IN THE NAME OF GOD HEART FAILURE Definition


 is a complex clinical syndrome resulting from structural and")






")





 is common in")














- Slides: 41
IN THE NAME OF GOD
HEART FAILURE Definition and types A. Soleimani MD Assistant professor of cardiology Medical university of Isfahan
HF definition �Heart failure (HF) is a complex clinical syndrome resulting from structural and functional impairment of ventricular filling or ejection of blood �Most patients have impairment of myocardial performance, with findings ranging from normal ventricular size and function to marked dilation and reduced function. �Although symptoms of HF frequently depend on the presence of elevated left- or right-sided heart filling pressures, the designation “congestive” in this context is no longer preferred
Stages, Phenotypes and Treatment of HF
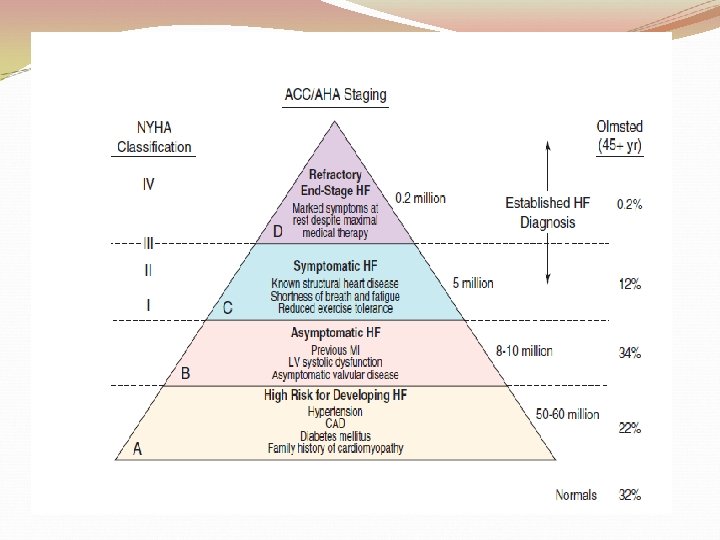
Classification of Heart Failure A B C ACCF/AHA Stages of HF At high risk for HF but without structural heart disease or symptoms of HF. Structural heart disease but without signs or symptoms of HF. Structural heart disease with prior or current symptoms of HF. None I I II IV D Refractory HF requiring specialized interventions. NYHA Functional Classification No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF. Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF. Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
Definition of Heart Failure Classification Ejection Fraction Description I. Heart Failure with ≤ 40% Reduced Ejection Fraction (HFr. EF) Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFr. EF and it is only in these patients that efficacious therapies have been demonstrated to date. II. Heart Failure with Preserved Ejection Fraction (HFp. EF) ≥ 50% Also referred to as diastolic HF. Several different criteria have been used to further define HFp. EF. The diagnosis of HFp. EF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. a. HFp. EF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFp. EF. b. HFp. EF, Improved >40% It has been recognized that a subset of patients with HFp. EF previously had HFr. EF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients.
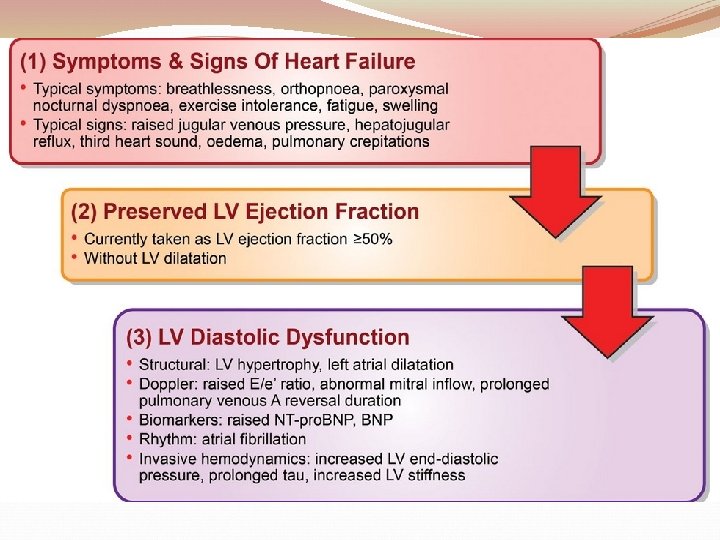
HFp. EF �Approximately half of the patients with HF have normal left ventricular function, that is, HF with preserved ejection fraction (HFp. E) �HFp. EF generally is defined as a left ventricular ejection fraction of 50% or greater, whereas HFr. EF is defined as an ejection fraction below 40%.
Dyspnea �Worsening dyspnea is a cardinal symptom of HF and typically is related to increases in cardiac filling pressures but also may represent restricted cardiac output. �The absence of worsening dyspnea, however, does not necessarily exclude the diagnosis of HF, because patients may accommodate symptoms by substantially modifying their lifestyle.
Dyspnea �Patients may sleep with the head elevated to relieve dyspnea while recumbent (orthopnea) �Paroxysmal nocturnal dyspnea, shortness of breath developing in recumbency, is one of the most highly reliable indicators of HF. �Nocturnal cough is a frequently overlooked symptom of HF. �These symptoms all typically reflect pulmonary congestion
Congestion history of weight gain, increasing abdominal girth, early satiety, and the onset of edema in dependent organs (extremities or scrotum) indicate right heart congestion Nonspecific, right upper quadrant pain due to congestion of the liver is common in those with significant right-sided HF and may be incorrectly attributed to other conditions
Fatigue �Another cardinal symptom of HF is fatigue, generally held to be reflective of reduction in cardiac output as well as abnormal skeletal muscle metabolic responses to exercise. � Other causes of fatigue in HF may include major depression, anemia, renal dysfunction, and endocrinologic abnormalities, as well as side effects of medications. � Cachexia may be prominent and lead to an extensive workup for malignancy
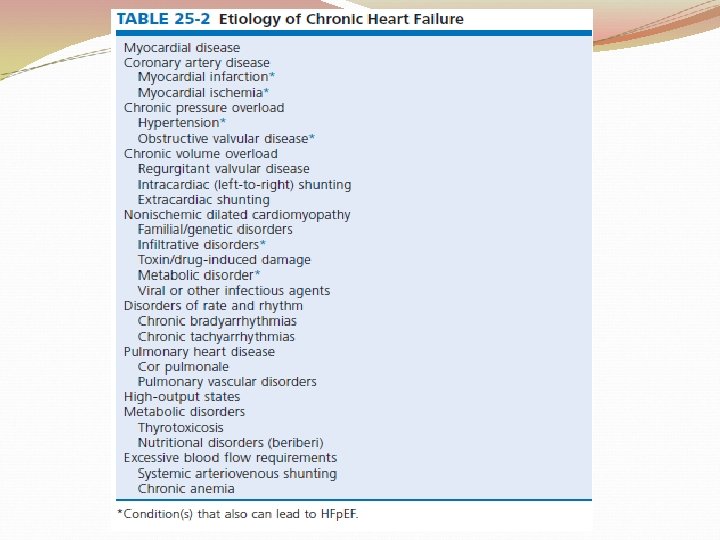
History �The presence of hypertension, coronary artery disease and/or diabetes is particularly helpful since these conditions account for approximately 90% of the population attributable risk for HF in the United States. � The medical history should also focus on what drugs are taken by the patient; agents associated with incident HF include cancer chemotherapy, diabetes drugs (e. g. , thiazolidinediones), ergot-based antimigraine drugs, appetite suppressants, certain antidepressants and antipsychotic agents (notably including clozapine), decongestants such as pseudoephedrine (owing to its ability to trigger severe hypertension), and antiinflammatory agents such as the antimalarial drug hydroxychloroquine and NSAIDs.
History �A history of use of herbal remedies and dietary supplements should be obtained. �Environmental or toxic exposures including alcohol or drug abuse should be carefully sought. �A multigenerational family history should be taken for previous HF or sudden cardiac death. �Although most disorders causing HF are cardiac, it is worth remembering that some systemic illnesses (e. g. , anemia, hyperthyroidism) can cause this syndrome without direct cardiac involvement
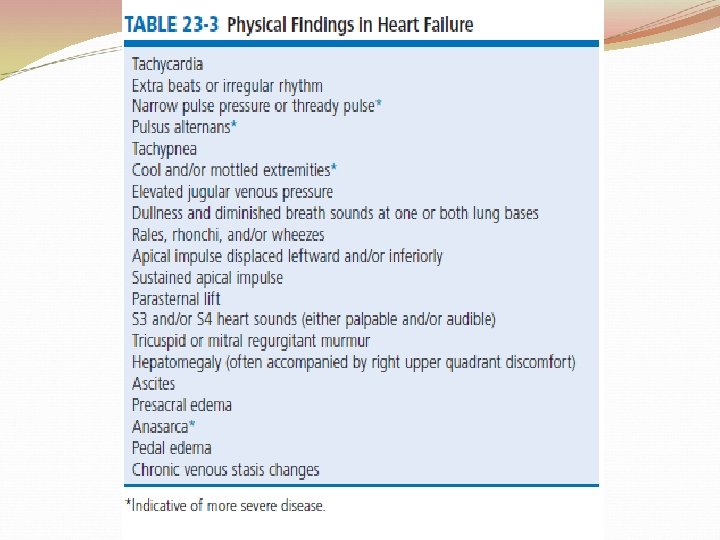
P/E �An evaluation for the presence and severity of HF should include consideration of the patient’s general appearance, measurement of vital signs in the seated and standing positions, examination of the heart and pulses, and assessment of other organs for evidence of congestion or hypoperfusion or indications of comorbid conditions.
P/E �Cheyne-Stokes respiration (also referred to as periodic or cyclic respiration) is common in advanced HF and usually is associated with low cardiac output and sleep -disordered breathing : adverse prognosis. � By observing or palpating the apical impulse, the examiner can rapidly determine heart size and quality of the point of maximal impulse. In cases of severe HF, a palpable third heard sound may be present. Cardiac auscultation is a crucial part of HF evaluation. �A characteristic holosystolic murmur of mitral insufficiency is heard in many patients with HF. Tricuspid insufficiency, also is common
P/E �The presence of a third heart sound is a crucially important finding and suggests increased ventricular filling volume; although difficult to identify, a third heart sound is highly specific for HF and carries a substantial prognostic meaning. �A fourth heart side usually indicates ventricular stiffening. �In advanced HF, the third and fourth heart sounds may be superimposed, resulting in a summation gallop.
P/E �A key objective of the examination in patients with HF is to detect and quantify the presence of volume retention, with or without pulmonary and/or systemic congestion. As with symptoms, evidence of congestion does not always indicate with certainty that HF is present, nor does absence of manifest congestion definitively exclude the diagnosis. � Patients with HFp. EF and those with HFr. EF do not generally show significant differences in frequency or significance of the stigmata of volume overload.
P/E �The most definitive method for assessing a patient’s volume status by physical examination is by the measurement of jugular venous pressure (JVP). � An elevated JVP has good sensitivity (70%) and specificity (79%) for elevated left-sided filling pressure. � The sensitivity and specificity of the JVP in detecting congestion can be considerably improved by exerting pressure on the right upper quadrant of the abdomen while assessing venous pulsations in the neck (hepatojugular reflux). �Changes in JVP with therapy usually parallel changes in left-sided filling pressure.
P/E � Limitations of JVP assessment include difficulties in its evaluation due to body habitus as well as significant interobserver variability in its estimation. � Increase in the JVP may lag behind left sided heart filling pressures or may not rise at all if pulmonary artery pressure is increased to the extent that right ventricular failure or tricuspid insufficiency occur. � Conversely, the JVP may be elevated without an increase in left ventricular filling pressures in patients with pulmonary arterial hypertension, in those with isolated right ventricular pressure, or when isolated severe tricuspid regurgitation is present.
P/E �Bilateral pleural effusions are most common but when an effusion is present unilaterally, it is usually right sided �only approximately 10% occurring exclusively on the left side.
P/E �Leakage of fluid from pulmonary capillaries into the alveoli can be manifested as rales or rhonchi, and wheezing may occur with reactive bronchoconstriction. �Pulmonary rales due to HF usually are fine in nature and extend from the base upwards, whereas those due to other causes (e. g. , pulmonary fibrosis) tend to be coarser. Rales or rhonchi may be absent in congested patients with advanced HF; this may reflect compensatory increase in local lymphatic drainage. �Cardiac asthma is due to the physical presence of fluid in the bronchial wall, as well as secondary bronchospasm, and can commonly result in an incorrect diagnosis of obstructive airways disease exacerbation, with consequent mistriage and incorrect therapy with bronchodilators and increased risk of death.
P/E �Lower-extremity edema is a common finding in volume-overloaded patients with HF but may commonly be the result of venous insufficiency (particularly after saphenous veins have been harvested for coronary artery bypass grafts) or as a side effect of medications (e. g. , calcium channel blockers). �Careful inspection of the JVP will help improve the specificity of pedal edema for HF.
P/E �Detection of reduced cardiac output and systemic hypoperfusion is a key component of the examination. �Although patients with poor systemic perfusion usually have low systolic and narrow pulse pressures as well as weak and thready pulses, this relationship is not exact �Many patients with systolic blood pressures in the range of 80 mm Hg (or even lower) may have adequate perfusion, whereas others with reduced cardiac output may maintain blood pressure in the normal range at the expense of tissue perfusion by greatly increasing systemic vascular resistance.
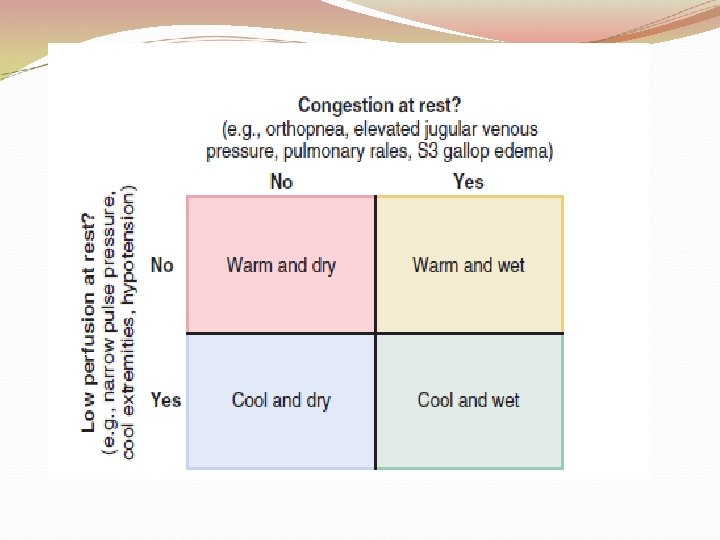
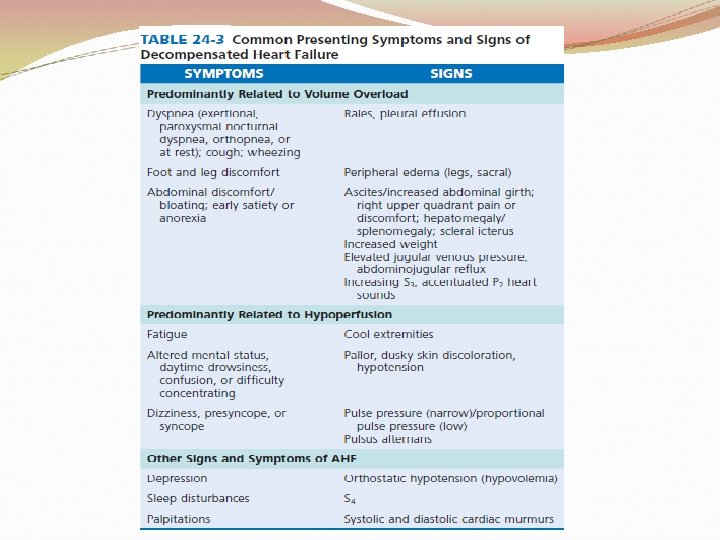
P/E �Findings suggesting reduced cardiac output include poor mentation, reduced urine output, mottled skin, and cool extremities. Of these, cool extremities are the most broadly useful. �Assessment for systemic congestion, taken together with evaluation for reduced cardiac output, may be useful to separate patients with HF into 4 categories: �“dry/warm” (uncongested with normal perfusion) �“wet/warm”(congested with normal perfusion): most common in DHF �“dry/cold”(uncongested but hypoperfused) �“wet/cold” (cardiogenic shock)
ACUTE HEART FAILURE
Acute HF