harm Reduction Video n Harm Reduction Video
ENGAGEMENT AND MOTIVATION 1. If you woke up tomorrow and your home was just the way you want it to be, how would your life be different? 2. What is something you want to do that you currently are not doing or cannot do because of the clutter in your home? Taking a strengths-based approach
Redefining our Perception of Success n. Have we minimized the risks? n. Is it safe and functional for the resident? n. Is the client aware of the risks?
Resources http: //vet. tufts. edu/hoarding/ http: //nselder. org/north-shore-center-for-hoardingdecluttering/ https: //www. aspca. org/ http: //massanimalcoalition. org/ https: //www. arlboston. org/ https: //www. facebook. com/groups/Hoarding. Task. Force. Network www. masshousing. com/hoarding www. ocdfoundation. org http: //www. mutual-support. com/ https: //www. facebook. com/groups/The. Clutter. Movement. Indivi dual. Support https: //www. facebook. com/groups/The. Clutter. Movement. Famil y. Support/ http: //thehoardingproject. org/home/