Normal and Abnormal Myocardial Function Cellular Basis of

Normal and Abnormal Myocardial Function Cellular Basis of Cardiac Contraction A. Cardiac Ultrastructure Contractile Process / Cardiac Activation B. Myocardial Mechanics and Cardiac Function Role of Muscle Length / The Force-Velocity Curve Ventricular Ejection Assessment of Cardiac Function Diastolic Function C. Control of Cardiac Performance and Output: Introduction Ventricular End-Diastolic Volume (Preload) Myocardial Contractility Ventricular Afterload Exercise D. The Failing Heart: Introduction Mechanisms of Heart Failure Neurohumoral and Cytokine Adjustments Heart Failure—A Disturbance of the Myocardial Pump

A. Cellular Basis of Cardiac Contraction A 1. Cardiac Ultrastructure Myocardium:striated muscle cell fiber cross-banded strands (myofibrils) sarcomere Sarcomere: structural and functional unit of contraction Primary contractile protein Myosin (thick filement): fibrous protein with cross-bridges globular head (ATPase) Actin (thin filament) double helix of 2 chains of actin combine reversibly with myosin in presence of ATP and Mg. Titin resists excess. shortening / elongation of sarcomere

Primary contractile protein major molecules of contractile system. thin actin filament interacts with myosin head Regulatory protein : troponins (Tn) and tropomyosin in actin troponin C (Tn. C) : Ca 2+ binding sites troponin I (Tn. I) : inhibits actin-myosin interaction troponin T (Tn. T)

A 2. Contractile Process : excitation-contraction coupling cross-bridge cycling : Hydrolysis of myosin-ATP by ATPase on myosin head 1 4 2 3 1. relaxed muscle : low cytosolic Ca 2+ tropomyosin 과 Tn- complex에 의해 cross-bridges의 활성이 억제 2. Ca 2+ 이 Tn. C에 결합하면 myosin head의 ATPase가 활성 tropomyosin을 이동시켜(uncover actin site) : myosin head 가 actin에 bind active complex형성되며 muscle contracts 3. low-energy rigor com: mechanical work (rowing motion of the cross-bridge). 4. resting state : new ATP binds to rigor complex dissociates cross-bridge from thin filament
")
Resting : cardiac cell 내부 transmembrane potential : 90 m. V (-80~-100 m. V) Resting sarcolemma : Na+ impermeable ATP require Na+, K+ pump cell 내부는 K+이, 외부는 Na+이 높다. action potential phase 2 : Ca 2+이 cell 내부로 유입 T tubule로 들어가 SR에서 많은 양의 Ca 2+을 release intracellular Ca 2+증가→Ca 2 - troponin C 결 합하여 myocyte 수축. Repolarization : Ca 2이 SR reaccumulation Ca 2+농도가 감소 → relaxation, contraction -relaxation 반복

B. Myocardial Mechanics and Cardiac Function 1. THE ROLE OF MUSCLE LENGTH ( Frank-Starling relation ) developed force (= ventricular contraction)은 muscle fibers 의 initial length 에 비례 (= LVEDV : ventricular end-diastolic volume. ) 2. THE FORCE-VELOCITY CURVE mechanical activity of cardiac muscle : expressed as shortening and tension development force-velocity relation velocity of shortening ; 발생한 tension 에 반비례

3. VENTRICULAR EJECTION and Filling ; ventricular function curve sv EDV = preload stretching of myocardium Heart as a pump : (Frank-Starling relation). relation between EDV (length of the muscle fibers) and stroke volume Stroke volume : diastolic fiber length (EDV = preload)와 비례 arterial resistance (afterload = BP)와 반비례 Level of contractility Relation between ventricular end-diastolic pressure ( = EDV) and stroke work of ventricle (ventricular function curve )

C. CONTROL OF CARDIAC PERFORMANCE AND OUTPUT : 4 major determinant factor = aftreload

The cardiac cycle A = isovolumic contraction B = ejection a = isovolumic relaxation b = early diastolic filling c = diastasis d = atrial filling. 1, aortic valve opening 2, aortic valve closure 3, mitral valve opening 3 a, pressure nadir; 4, rapid early diastolic filling 5, onset of atrial contraction 6, end-diastole
 and Stroke volume(SV) Fick principle로 측정")
4. Assessment of Cardiac Performance A. Cardiac output(CO) and Stroke volume(SV) Fick principle로 측정 Cardiac index = Cardiac output (L/min)/body surface area (m 2) Normal range: 2. 5 - 3. 6 L/min/m 2 Heart failure:failure to increase C. O. during exercise decrease C. O. at rest B. Stroke volume and ejection fraction (EF) SV= LVEDV - LVESV Ejection fraction = stroke volume/ventricular end-diastolic volume Estimate by angiography, radionuclide, or echocardiography Normal:EF 67 ± 8%, LVEDV : 70± 20 ml/m 2 C. Ventricular end-diastolic pressure Inadequate systolic emptying of ventricle : increased EDV and EDP normal LVEDP: 12 mm. Hg = pulmonary capillary wedge pressure normal RVEDP: 6 mm. Hg = central venous pressure

D. End-systolic left ventricular pressure-volume relationship √ useful index of vent. performance : independ. of both preload, afterload at any level of myocardial contractility left ventricular end-systolic volume 은 end-systolic pressure와 역비례 preload and afterload 변화 no change in contractility, ESPVR is unchanged Contractility 증가 : ESPVR : left로 이동 (lower ESV at any ESP) SV증가 (1→ 3). Afterload 증가 SV falls (1→ 2); Preload 증가 SV rises (1→ 3). Contractility 저하, ESPVR : right로 이동 ESV증가, SV감소 (1→ 2). SV

E. Systolic time intervals total electromechanical systole = ventricular ejection time + preejection period pre-ejection period / ejection time = 0. 35 ± 0. 04 F. Ventricular dyssynergy hypokinesis, akinesis, dyskinesis G. Rate of increase in intraventricular pressure (dp/dt) clinical assessment of contractility, peak dp/dt H. Regional left ventricular function I. Exercise A useful technique for evaluating ventricular performance 정상 : O 2 consumption 이 100 m. L/min 증가 → CO 500 m. L/min 이상증가 LVEDP : 12 mm. Hg 유지(운동시에도) Failing LV LVEDP> 12 mm. Hg, subnormal increase in CO treadmill Ex- Vmax. O 2(maximal O 2 consumption)< 10 m. L/min/kg 정상> 20 m. L/min/ kg

5. DIASTOLIC FUNCTION Pressure-volume relation loop Normal 1 2 3 4 Diastolic dysfunction Impaired relaxation and filling ↑LVEDP

C. CONTROL OF CARDIAC PERFORMANCE AND OUTPUT = aftreload

Normal and Abnormal Myocardial Function The Failing Heart 심부전 Introduction Mechanisms of Heart Failure Neurohumoral and Cytokine Adjustments Heart Failure—A Disturbance of the Myocardial Pump
 Introduction 심장의 구조, 기능적 장애로 metabolizing tissues의")
D. THE FAILING HEART: heart failure (HF) Introduction 심장의 구조, 기능적 장애로 metabolizing tissues의 요구에 부합되게 심박출 하지 못하거나, LVEDV(P)가 증가해야 가능한 상태 1. Systolic HF : impaired myocardial contractility weak systolic contraction → ↓SV, CO cardiac dilatation, ↑LVEDP dilated cardiomyopathy, cardiogenic shock in MI 2. diastolic HF impaired relaxation / filling of ventricle ↑LVEDP stiff, thickened ventricle 3. Coexist cardiac hypertrophy and dilatation, systolic and diastolic HF 을
 curve SV CO contractility LVEDP, LVFP")
VENTRICULAR EJECTION and Filling ; ventricular function (Frank-Starling) curve SV CO contractility LVEDP, LVFP EDV, ED diameter Heart as a pump : (Frank-Starling relation). relation between EDV (length of the muscle fibers) and stroke volume Stroke volume : diastolic fiber length (EDV = preload)와 비례 arterial resistance (afterload = BP)와 반비례 Level of contractility Relation between ventricular end-diastolic pressure ( = EDV) and stroke work of ventricle (ventricular function curve)

Schematic LV pressure-volume relationship through 1 cardiac cycle in systolic heart failure, normal control and diastolic heart failure (right) impaired contractility Diastoie Impaired relaxation / filling ↑LVEDP Systole

D 1. MECHANISMS OF HEART FAILURE ADAPTIVE AND MALADAPTIVE MECHANISMS 1. Frank-Starling mechanism : enhancing contraction 2. Compensatory hypertrophy 3. Ventricular remodeling 4. ALTERATIONS IN ENERGY METABOLISM 5. ALTERATIONS IN SARCOMERIC PROTEINS 6. ABNORMALITIES OF EXCITATION-CONTRACTION COUPLING 7. MYOCARDIAL CELL DEATH D 2. NEUROHUMORAL AND CYTOKINE ADJUSTMENTS

D 1. MECHANISMS OF HEART FAILURE ADAPTIVE AND MALADAPTIVE MECHANISMS 1. Frank-Starling mechanism : enhancing contraction ↑ preload, ↑sensitivity to Ca 2 ventricular dilatation -- maladaptive in severe valvular regurgitation, → Laplace's law : ↑ wall stress, shortening 감소.

2. Compensatory hypertrophy 3. Ventricular remodeling insufficient hypertrophy Dilates, ↑wall stress ventricular hypertrophy로 ventricular filling장애 심근허혈 Laplace's law ↑ wall stress more spherical mechanical overload Hypertension Cardiomyopathy myocardial infarction.

ventricular remodeling more spherical Diastolic HF systolic HF combination of changes in left ventricular dilation and hypertrophy

Factors That Lead to the Progressive Remodeling of the Left Ventricle Cell Growth Fibrosis Apoptosis Counter-regulatory Factors Angiotensin II TNF-α ANP Catecholamines Endothelin Fas ligand Bradykinin Endothelin Aldosterone Nitric oxide TNF-α TGF-β BNP Growth hormone IGF Cardiotrophin-1 Mechanical stretch

4. ALTERATIONS IN ENERGY METABOLISM Acute, chronic ischemia : ↓supply of oxygen subendocardium ATP generation과 creatine phosphate 감소 myocardial energy reserves 감소 5. ALTERATIONS IN SARCOMERIC PROTEINS Hemodynamic overload, neurohormonal/ cytokine stimulation 으로 fetal sarcomeric proteins발현 : contractility 저하 troponin T, myosin light chain kinase 2 변화로 myosin ATPase activity 저하 6. ABNORMALITIES OF EXCITATION-CONTRACTION COUPLING disturbed delivery of Ca 2+ to the contractile protein 7. MYOCARDIAL CELL DEATH Apoptosis of myocytes hemodynamic overload, neurohormone/ cytokine stimulation severe ischemia로 유발되 → 생존 심근에 부하 증가 √
 2. renin-angiotensin-aldosterone")
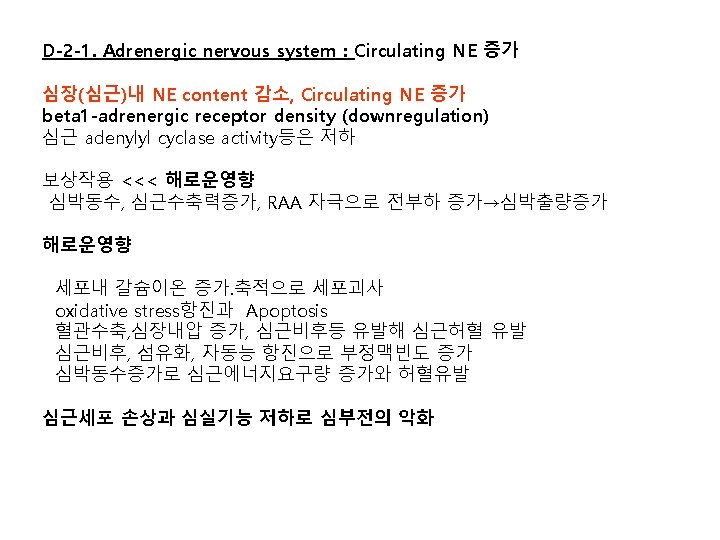
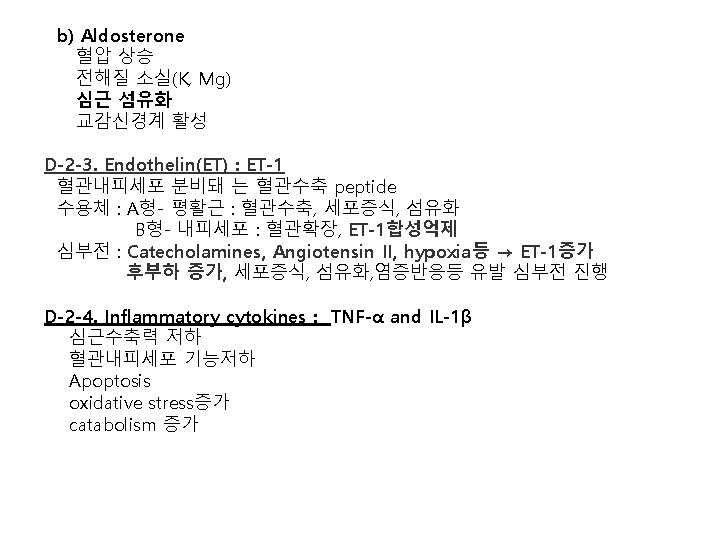
D 2. NEUROHUMORAL AND CYTOKINE ADJUSTMENTS Activation of 1. sympathoadrenal system (SAS) 2. renin-angiotensin-aldosterone (RAAS) 3. Endothelin 4. cytokines tumor necrosis factor (TNF) 5. argininevasopressin (AVP). renin 분비 증가 Juxtaglomerular 기구내 ß-1수용체 자극돼 신혈류량감소로 압력수용체자극
 circulating angiotensin II tissue renin-angiotensin system cardiotoxic effect activate")
D-2 -2. renin-angiotensin-aldosterone system. a) circulating angiotensin II tissue renin-angiotensin system cardiotoxic effect activate phospholipase C, protein kinase C. stimulates cardiac hypertrophy, ventricular remodeling. peripheral vasoconstrictor release of NE, aldosterone cellular hypertrophy, induction of fetal gene programs Apoptosis oxidative stress inflammation,
의 임상 Heart Failure (HF ; 심부전) 심장의 구조, 기능적")
Heart Failure (HF ; 심부전)의 임상 Heart Failure (HF ; 심부전) 심장의 구조, 기능적 장애로 metabolizing tissues의 요구에 부합되게 심박출을 하지 못하거나, LVEDV(P)가 증가해야 가능한 상태 Heart failure is a clinical syndrome of following features: • Symptoms typical of heart failure (breathlessness at rest or on exercise, fatigue, tiredness, ankle swelling) • Signs typical of heart failure (tachycardia, tachypnea, pulmonary rales, pleural effusion, raised jugular venous pressure, peripheral edema, hepatomegaly) • Objective evidence of a structural or functional abnormality of the heart at rest (cardiomegaly, third heart sound, cardiac murmurs, abnormality on the echocardiogram, raised natriuretic peptide concentration) 모든 심장질환이 원인 허혈성심질환, 판막증, 고혈압성 심질환, 심근증 Congestive Failure vs. Congestive State Congestive state:Overfilling of circulation without myocardial failure rapid infusion, anemia, chronic renal failure.

2. PRECIPITATING CAUSES 1. Infection : fever, tachycardia, hypoxemia, metabolic demand 증가 2. Arrhythmias. (a) Tachyarrhythmias : reduce ventricular filling, ischemic l (b) atrial 과 ventricular dissociation : loss of atrial booster pump (c) abnormal intraventricular conduction (d) bradyarrhythmias : cardiac output 저하 3. Physical, Dietary, Fluid, Environmental, and Emotional Excesses 4. Myocardial Infarction 5. Pulmonary Embolism 6. Anemia 7. Thyrotoxicosis and Pregnancy 8. Aggravation of Hypertension 9. Rheumatic, Viral, and Other Forms of Myocarditis 10. Infective Endocarditis

3. FORMS OF HEART FAILURE • New onset First presentation Acute or slow onset • Transient • Chronic Recurrent or episodic Persistent Stable, worsening, or decompensated 1. Acute vs. Chronic Heart Failure Acute:Acute myocardial infarction, acute valvular regurgitation Chronic:Rheumatic valvular disease, hypertension, cardiomyopathy acute failure : sudden ↓ cardiac output, systemic hypotension without peripheral edema, chronic failure : arterial pressure well maintained, edema. 2. Left vs. Right Heart Failure Left HF:Coronary arteriosclerosis, hypertension : pulmonary congestion and edema. Right HF:most common causes : left ventricular failure pulmonary stenosis, pulmonary hypertension. Systemic venous congestion and peripheral edema. Combination of left and right ventricular failure:traditional heart failure.

3. Backward vs. Forward Heart Failure Backward:Daming of blood proximal to the failing ventricle venous congestion-- sundrome of heart failure. Forward: decrease in cardiac output and underfilling of artery. 4. Low vs. High output failure Low:Common causes of HF, hypertension, vulvular High:Cardiac output is normal or elevated Hyperthyroidism, anemia, beri, A-V fistula, . 5. Congestive Failure vs. Congestive State 6. Systolic vs. Diastolic Failure · Systolic failure:inable to expel sufficient blood, inadequate CO. · Diastolic failure:relax & filling 장애, decreased compliance, elevation of filling pressure.

Key features of the clinical history in patients with heart failure Symptoms Breathlessness Fatigue Angina, palpitations, syncope (orthopnoea, paroxysmal nocturnal dyspnea) (tiredness, exhaustion) Cardiovascular events Coronary heart disease Myocardial infarction Thrombolysis Intervention PCI Other surgery CABG Stroke or peripheral vascular disease Valvular disease or dysfunction Risk profile Family history, smoking, hyperlipidaemia, hypertension, diabetes Response to current and previous therapy
 Coronary")
Common causes of heart failure due to disease of heart muscle (myocardial disease) Coronary heart disease Hypertension Many manifestations left ventricular hypertrophy and preserved ejection fraction Cardiomyopathies* Familial/genetic or non-familial/non-genetic (including acquired, e. g. myocarditis) Hypertrophic (HCM), dilated (DCM), restrictive (RCM), arrhythmogenic right ventricular (ARVC), unclassified Drugs β-Blockers, calcium antagonists, antiarrhythmics, cytotoxic agents Alcohol, medication, cocaine, trace elements (mercury, cobalt, arsenic) Diabetes mellitus, hypo/hyperthyroidism, Cushing syndrome, adrenal insufficiency, excessive growth hormone, pheochromocytoma Deficiency of thiamine, selenium, carnitine. Obesity, cachexia Toxins Endocrine Nutritional Infiltrative Others Sarcoidosis, amyloidosis, hemochromatosis, connective tissue disease Chagas' disease, HIV infection, peripartum cardiomyopathy, end-stage renal failure

4. CLINICAL MANIFESTATIONS : Symptom Dyspnea:Dyspnea on exertion, the first symptom Orthopnea:Dyspnea soon after lying flat, relieved by sitting up Cough, sputum:Venous congestion , edema of tracheobronchial walls Paroxysmal nocturnal dyspnea:urgent respiratory distress, relief by sitting up open window to breath fesh air. labored respiration, cardiac asthma Acute pulmonary edema:Acute episode of LVF(acute myocardial infarction) Respiratory alkalosis ( hyperventilation) → respiratory acidosis Hemoptysis: Rusty sputum-heart failure cells (alveolar macrophages- hemosiderin). Frank bloody sputum : pulmonary infarction. Cheyne-Stokes respiration: Periodic breathing of apena and hyperventilation Discrepancy between arterial and alveolar gas tension Fatigue and weakness:Reduction of perfusion of skeletal muscle Cerebral symptoms : Neurathenia, headache insomnia, anxiety Urinary symptoms : Nocturia, oliguria Cyanosis

5. Physical signs General appearance:Pale, breathlessness Skin:Cold and sweaty Pulse:Weak, narrow pulse pressure Pulsus alternans:Alternating strong and weak pulse * Electrical alternans Heart:Enlarged P 2 accentuation, Gallop (ventricular, atrial, summation) Lung:Bilateral basal moist rale-terminal bronhioles and alveolar edema Systemic venous congestion : hallmark of right heart failure Cardiac edema prominent jugular vein jugular pulse (prominent V wave-functional tricuspid insufficency) Hepatojugular reflux Hepatomegaly-cardiac cirrhosis Extracellular fluid accumulation Subcutaneous edema, hydrothorax, asctes, pericardial effusion, anasarca Cardiac cachexia

6. 심부전의 진단 : FRAMINGHAM CRITERIA FOR DIAGNOSIS OF CHF. Major criteria ·Paroxysmal nocturnal dyspnea ·Neck vein distension ·Rales ·Cardiomegaly ·Acute pulmonary edema ·S 3 gallop ·Increased venous pressure (> 16 cm. H 2 O) Minor criteria ·Extremity edema ·Night cough ·Dyspnea on exertion ·Hepatomegaly ·Pleural effusion ·Vital capacity reduced by one-third from normal ·Tachycardia (≥ 120 bpm) Major or minor ·Weight loss ≥ 4. 5 kg over 5 days treatment 진단 기준 : At least one major and two minor criteria

Classifications of the severity of heart failure in acute infarction myocardial Killip classification Forrester classification estimate of clinical severity of circulatory Designed to describe clinical and derangement in treatment haemodynamic status in acute myocardial infarction. Stage I No heart failure. No signs of cardiac decompensation 1. Normal perfusion and PCWP = left atrial pressure) Stage II Heart failure. rales, S 3 gallop, pulmonary venous hypertension. Pulmonary congestion with wet rales in the lower half of the lung fields. Severe heart failure. Frank pulmonary edema with rales throughout the lung fields Cardiogenic shock. hypotension (SBP <90 mm. Hg), peripheral vasoconstriction ( oliguria, cyanosis and sweating) 2. Poor perfusion and low PCWP (hypovolaemic) Stage III Stage IV 3. Near normal perfusion and high PCWP (pulmonary edema) 4. Poor perfusion and high PCWP (cardiogenic shock)
 NT-pro. BNP, BNP")
심부전 진단 지침(Guideline) NT-pro. BNP, BNP

Common ECG abnormalities in heart failure Abnormality Causes Clinical implications Sinus tachycardia Decompensated HF, anaemia, fever, hyperthyroidism Clinical assessment Laboratory investigation Sinus bradycardia β-Blockade, digoxin, Anti-arrhythmics Hypothyroidism, Sick sinus syndrome Evaluate drug therapy Laboratory investigation Atrial tachycardia/flutter/ fibrillation Hyperthyroidism, infection, mitral valve Diseases, Decompensated HF, infarction Slow AV conduction, medical conversion, electroversion, catheter ablation, anticoagulation Ventricular arrhythmias Ischemia, infarction, cardiomyopathy, myocarditis Laboratory investigation hypokalaemia, hypomagnesaemia Exercise test, perfusion studies, coronary Digitalis overdose angiography, electrophysiology testing, ICD Ischaemia/Infarction Coronary artery disease Echo, troponins, coronary angiography, revascularization Q waves Infarction, hypertrophic cardiomyopathy LBBB, pre-excitation Echo, coronary angiography LV hypertrophy Hypertension, aortic valve disease, hypertrophic Echo/Doppler cardiomyopathy AV block Infarction, drug toxicity, myocarditis, sarcoidosis, Evaluate drug therapy, pacemaker, systemic Lyme disease Microvoltage Obesity, emphysema, pericardial effusion, amyloidosis Echo, chest X-ray QRS length >120 ms of LBBB morphology Electrical and mechanical dysynchrony Echo , CRT-P, CRT-D
 redistribution")
Radiologic aspect Enlarged cardiac silhoutte Vasculature is prominent at apeces (pulmonary venous hypertension) redistribution of blood flow : edema & fibrosis of base Prominent septal line - Kerley’s B line Generalized clouding - pulmonary edema, Hydrothorax Acute Chronic

Diagnostic assessments of heart failure Assessment Diagnosis of heart failure Supports if present Opposes if normal or absent Compatible symptoms Compatible signs Cardiac dysfunction on echocardiography ++ +++ Response of symptoms or signs to therapy +++ ++ ECG Normal Abnormal Dysrhythmia ++ ++ + + Laboratory Elevated BNP/NT-pro. BNP +++ + + + + Chest X-ray Pulmonary congestion Reduced exercise capacity +++ + ++ Abnormal pulmonary function tests + + Abnormal haemodynamics at rest +++ ++ Low/normal BNP/NT-pro. BNP Hyponatraemia Renal dysfunction Mild elevations of troponin

Common chest X-ray abnormalities Abnormality Causes Clinical Implications Cardiomegaly Echo/Doppler Normal pulmonary findings Dilated LV, RV, atria Pericardial effusion Hypertension, aortic stenosis, hypertrophic cardiomyopathy Pulmonary congestion unlikely Pulmonary venous congestion Elevated LV filling pressure Left heart failure confirmed Interstitial oedema Elevated LV filling pressure Left heart failure confirmed Pleural effusions Elevated filling pressures HF likely if bilateral Consider non-cardiac aetiology if abundant If abundant, consider diagnostic or therapeutic centres Ventricular hypertrophy Echo/Doppler Reconsider diagnosis (if untreated) Serious lung disease unlikely Kerley B lines Pulmonary infection, surgery, malignant effusion Increased lymphatic pressures Hyperlucent lung fields Emphysema or pulmonary embolism Spiral CT, spirometry, Echo Pulmonary infection Pneumonia may be secondary to pulmonary congestion Systemic disease Pulmonary infiltration Mitral stenosis or chronic HF Treat both infection and HF Diagnostic work-up

Eur Heart J 2008 29: 2388 -2442
 Anaemia")
Common laboratory test abnormalities in heart failure Abnormality Increased serum creatinine (>150 µmol/L) Anaemia (<13 g/d. L in men, <12 in women) Hyponatraemia (<135 mmol/L) Hypernatraemia (>150 mmol/L) Hypokalaemia (<3. 5 mmol/L) Hyperkalaemia (>5. 5 mmol/L) Hyperglycaemia (>6. 5 mmol/L) Hyperuricaemia (>500 µmol/L) BNP >400 pg/m. L, NT-pro. BNP >2000 pg/m. L BNP <100 pg/m. L, NT-pro. BNP <400 pg/m. L Cause Renal disease ACEI/ARB, aldosterone blockade Clinical implications Calculate GFR, Consider reducing ACEI/ARB, or aldosterone blocker dose Check potassium and BUN Chronic HF, haemodilution, iron loss or Diagnostic work-up poor utilization, renal failure, Consider treatment chronic disease Chronic HF, haemodilution. AVP release, Consider water restriction, reducing diuretics diuretic dosage Ultrafiltration, vasopressin antagonist Hyperglycaemia Assess water intake Dehydratation Diagnostic work-up Diuretics, secondary Risk of arrhythmia hyperaldosteronism Consider potassium supplements, ACEIs/ARB, aldosterone blockers Renal failure, potassium supplement, Stop potassium-sparing treatment renin–angiotensin–aldosterone system (ACEIs/ARB, aldosterone blockers) blockers Assess renal function and p. H Risk of bradycardia Diabetes, insulin resistance Evaluate hydration, treat glucose intolerance Diuretic treatment, gout, malignancy Allopurinol Reduce diuretic dose Increased ventricular wall stress HF likely Indication for echo Consider treatment Normal wall stress Re-evaluate diagnosis HF unlikely if untreated
 Albumin low (<30 g/L) Transaminase increase Elevated troponins Abnormal thyroid")
Albumin high (>45 g/L) Albumin low (<30 g/L) Transaminase increase Elevated troponins Abnormal thyroid tests Urinalysis INR >2. 5 CRP >10 mg/L, neutrophilic leukocytosis Dehydratation, myeloma Rehydrate Poor nutrition, renal loss Diagnostic work-up Liver dysfunction Diagnostic work-up Right heart failure Liver congestion Drug toxicity Reconsider therapy Myocyte necrosis Evaluate pattern of increase (mild Prolonged ischaemia, severe increases common in severe HF) HF, myocarditis, sepsis, renal failure, Coronary angiography pulmonary embolism Evaluation for revascularization Hyper/hypothyroidism Amiodarone Treat thyroid abnormality Proteinuria, glycosuria, bacteria Diagnostic work-up Rule out infection Anticogulant overdose Evaluate anticoagulant dosage Liver congestion Assess liver function Assess anticoagulant dose Infection, inflammation Diagnostic work-up

Common echocardiographic abnormalities in heart failure Measurement LV ejection fraction LV function, global and focal Abnormality Reduced (<45– 50%) Akinesis, hypokinesis, dyskinesis Clinical implications Systolic dysfunction Myocardial infarction/ischaemia Cardiomyopathy, myocarditis End-diastolic diameter Increased (>55– 60 mm) Volume overload HF likely End-systolic diameter Increased (>45 mm) Volume overload HF likely Fractional shortening Reduced (<25%) Systolic dysfunction Left atrial size Increased (>40 mm) Increased filling pressures Mitral valve dysfunction Atrial fibrillation Left ventricular thickness Hypertrophy (>11– 12 mm) Hypertension, aortic stenosis, hypertrophic cardiomyopathy Valvular structure and function Valvular stenosis or regurgitation primary cause of HF or complicating aortic stenosis and mitral insufficiency) factor Assess gradients and regurgitant fraction Mitral diastolic flow profile Abnormalities of the early and late Diastolic filling patterns Tricuspid regurgitation peak velocity Pericardium Increased (>3 m/s) Aortic outflow velocity time integral Inferior vena cava Indicates diastolic dysfunction and suggests mechanism Increased right ventricular systolic pressure Suspect pulmonary hypertension Effusion, haemopericardium, thickening Consider tamponade, uraemia, malignancy, systemic disease, acute / chronic pericarditis, constrictive pericarditis Reduced (<15 cm) Reduced low stroke volume Dilated Retrograde flow Increased right atrial pressures Right ventricular dysfunction Hepatic congestion
 : systolic dysfunction 2. Assessment of LV")
Echocardiography 1. Left ventricular ejection fraction (LVEF) : systolic dysfunction 2. Assessment of LV diastolic function 정상 30 -35 50

Doppler-echocardiographic indices and ventricular filling Doppler indices E/A waves ratio Pattern Restrictive High filling pressures ( short deceleration time <115 to 150 ms) Volume overload Slowed relaxation (<1) Increased (>15) Reduced (<8) Intermediate (8– 15) >30 ms Normal filling pressures Poor compliance Inconclusive as may be pseudo-normal High filling pressures Low filling pressures Inconclusive Normal filling pressures <30 ms >D wave <45 cm/s >2. 5 <2 Change of the pseudonormal to abnormal filling pattern High filling pressures Low filling pressures Slow relaxation High filling pressures Low filling pressures Unmasks high filling pressure in Systolic and diastolic dysfunction Normal (>1) E/Ea (A mitral–A pulm) duration Pulmonary S wave Vp E/Vp Valsalva manoeuvre Consequence
")
Doppler echo : DIASTOLIC DYSFUNCTION 진단 Normal : E>A rapid in early diastole (E) than atrial systole(A) impaired relaxation : E<A Pseudo-normalized E>A, ↓Em = Am High E / E’ : >> 15, Higher LVEDP MV 통과하는 헐류의 속도 (E : 70 - 80 cm/s) 승모판륜의 속도 (Em = E’ : 10 cm/s) Restrictive ↑↑E>A, ↓Em = Am E/Em = E/E’>12, Em = Am(5 cm/sec)

A E E A DT E / A ratio : 0. 5 deceleration time (DT) : 280 ms Progresses restriction to filling high early diastolic velocity low velocity at atrial contraction high E / A 3. 0 DT of 120 ms

7. Stages & Classes of Heart Failure : ACC /AHA Designed to emphasize preventability of HF Designed to recognize the progressive nature of LV dysfunction
 Class I:without limiting of Ordinary physical activity Class")
FUNCTIONAL CAPACITY OF HEART FAILURE (NYHA) Class I:without limiting of Ordinary physical activity Class II:Slight limitation of physical activity. Comfortable at rest, ordinary physical activity results Sxs Class III:Marked limitation of physical activity. Comfortable at rest, less than ordinary activity cause Sxs Class IV: Inability to carry out any physical activity without discomfort. Symptoms of cardiac insufficency persistent even at rest. If any physical activity is undertaken, discomfort is increased COMPLEMENT, DO NOT REPLACE NYHA CLASSES NYHA Classes - shift back/forth (in response to Rx and/or progression of disease Stages - progress in one direction due to cardiac remodeling

8. MANAGEMENT OF CONGESTIVE HEART FAILURE Management outline of CHF Establish heart failure Ascertain presenting features: pulmonary edema, exertional breathlessness, fatigue, peripheral edema Assess severity of symptoms Determine etiology of heart failure Identify precipitating and exacerbating factors Identify concomitant diseases relevant to heart failure and its management Estimate prognosis Assess complicating factors (e. g. renal dysfunction, arthritis) Choose appropriate management Monitor progress and manage accordingly Counsel patient and relatives 심부전 치료의 원칙과 목표 원인질환의 교정, 진행을 억제 악화요소 제거, 완화 목표 좌심실 기능회복, 심부전 증상 개선, 사망률 감소, 삶의 질 향상

치료 Stage A Stage B Therapies NOT Recommended Digoxin should not be used in low EF with sinus rhythm, Ventricular rate control Noninvasive evaluation of LV function Calcium channel blockers with negative inotropic in low LVEF

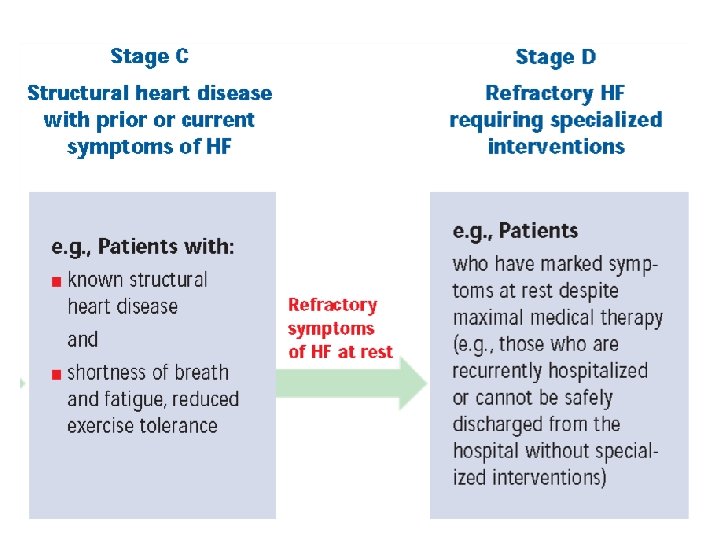
Stage C Stage D Cr ≤ 2. 0 mg/d. L →Cardiac Resynchronization →QRS duration > 120 ms Not Recommended Intermittent Intravenous LVEF < 35% LBBB Positive Inotropic

Class I recommendations for devices in patients with LV systolic dysfunction ICD Prior resuscitated cardiac arrest Ischaemic aetiology and >40 days of MI Class I Level A Non-ischaemic aetiology Class I Level B CRT NYHA Class III/IV and QRS >120 ms Class I Level A To improve symptoms/reduce hospitalization Class I Level A To reduce mortality Class I Level A

Nebivolol
 Target dose (mg)")
Dosages of commonly used drugs in heart failure Starting dose (mg) Target dose (mg) 6. 25 2. 5– 5. 0 2. 5 0. 5 t. i. d. b. i. d. o. d. 50– 100 10– 20 20– 35 5 4 t. i. d. b. i. d. o. d. ACEI Captopril Enalapril Lisinopril Ramipril Trandolapril ARB Candesartan Valsartan 4 or 8 40 o. d. b. i. d. 32 160 o. d. b. i. d. Aldosterone antagonist Eplerenone Spironolactone 25 25 o. d. 50 25– 50 o. d. 1. 25 o. d. 10 o. d. 3. 125 b. i. d. 25– 50 b. i. d. 12. 5/25 o. d. 200 o. d. 1. 25 o. d. 10 o. d. β-Blocker Bisoprolol Carvedilol Metoprolol Nebivolol

DIASTOLIC FUNCTION Pressure-volume relation loop 1. acute ischemia ventricular relaxation 장애 2. ↓ventricular distensibility restrictive cardiomyopathies extrinsic compression constricted or tamponade 3. ↑ ventricular mass / wall thickness a. concentric left ventricular hypertrophy, aortic stenosis, hypertension hypertrophic cardiomyopathy b. ↑intrinsic myocardial stiffness infiltration (e. g. , amyloidosis) endomyocardial fibrosis, ischemia Normal Diastolic dysfunction 4. volume overload acute valvular regurgitation acute left ventricular failure : myocarditis

Stage C

Treatment of Heart Failure and Normal Left Ventricular Ejection Fraction control systolic and diastolic hypertension, in accordance with guidelines. I control ventricular rate in patients with atrial fibrillation. I diuretics to control pulmonary congestion and peripheral edema. I Recommend coronary revascularization in patients with CAD in whom symptomatic or demonstrable myocardial ischemia is judged to be having an adverse effect on cardiac function. Restoration and maintenance of sinus rhythm in patients with atrial fibrillation might be useful to improve symptoms. IIa IIb The use of beta-adrenergic blocking agents, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, or calcium antagonists in patients with controlled hypertension might be effective to minimize symptoms of heart failure. IIb The use of digitalis to minimize symptoms of heart failure might be considered. IIb

Management of patients with heart failure and atrial fibrillation General recommendations • Precipitating factors and co-morbidities should be identified • HF treatment should be optimized Rhythm control • Immediate electrical cardioversion : patients with new-onset AF, myocardial ischaemia, symptomatic hypotension, symptoms of pulmonary congestion rapid ventricular response not controlled by appropriate pharmacological measures Rate control • Digoxin alone or in combination with β-blocker is recommended Prevention of thromboembolism • Antithrombotic therapy is recommended, unless contraindicated • Optimal approach should be based on risk stratification: in patients at highest risk of stroke [prior stroke, transient ischaemic attack (TIA), or systemic embolism] oral anticoagulant therapy with a vitamin K antagonist

Management of arterial hypertension in patients with heart failure In hypertensive patients with evidence of LV dysfunction • Systolic and diastolic blood pressure should be carefully controlled therapeutic target of 140/90 and 130/80 mm. Hg in diabetics and high risk patients • Anti-hypertensives (renin–angiotensin system antagonists ; ACEIs or ARBs) In hypertensive patients with HFPEF: • Aggressive treatment (several drugs with complementary mechanisms of action) • ACEIs and/or ARBs should be considered the first-line agents

Eur Heart J 2008 29: 2388 -2442

Digitalis : Mechanism of Action. Blocks Na+ / K+ ATPase => ↑Ca+ + Inotropic effect Natriuresis : inhibiting Na+-K+ ATPase in the kidney, Neurohormonal control ↓Plasma Noradrenaline ↓ Peripheral nervous system activity ↓ RAAS activity ↑ Vagal tone Normalizes arterial baroreceptors Negative chronotropic effect Slowed A-V junction by direct effect and reflex vagal action ↑ refractory period in A-V junction ↑ automaticity:Purkinje cell Clinical Effects Improve symptoms Modest reduction in hospitalization Does not improve survival

Digitalis. Indications persistent symptoms of HF severe SXs not responded to ACE-i + diuretics + beta-blockers AF: to slow AV conduction(adjunctive to beta-blockers) not indicated as primary therapy for the stabilization in acute exacerbation of HF (fluid retention or hypotension) Dose : 0. 125 to 0. 250 mg / day Contraindications Digoxin toxicity Advanced A-V block without pacemaker Bradycardia or sick sinus without PM PVC’s and VT Marked hypokalemia W-P-W with atrial fibrillation little or no value HF sinus rhythm hypertrophic cardiomyopathy myocarditis, mitral stenosis chronic constrictive pericarditis, diastolic HF

range of 0. 5 to 1. 0 ng per m. L >2 ng per m. L : ↑ digitalis toxicity Hypokalemia or hyperkalemia Hypomagnesemia, Hypercalcemia Hyponatremia Hypothyroid Renal function Acid-base imbalance Concomitant drug administration Anesthetics Catecholamines and sympathomimetic Antiarrhythmic agent: quinidine, amiodarone, verapamil erythromycin itraconazole, cyclosporine, Treatment of digitalis toxicity Stop digitalis and diuretic Block:Atropine, pacemaker Tachyarrhythmia:Potassium supply in normal renal function Ventricular arrhythmia:Lidocaine, phenytoin Fab fragments of purified intact digitalis antibodies

5. Spironolactone. Indications Recent or current Sxs despite ACE-i, diuretics, dig. and b-blockers Recommended in advanced heart failure (III-IV) in addition to ACE-i and diuretics Hypokalemia Practical use Do not use if hyperkalemia, renal insuf. Monitor serum K+ at “frequent intervals” Start ACE-i first Start with 25 mg / 24 h If K+ >5. 5 mmol/L, reduce to 25 mg / 48 h If K+ is low or stable consider 50 mg / day

Nitrates. Clinical Use CHF with myocardial ischemia Orthopnea and paroxysmal nocturnal dyspnea In acute CHF and pulmonary edema : NTG sl / iv Nitrates + Hydralazine : intolerance to ACE-I (hypotension, renal insufficiency) Clinical indication of vasodilator therapy 1. Acute pulmonary edema 2. Acute myocardial infarction heart failure, cardiogenic shock mechanical complication: Acute mitral regurgitation ventricular septal rupture 3. Acute left ventricular failure due to cardiac overload: hypertensive crisis acute aortic regurgitation 4. Chronic vasodilator therapy: hypertension chronic myocardial failure:unresponse to cardiotonic and diuretics

Conditions associated with a poor prognosis in heart failure Demographics Clinical Advanced age* Hypotension* Ischaemic etiology*NYHA functional class III–IV* Resuscitated Prior HF sudden death* hospitalization* Poor compliance Tachycardia Renal dysfunction Pulmonary rales Diabetes Aortic stenosis Anaemia Low body mass index COPD Sleep-related breathing disorders Depression Electrophysiological Functional/ exertional Tachycardia Q waves Wide QRS* LV hypertrophy Complex ventricular arrhythmias* Reduced work, low peak VO 2* Laboratory Marked elevation of BNP/ NT pro-BNP* Hyponatraemia* Imaging Low LVEF* Elevated troponin* Elevated biomarker neurohumoral activation* Low heart rate variability. Poor 6 min walk Elevated creatinine/BUN distance Atrial fibrillation T-wave alternans High VE/VCO 2 slope. Elevated bilirubin Anaemia Periodic breathing Elevated uric acid Increased LV volumes Low cardiac index High LV filling pressure Restrictive mitral filling pattern, pulmonary hypertension Impaired right ventricular function

급성심부전, 심장성 쇽 Causes and precipitating factors of acute heart failure Ischaemic heart disease • Acute coronary syndromes • Mechanical complications of acute MI • Right ventricular infarction Circulatory failure • Septicaemia • Thyrotoxicosis • Anaemia • Shunts • Tamponade Valvular • Pulmonary embolism • Valve stenosis Decompensation of pre • Valvular regurgitation existing chronic HF • Endocarditis • Lack of adherence • Aortic dissection • Volume overload • Infections, especially Myopathies pneumonia • Postpartum cardiomyopathy • Cerebrovascular insult • Acute myocarditis • Surgery • Renal dysfunction Hypertension/arrhythmia • Asthma, COPD • Hypertension • Drug abuse • Acute arrhythmia • Alcohol abuse
")
AHF : clinical and hemodynamic characteristics (1)

Cardiogenic shock Reduced blood pressure systolic BP<90 mm. Hg drop of mean arterial pressure> 30 mm. Hg) low urine output (<0. 5 ml/kg/h) pulse rate >60 organ congestion. Organ hypoperfusion

Eur Heart J 2008 29: 2388 -2442
 noncardiogenic shock (sepsis) Pulmonary edema Hypovolemic Tamponade 우심실경색증")
Normal volume overload (acute renal failure) noncardiogenic shock (sepsis) Pulmonary edema Hypovolemic Tamponade 우심실경색증 폐색전증 systolic pump failure, acute mechanical defect (MR, AR, VSD) Critical MS, AS Cardiogenic shock 2 -4. Clinical classification of heart failure (Forrester classification)

Normal Diuretics Vasidilators NTGS, Nitroprusside Pulmonary edema Hypovolemic shock Fluid Normal BP : Vasodilators Low BP : Inotropics Vasopressors Cardiogenic shock Clinical classification of heart failure (Forrester classification).

Indications and dosing of vasodilators VASODILATOR THERAPY : Principles of action ↓afterload : improve ventricular empting: ↓ Reduce preload:↓ venous tone ↓ ventricular dimension and myocardial oxygen requirement

6. vasodilators Effects of vasodilators Agent Preload Afterload Nitroprusside +++ Nitrate +++ ± Hydralazine ± +++ Captopril ++ ++ VASODILATOR THERAPY : Principles of action ↓afterload : improve ventricular empting: ↓ Reduce preload:↓ venous tone ↓ ventricular dimension and myocardial oxygen requirement

positive inotropic agents Dopamine : precursor of norepinephrine hypotensive states and HF. At very low doses : dilates renal and mesenteric 2 to 10 µg/kg / min : myocardial ß-1 receptors 자극. little tachycardia higher doses : α-adrenergic receptors, ↑ arterial pressure. Dobutamine : synthetic sympathomimetic agent ß-1, 2, and α-1 receptors. potent inotropic action, modest cardio accelerating ↓peripheral vascular resistance
 : Smooth m. K channel opening : phosphodioesterase inhibition")
Levosimendan Ca sensitization (contractile proteins) : Smooth m. K channel opening : phosphodioesterase inhibition positive inotropic action peripheral vasodilation
- Slides: 87