RICKETS Rickets Definition Failure of mineralisation of the





 Intestine ----- Calcitriol promotes absorption of calcium and")
ossification at epiphysis")


 Rickets refractory to vitamin D treatment may")
 2 -X-linked Dominant type 3")
 Definition the bone disorders seen in children with")




 --the sternum and adjacent")





 Bowleg deformity (genu varum)")




 A line of preparatory calcification")

 Healing after 28")






- Slides: 40
RICKETS
Rickets Definition - Failure of mineralisation of the growing bones - Disease of the growing child - Rickets is a childhood disorder involving softening and weakening of the bones. - It is primarily caused by lack of vitamin D, calcium and phosphate.
Sources of Vitamin D q Sunlight is the most important source q Fish liver oil q Fish & sea food q Eggs q Plants do not contain vitamin D 3
Vitamin D is a fat-soluble vitamin that may be absorbed from the intestines or may be produced by the skin when the skin is exposed to sunlight (ultraviolet light of sunlight helps the body to form vitamin D). The absorbed vitamin D is converted into its active form to act as a hormone to regulate calcium absorption from the intestine and to regulate levels of calcium and phosphate in the bones.
Path way of Vi tami n. DP rodu ction
Vitamin D Calcitriol (1, 25 -DHC) Intestine ----- Calcitriol promotes absorption of calcium and phosphorus Kidney ------ Increases reabsorption of calcium and phosphate Bones ----- Mineralisation of the bone matrix In rickets, another mechanism in the body works to increase the blood calcium level. The parathyroid gland may increase its functioning rate to compensate for decreased levels of calcium in the blood (increase secretion of PTH) PTH----- increase bone resorption to maintain normal ca level and increase weakness of bones
Physiology of normal bone formation There 2 types of ossification 1 -Endochondrial(intracartilagenous)ossification at epiphysis --- responsible for increase in bone length 2 -Subperiosteal ossification ---- responsible for increase in bone thickness Ossification start from epiphysis toward diaphysis 1 -Resting cartilage 2 -proliferating cartilage 3 -provisional calcification 4 -New bone formation
Etiology of Rickets 1 - Vitamin D deficiency rickets 1 - Lack of vitamin D intake(infantile or nutritional rickets) 2 - Lack of sun light exposure 3 - Defective absorption— malabsorption 4 - Hepatic disease --- defective hydroxylation 5 - Anticonvulsants (phenytoin, phenobarbital)
2 - Vitamin D dependent 1 - Vitamin D-dependent rickets type I is secondary to a defect in the gene that codes for the production of renal 25(OH)D 3 -1 -alphahydroxylase(defective of renal hydroxylation) 2 - Vitamin D-dependent rickets type II is a rare autosomal disorder caused by mutations in the vitamin D receptor. Type II does not respond to vitamin D treatment; elevated levels of circulating calcitriol differentiate this type from type I. (End organ resistance)
3 - Vitamin D resistant (Hypophosphataemic rickets) Rickets refractory to vitamin D treatment may be caused by the most common heritable form, known as vitamin D-resistant rickets or familial hypophosphatemic rickets. Because of mutations of the phosphate-regulating gene on the X chromosome, renal wasting of phosphorus at the proximal tubule level results in hypophosphatemia. Normal levels of calcitriol are found in this disorder.
Hypophosphataemic rickets 1 -Familial hypophosphataemic rickets(vitamin D resistant rickets) 2 -X-linked Dominant type 3 - Autosomal Dominant type 4 - Autosomal Recessive Type 1 5 - Autosomal Recessive Type 2 6 - Associated with increase phosphatonin (a) Mc. Cune-Albright syndrome (b) Tumour induced osteomalacia (c) Linear nevus sebaceous syndrome
4 - Renal osteodystrophy (Renal rickets) Definition the bone disorders seen in children with chronic kidney disease (CKD) 1 - Decreased 25, 1 alpha hydroxylase --- decrease 1, 25 (OH) D 3 ---- decrease Ca absorption from GIT 2 - Hyperparathyroidism due to hypocalcaemia --PTH---increase bone resroption to correct hypocalcaemia 3 - In CKD --- decrease phosphate excretion --hyperphosatemia which promote hypocalcaemia(to maintain Ca /P ratio normal )
Clinical picture of Renal rickets 1 - Growth failure due to CKD 2 - Muscle weakness , bone pain and bone deformities 3 - Tetany due to hypocalcaemia 1 nvestigations 1 - Hypocalcaemia or normocalcemia 2 - Hyperphosphatemia 3 - Hyperphosphatesia 4 - PTH --- elevated 5 - X ray ---- signs of rickets
Treatment of Renal Rickets 1 - Diet restriction of phosphate 2 - Oral administration of phosphate binders as calcium carbonate 3 - Vit D 4 - Treatment of CKD
Clinical Manifestation A- Early rickets Age ; most common 6 months to 2 years 1 -Vague manifestation — irritability, profuse sweating over head 2 -Craniotabes — it is caused by thinning of the outer table of the skull -- pressing over the posterior part of the parietal bone produce ping-pong sensation 3 -Rachitic rosary along the costochondral junctions("Bumps" in the rib cage )
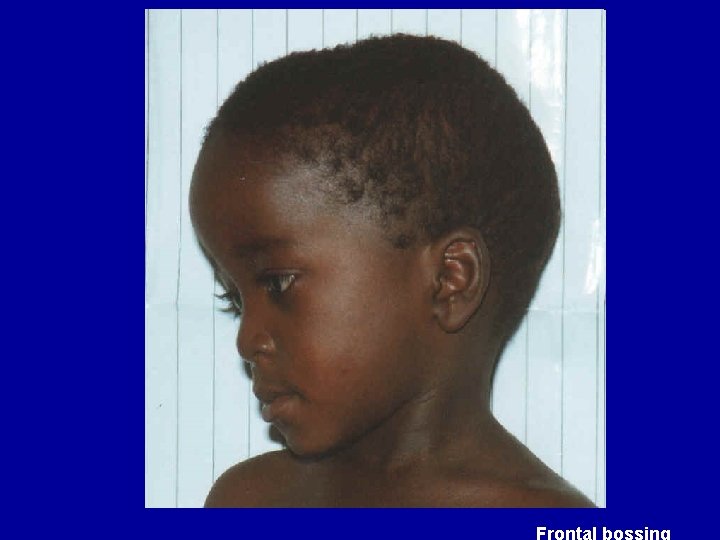
Clinical Manifestation B-Advanced rickets A- head 1 - Craniotabes and delayed formation of teeth 2 - Delays the closure of the anterior fontanelle 3 - Bossing of skull due to osteoid deposition in centre of parietal and frontal bones give the picture of boxy skull(Caput quadratum) B-thorax 1 - Rachitic rosary along the costochondral junctions 2 - Harrison sulcus; horizontal groove at the lower part of the chest which dragged in during inspiration
Clinical Manifestation 3 - Pigeon chest or (Pectus Carinatum ) --the sternum and adjacent parts project forward 4 - Funnel chest (Pectus Excavatum) --depression of the lower end of sternum Consequence of chest deformity 1 - limited chest expansion --- recurrent chest infection 2 - Downward displacement of the liver and spleen
Clinical Manifestation C- Hypotonia and relaxed ligaments 1 - Delayed sitting , standing and walking 2 - Kyphosis — appearance while sitting , smooth and not angular and corrected by holding the child from shoulders 3 - Protruding abdomen (potbelly) due to hypotonia of abdominal wall muscles
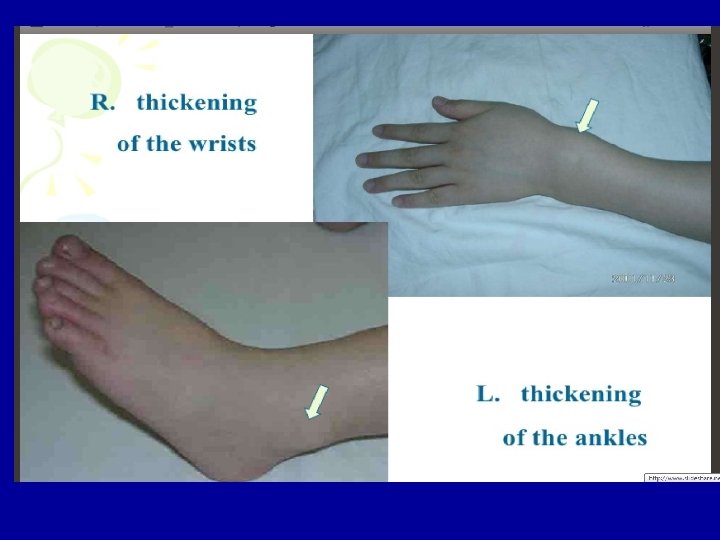
Clinical Manifestation D- Extremities 1 - Widening of the wrist and ankle due to expansion and cupping of growing ends of long bones 2 - Marfan sign ; transverse groove over medial malleolus due to defective osteoid deposition 3 - Deformities from weight bearing at the shaft of the bones A- Crawling ; deformities of humerus , radius and ulna B- Walking; bow legs and knock knees
Complication of rickets 1 - Repeated chest infection 2 - Hypocalcaemia --- tetany , seizures and stridor 3 - Bone fracture and deformities 4 - Iron deficiency anemia
Pigeon chest Chest deformity Funnel chest – pectus excavatum
Clinical signs Bowlegs and knock-knees.
Knock knee deformity (genu valgum) Bowleg deformity (genu varum)
Vitamin D Deficiency - Rickets
Pelvic deformities Bowlegs and knock-knees
Laboratory findings Laboratory investigation may include: Serum calcium---normal or low in sever cases Serum phosphorus---reduced <4 mg/dl Serum alkaline phosphatase (ALP)--increased >500 IU
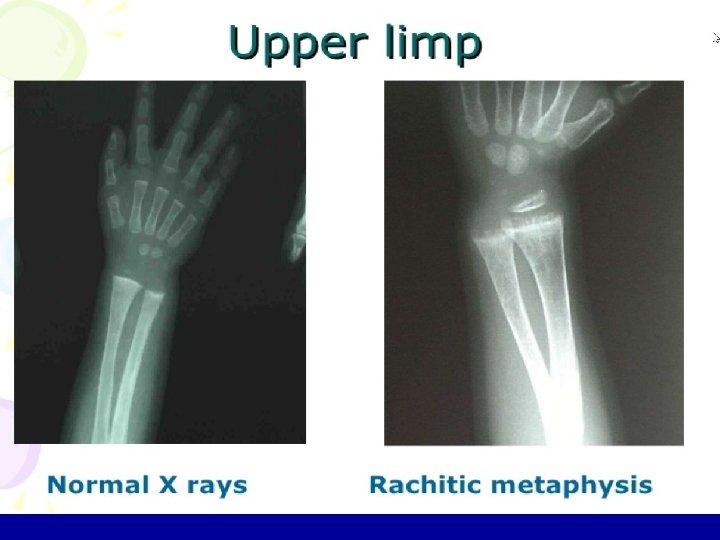
Radiological changes These are best seen at the lower end of the radius and ulna A-Active rickets 1 -Distal ends are widened, cupped or concave and frayed and ill defined 2 -Wrist joint space ---is wide 3 -Rarefaction--- decrease bone density 4 - Green stick fracture and deformities
Radiological changes B- Healing rickets(2 -3 weeks after treatment) A line of preparatory calcification appear which is separate from the distal end of the shaft C- Healed rickets(6 -8 weeks after treatment) There is thickening and slight irregularity of the lower end of the radius
Rickets in wrist - uncalcified lower ends of bones A (B) Healing after 28 days of treatment B C (C) After 41 days of treatment
Classic radiographic findings include Anteroposterior and lateral radiographs of the wrist of an 8 -yearold boy with rickets demonstrates cupping and fraying of the metaphyseal region
Radiographic image of wrist and forearm showing pathologic fractures of radius and ulna with rachitic changes of distal end of radius and ulna.
X-ray in rickets
Prevention of rickets Because of breast milk contains only a small amount of vitamin D, recommends that all breast-fed infants receive 400 IU of oral vitamin D daily beginning during the first two months of life Vitamin D supplementation: In prematures, twins and weak babies, give Vitamin D 800 IU per day, For term babies and infants the demand of Vitamin D is 400 IU per day
Treatment of rickets Vitamin D therapy A- General method: Vitamin D 1500 -5000 IU/day for 6 -8 weeks, then change to preventive dosage – 400 IU. B- A Single large dose: For severe case, , or those who can’t tolerate oral therapy 200, 000 IU given once orally or IM second dose after one month interval Calcium supplementation Plastic therapy: In children with bone deformities after 4 years plastic surgery may be useful.
TOXICITY • Hypervitaminosis D causes hypercalcemia, which manifest as: üNausea & vomiting and constipation üExcessive thirst & polyuria üSevere itching üJoint & muscle pains üDisorientation & coma. üTreatment by discontinuation of vit D and