Rickets PRESENTED BY DR KRITIKA JOSHI Assistant Professor

Rickets PRESENTED BY DR. KRITIKA JOSHI Assistant Professor Deptt. Of Kaumarabhritya HAMC&H
 • Classically, Vit. D deficiency predominantly causes defect")
Vitamin D deficiency Rickets (Nutritional Rickets) • Classically, Vit. D deficiency predominantly causes defect of bones, i. e. rickets in growing infants and children before closure of epiphysis. • In adults vitamin D deficiency causes Osteomalacia which is characterized by spongy trabecular bones resulting from demineralization after the closure of epiphysis. i. e. in adults.

Vitamin D • Vitamin D plays an important role in calcium and phosphorus homeostasis. • Vitamin D is absorbed in the small intestine, mainly in duodenum by an active transport. • The ultraviolet rays of the sunlight are responsible for converting the 7 -dehydrocholesterol( normally present under the skin) into Vit D 3 or cholecalciferol.

• Vit D 3 or cholecalciferol, further converted in to 25 hydroxycholecalciferol in liver. • 25 hydroxycholecalciferol is then converted to 1, 25 dihydroxycholecalciferol in kidney • In the intestine vit D induces a calcium transport system involving transport protiens and intracellular Ca binding protein(CBP) • In the kidney vit D enhances Ca reabsorption in the tubule by a mechanism similar to that in gut.
 Skin(Inactive form of vit")
Mechanism of Activation of Vitamin. D Sunlight (u. v. rays) Skin(Inactive form of vit D/ 7 dehydrocholesterol) 7 dehydrocholesterol converted into Vit D 3 or cholecalciferol (1 st Liver hydroxilation) 25 hydroxycholecalciferol Kidney hydroxilation) 1, 25 Dihydroxycholecalcifero {Active form of vit D} (2 nd

SOURCES OF VIT. D • Most food contain only small amount of preformed Vit D. Fish, liver and oils are good sources. • Human milk contains only 30 -40 IU/L. • In addition to dietry sources, photoconversion by the action of sunlight in ultraviolet band is an important source of vitamin D for infants and children.

Vitamin D Requirement • Produced endogenously in the skin. There is no nutritional requirement of vit D when suffiicient sunlight is available. • If not then, recommended daily dose in infants is 5 micro gm(200 IU) per day and in children 10 micro gm(400 IU) per day.

Deficiency Causes • • • . Absence of sun light exposure. Decreased synthesis by skin. Liver failure Kidney failure Fat malabsorption syndrome

SIGN & SYMPTOMS OF RICKETS General symptom v. Failure to gain wt. & height. v. Generalized muscle weakness. v. Delayed dentition. v. Delayed milestones. Head v. Open fontanale/Delayed closure. v. Softening of skull bones known as craniotabes. v. Frontal bossing(prominent frontal bone)

Thorax v. Protuberance at costochondral junction called rachitic rosary. v. Depression at lower costal margin known Harrison sulcus or groove. v. Pigeon chest(pectus carinatum) v. Recurrent chest infection. Extremities v. Widening of wrist joint. v. Leg pain. v. Lower limb deformity.
 Genu valgum(knock-knees) in older children. b) Genu varum(Bowed legs) in toddlers.")
a) Genu valgum(knock-knees) in older children. b) Genu varum(Bowed legs) in toddlers.

Spine: • Scolosis, kyphosis. • Severe deformity of the spine may end up with disproportionate short stature of short trunk type.

INVESTIGATIONS 1. Biochemical • Raised alkaline phosphatase (except in malnourished children in whom this may be normal). • Usually normal or somewhat low serum calcium and reduced phosphorus. • Reduction in the serum 25 -hydroxyvitamin D 3 level(<10 microgm/ml)is considerd a sensitive and reliable index of rickets even in malnourished children, this is the only way to diagnose subclinical Vit D deficiency.

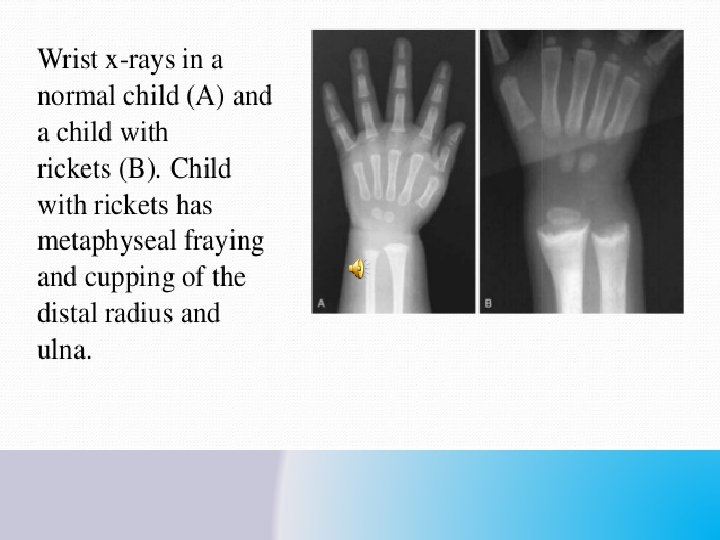
2. Radiological: Radiological findings are best seen in the wrist, i. e. lower ends of radius and ulna. These includes: • Cupping(saucer like concave depression) The osteoid (matrix-mineralisation), being radio translucent is not seen. In fact the space normally occupied by mineralized matrix, is empty. • Splaying : widening of metaphysial end of bone. • Fraying(rarefaction): Irregular tooth brush like margins(bottom of the cup)

Lower limb x-ray in rickets

• Treatment Specific treatment: stoss therapy consists of administering a single massive dose of vitamin D 3 6 lakh I. U. or 60, 000 I. U. for 10 days orally together with supplimentry calcium (50 -75 mg/kg/day ). • Radiological evidence –with in 4 weeks of therapy.

Prognosis • Response to pharmacotherapy is gratifying. • In certain cases a poor response to adequate doses of vitamin D 3 encountered. • In such a case probability of refractory or resistant rickets should be considered & the child should be investigated for following conditions: i. iii. iv. v. vi. Malabsorption Renal rickets Prolonged anticonvulsant therapy. Chronic liver disease. Hereditary vit. D dependent rickets. Oncogenic rickets.

• Prevention § Availability of at least 400 of vitamin D through sunshine, diet or supplement must be ensured. § Health education to parents against over clothing the infants and young children.
 • Rare autosomal recessively")
Some Other types of rickets 1. VITAMIN D Dependent rickets(VDDR) • Rare autosomal recessively inherited rickets. • Seen in infants b/w age 3 to 6 months, who have been receiving the usual amount of Vit D. q 2 Forms are seen § VDDR TYPE 1 § VDDR TYPE 2

VDDR TYPE 1 VDDR TYPE 2 • Deficiency of enzyme 25 hydroxyvitamin D-1 -alfa Hydroxylase. • There is end organ resistance to 1, 25 dihydroxy D 3. • Blood level of 25(OH)D 3 are normal but those of 1, 25 dihydroxy D 3 are markedly decreased. • This leads to virtual abolition of actions of 1, 25 dihydroxy D 3, despite its markedly raised levels in circulation. (secondary to hypocalemia and low 24 -hydroxylase activity). • C/F are same as Vit D deficiency rickets and include hypotonia growth failure motor retardation (Poor head control, Delayed Standing and Walking). • The treatment of VDDR TYPE 1 Alfacalcicidol or calcicitrol ( 1 to 2 microgms daily) with Ca , with or without phosphorus. • Early onset of rickets, high prevalence of alopecia and ectodermic defect. • The response to treatment in patients is not satisfactory.

2. Chronic Kidney Disease • It may be a cause of Refractory rickets. • Elevated blood levels of creatinine and phosphate are characteristic. • Therapy consists of restricting of phosphate intake and providing supplements of Ca and active Vit D analogs.

• 3. Oncogenous Rickets • Rarely benign mesenchymal tumors may secrete a circulating substance that results in phosphaturia, hypophosphatemia, rickets and muscle weakness. • The tumor may be small and difficult to detect. • But removal of tumor reverses the biochemical abnormalities and heal the rickets.

- Slides: 24