Physical Profiling in the Military CAPT Quinlan USN
 Leggit,")










 • Documented period of medically restricted duty, in consideration of")
 • PLD is defined as a need for a service")

 • Inherent in a PEB is the provider’s opinion that")

 –")
 –")









 Applications www. mods. army. mil")

 • Describes the Soldier’s capabilities utilizing the PRT program")






: • Most current")

 reviewed annually")





 • 469 Completed for DLC/MLC")












 to MOS Administrative Retention Review (MAR 2) The MAR")






- Slides: 72
Physical Profiling in the Military CAPT Quinlan, USN Maj Bunt, USAF COL (ret) Leggit, USA
Profiling 101 Physical Profiling Basics – Definition • Definition: – A means to communicate important medical restrictions, readiness status, or advice to a Service Member’s chain of command – Analogous to a civilian “work note” or “doctor’s note” Slide 2
Profiling 101 Physical Profiling Basics – Definition • Definition: – A means to communicate important medical restrictions, readiness status, or advice to a Service Member’s chain of command – Analogous to a civilian “work note” or “doctor’s note” • Is NOT – A sign of a weak or unmotivated soldier – The (automatic) end of someone’s career Slide 3
Profiling 101 Physical Profiling Basics – Definition • Definition: – A means to communicate important medical restrictions, readiness status, or advice to a Service Member’s chain of command – Analogous to a civilian “work note” or “doctor’s note” • IS: – A chance to maximize conditions for recovery from injury or illness – A means to prevent worsening of injury – A place to document significant, duty-limiting, diagnoses in the permanent personnel record – A communication tool between the doc and the commander Slide 4
Profiling 101 Physical Profiling Basics – Definition • Definition: – A means to communicate important medical restrictions, readiness status, or advice to a Service Member’s chain of command – Analogous to a civilian “work note” or “doctor’s note” • Can BE: – A source of inconsistency between providers – An end to someone’s deployability, promotion or assignment How? – A major sore spot for unit commanders and supervisors Slide 5
Primary Reference and System Navy & Marine Corps – MILPERSMAN 1306 -1200 & MANMED Chapter 18 Air Force- AFI 10 -203 and AFI 48 -123 Army- AR 40 -501 Chapter 3 and 7 & e-profile (new changes as of 6/1/2016)
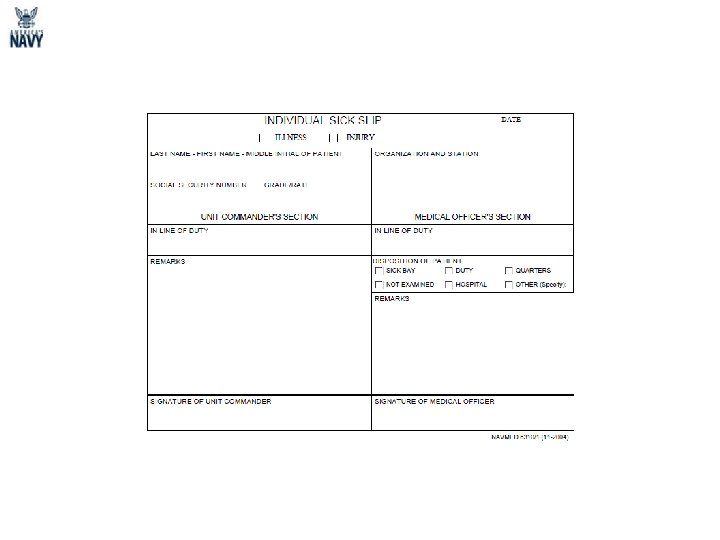
Profiling 101 Physical Profiling Basics – Types • Form used: DD 689 – a. k. a. “sick call slip” – Handwritten or typed – DD 689 is a “unit form, ” not a “hospital form” – NOT a “Get out of work free” card Quarters for 48 hours – Per MEDCOM MSG PT at own pace & (June 2012), the DD 689 distance for 7 days is no longer authorized for restrictions > 7 days – Special considerations • Can’t use for convalescent leave Air Force Doesn’t use this form any longer (CON LV) Navy same form but called NAVMED 6310/1 • Cannot specify an alternate Army Physical Fitness Test Slide 7
PEB MEB Physical Evaluation Board Medical Evaluation Board • Three Medical Officers • No Line Officers • Summarizes medical treatment, exams, limitations • Local Board • Does condition meet medical retention standards? • • Medically Based Performance Based Two Line Officers One Medical Officer Industrial impact Considers what Command tells the PEB • Central Board • Does the condition and limitations prevent SM from performing duties? -Fit or Unfit for Duty
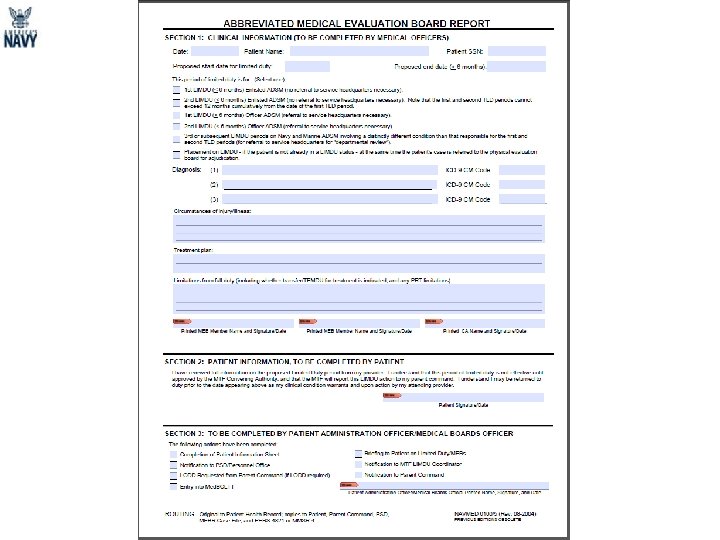
Navy & Marine Corps MEDICAL BOARDS Limited Duty/Physical Evaluation Board REFERENCES: MANMED, CHAPTER 18 MILPERSMAN 1306 -1200 SECNAVINST 1850. 4 E
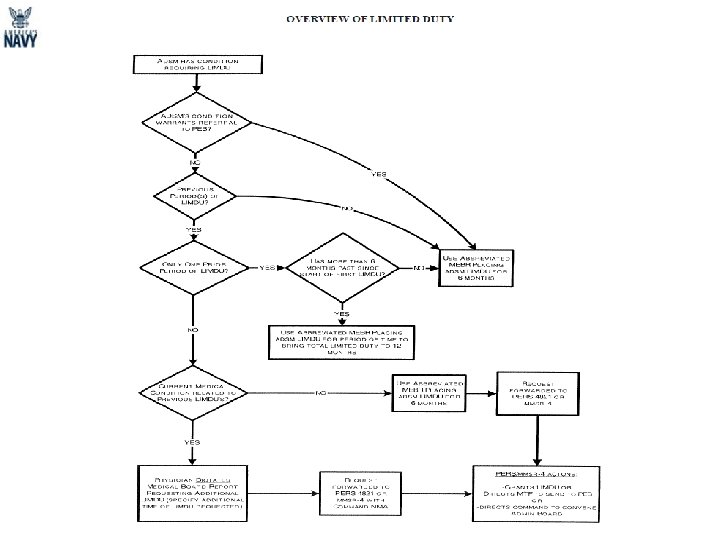
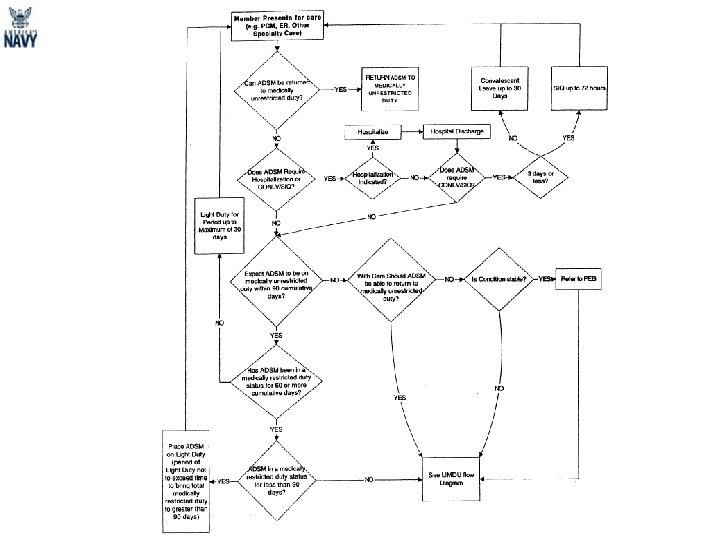
LIGHT DUTY • Light duty is a period when the member is excused from performing specified duties. A provider authorizes light duty in 30 day increments. Light duty will not exceed 90 consecutive days. At the end of the light duty period, the member will either be immediately returned to duty or referred to a Limited Duty or Physical Evaluation Board.
• • Limited Duty A period when a member is restricted from performing certain aspects of his military duties, usually in 6 months increments. Two periods of limited duty may be locally approved. Third periods of limited duty must be approved by Service Headquarters. Return to unrestricted duty is anticipated.
Temporary Limited Duty (TLD) • Documented period of medically restricted duty, in consideration of a patient’s illness, injury, or disease process. • Most appropriate only for Sailors whom a return to medically unrestricted duty status is anticipated. • The Convening Authority of a Medical Treatment Facility (MTF) has the authority to authorize up to twelve months of TLD for enlisted Sailors. Any additional TLD MUST be submitted for approval to Navy Personnel Command (PERS-454) • All requests for TLD involving Officers MUST be submitted to Navy Personnel Command (PERS-454). A member whose case has been referred to the Physical Evaluation Board (PEB) for disability adjudication will be concurrently placed on TLD pending the PEB outcome.
Permanent Limited Duty (PLD) • PLD is defined as a need for a service member’s skill or experience that justifies the continuance of that service member on active duty in a limited assignment; the service member may be retained on active duty or in active status for a specified period of time. Each case is individually considered, and the member’s length of service is not controlling in PLD decisions. • PERS-82 may, upon a member's request, particularly from a member with over 18 years but less than 20 years of active service, retain unfit to continue naval service members in a PLD status when such retention is in the best interests of the service and consistent with the guidance in paragraph 6003 of SECNAVINST 1850. 4 E. • Permanent Limited Duty (PLD) will not be approved when retention in a PLD status would jeopardize the member’s health or safety, or that of others
The following criteria must be met for consideration: • • 1. Member must be found “UNFIT” by the Integrated Disability Evaluation System (IDES)/Physical Evaluation Board (PEB). 2. Unfit member must be able to maintain his or herself in a normal military environment, without adversely affecting his or health or the health of other members. The IDES/PEB will determine if member is a risk. 3. Unfit member may be retained to complete service obligations for Navy funded education or training (i. e. , initial and advanced skill training schools). Unfit member may be retained to meet shortages against authorized strength in an enlisted skill, competitive category, designator or specialty, or a military occupational field or specialty, provided they can perform required duties in an authorized billet for that skill. 4. Unfit member may be retained to complete a current tour of duty or to provide continuity in key billets pending relief. 5. Unfit members may be retained for a specified period of time, at the request of a commanding officer of a medical treatment facility, to meet the need for that specific type of condition in a graduate medical education program at a specific MTF that cannot be met at that MTF by other authorized means and is essential to maintaining program accreditation. 6. Unfit member may be retained to reach fleet reserve eligibility if member has over 18 years of active service per U. S. Title 10, Chapter 61. 7. Member must not be a risk per the IDES/PEB.
PHYSICAL EVALUATION BOARD (PEB) • Inherent in a PEB is the provider’s opinion that the member’s condition is of such severity as to interfere with the ability to adequately perform his or her duties.
FIT TO CONTINUE SERVICE: • Fit: Member can reasonably perform duties of their office, grade, rank or rating. Fit does not mean “fit for full duty” or “suitable. ” • Suitable: Member meets all requirements for an overseas, remote or operational assignment. • Although the PEB determines that a member is FIT, he/she may not be able to: - Pass PFA/PFT - Deploy - Serve in Special Duty assignments (flight, submarine, etc. )
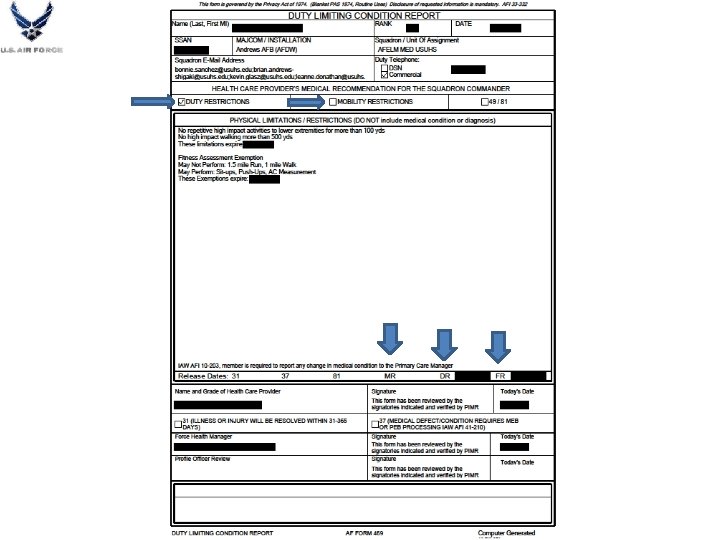
Profiling 101 Air Force Physical Profiling Basics – Types • Duty-Limiting Condition (DLC) – – – Completed on AF Form 469 in ASIMS, define Duty Restrictions (DR) Definite endpoint (Cannot be entered for longer than 365 days) Expectation is that the condition will improve or resolve Need to include verbiage about what the member cannot do Need to include fitness restrictions (FR) (pushups, situps, running/walking, abdominal circumference) – Commander must approve (can deny!!) – Does not lead directly to a MEB* • *However, 365 cumulative days of profile for same condition will require referral to DAWG (Deployment Availability Working Group) at your local MTF • *Certain conditions/diagnoses will automatically require MEB (Cancer, Asthma, OSA, Diabetes, etc. ) Slide 24
Profiling 101 Air Force Physical Profiling Basics – Types • Mobility-Limiting Condition (MLC) – Completed on AF Form 469 (Check Mobility-Limiting box) – Indefinite or Definite endpoint for Mobility Restrictions (MR) – Condition may NOT improve or resolve – Associated with specific diagnosis – NOT worldwide qualified – MR required to be checked if: • Cannot run at least 100 yds, Carry up to 40 lbs or live in austere environment – Will likely lead directly to a MEB* • *Pregnancy is mobility restricting, but does not lead to an MEB Slide 25
USAF DAWG • DAWG Referral initiated in ASIMS • DAWG evaluates and determines – Return to Duty, no restrictions – Return to Duty, continue yearly 469 DR/FR entry – Return to duty with Assignment Limitation Code (ALC) – Complete i. RILO/Narrative Summary (local MEB at DAWG) – Forward to full MEB (San Antonio, TX)
MEBs AF • DAWG performs local MEB • Assignment Limitation Codes – Return to Duty with code limiting mobility – Examples (OSA, Asthma) • Yearly Review-in-lieu-of (RILO) MEB – Completed by PCM – May require additional secondary care input
USAF Form 422 • Medical Clearance Form • Overseas and Re-training form • Exercise Prescriptions • No longer utilized by provider for FR
Policy Changes Program requires specific changes to MR policy and standardized practices Current Regulations New Regulations AR 40 -501 Standards of Medical Fitness Chapter 3: Retention Standards Chapter 7: Physical profiling Chapter 11: Deployability • Medical Readiness AR will cover medical readiness standards, physical profiling, and deployment requirements • Medical Readiness DA PAM published to describe how to use new reg. New Policy: SECARMY Directive, Medical Readiness AR and DA PAM Policy Revisions: AR 40 -501, AR 220 -1, AR 635 -40 and AR 600 -8 -101
“Available” to “Deployable” Soldiers Deployable – A Soldier under the direct operational control of the reporting unit, whether present or can be present within 72 hours, who is in compliance with all required personnel readiness standards, and not restricted from deploying to perform the unit’s core designed and assigned missions. M 1 -Deoloyable M 2 -Deployable –quick fixes M 3 - Not Deployable - bigger issues-MEB/PEB, Pregnancy, etc (CDR can override) M 4 -Not Deployable- delinquent on issues or unknown issues (CDR can override) Applicable to all Operating & Generating Force Soldiers regardless of component. Non-Deployable – Abaseline Soldier individual who is • Non-Deployable Does not meet the Army’s restricted from worldwide for a unit’s as readiness standards fordeployment worldwide deployment core designed or assigned mission due one of defined by Administrative and Medicaltopolicies; following reasons: • the. Does not meet the Combatant Commander’s specific individual readiness standards when tailored for accomplishment of an assigned mission; • Cannot be under the direct operational control of the reporting unit (cannot be present within 72 hours); or • Has not graduated from an Area Of Concentration (AOC) or Military Occupational Specialty (MOS) awarding course. • Commander’s Call - any reason not mentioned above
Temporary & Permanent Profile Changes Temporary Profile Key Points • Written by credentialed provider within area of specialty • No PULHES designation • Should describe a stable limitation that will persist for a year or longer • No automatic recovery period • The numerical designator for the PULHES indicates the severity of the limitation • CO CDR review in 14 days AC, 30 days for NG/AR • All P 2 profiles must be signed by the profiling officer and a physician • Differentiated by duration • Chain of command must also review profiles at: • • Permanent Profile Key Points • >120 BN/SQD CDR • >180 BDE CDR • >240 Senior Commanders Up to one year in duration MRDP: consider transition to permanent profile • All P 3 & 4 must be signed by profiling officer and approval authority • QC/QA-second signatures • Will be reviewed and assessed at every readiness visit
Profiling Officers • Temporary profiles can be written by any privileged profiling officer working in a provider capacity (+/- countersignature) • Permanent profiles (P 2) must be signed by 2 profiling officers, the second signature needs to be a physician • Permanent profiles (P 3 & 4) must be signed by at least 2 profiling officers, the final signature needs to be a Approval Authority • Civilian providers • Credentialed in the Do. D�may serve as profiling officers according to their privileges, training, and knowledge. • Not credentialed in the Do. D �are not profiling officers • DOD providers will convert appropriate restrictions to a correctly-written and processed DA 3349 in e-Profile
Profiling Officers Who can write profiles? No Restrictions. Can • Physicians write a Temporary • Dentists profile up to a year on 90 days increment. • Audiologists • Optometrists Can write a • Podiatrists Temporary profile up • Chiropractors to 90 days and will need an extra • Physical Therapists signature (Physician) • Occupational Therapists to extend after 90 days. • Nurse Practitioners TP up to 90 days, then • Nurse Midwives re-evaluate up to • Licensed Clinical Psychologists/ Social Workers and 180 days W/S. Extra • Physician Assistants Sig. after 180 days. • Athletic Trainers (pre-decisional)
Approval Authority ARNG and State Surgeon • May be delegated to a physician as appropriate HRP Commander • May be delegated to a physician (Generally a MEB physician or a clinical deputy) USAR Command Surgeon • May be delegated to a physician as appropriate • Can be delegated (i. e. Profile Review Officer, Medical Board Provider) • Responsible for accurate, complete, consistent communication, as it relates to Medical Readiness policy • Approves all MEB packets (final review) • Applies the ‘S’ code if MEB determines the Soldier meets retention standards
Medical Operational Data System (MODS) Applications www. mods. army. mil
New DA 3349 Physical Profile • A single living document with temporary and permanent profiles on a single form • Incorporates all current functional and assignment limitations • Tracks total number of days a Soldier has been on profile and by condition • Increases visibility (MEB/IDES) • Permanent profiles must be transcribed into the new system within 15 months (with current supporting evidence if needed) • If in MEB/PEB process, only MEB physician can transcribe
New DA 3349 (Page 2) • Describes the Soldier’s capabilities utilizing the PRT program • Can take APFT on Temporary profile if allowed by provider • Shows both permanent and temporary APFT limitations • No automatic recovery period after profiling • Documents the Unit CDR’s review
Limitations vs. Duty Assignments Overly restrictive and should not be used Profiling limitations proper guidance • SM can only work from 9 -5 pm or SM cannot present to work until 1000 hours • No uniforms • No formations • No 24 -hour duty • No PT before 0800 • Requires eight consecutive hours of sleep in a 24 -hour period • Soldier should not be exposed to stimuli suggestive of combat experiences (i. e. , no simulator training, no ranges, no simulated mortars, no patrol lanes, no IED training, etc. ) • No alcohol • No weapons/ammunition • SM has been referred to the MEB process. No deployments to an austere environment; PCS, TDY or ETS until final fitness for duty has been determined
APFT/PRT Changes • Soldier may take a record APFT while on a temporary profile as indicated on profile • One aerobic event required • PRT capabilities will inform the command team of the activities Soldiers can safely perform within the limits of the profile • No automatic recovery period
Section 2: Permanent Profile KNEE PAIN ARM PAIN 2 3 S F V PA, NP MD MD AA Profile Issue Date 1 3 2 1 1 1 The PULHES is combined for all the permanent conditions listed on the profile. Profile codes describe administrative processes and/or deployment limitations. In this example above, the codes indicate that the permanent knee pain was determined by the MEB to meet retention standards and is reflected by a S code. The arm pain has a numerical designator of 3 indicating severe limitations and F and V codes describing the deployment limitations.
Physical Category Codes CODE Description F No assignment or deployment to OCONUS areas where definitive medical care for the soldier’s medical condition is not available S MEB. Soldier has been determined to meet medical retention standards by a Medical Evaluation Board T Waiver granted for a disqualifying medical condition/standard for initial enlistment or appointment V Deployment. This code identifies a soldier with restrictions on deployment to certain areas W MAR 2. Soldier has a permanent 3 or 4 profile with a MAR 2 finding of retain or reclassify and return to duty X COAD/COAR. Soldier is allowed to continue in military service with a medical condition that is below medical retention standards, pursuant to a waiver of retention standards, or waiver of unfit findings and continued on active duty or in active reserve status under AR 635 -40 Y Found Fit for duty after complete processing under AR 635 -40
Section 3: Temporary Profile Ankle Sprain 0 Moderate 0 Sports Yes 20160630 30 Jones, NP 20160730 x
Section 5: Medical Instructions to Unit Commander Medically-oriented instructions Profiling officers describe limitations and capabilities; commanders assign duties. Appropriate limitations: Requires eight consecutive hours of sleep in a 24 -hour period No alcohol (if medically indicated) No weapons/ammunition SM is referred to the MEB. No deployment to an austere environment. SM should remain near an MTF with definitive specialty care is available. Overly restrictive: SM can only work from 9 -5 pm or SM cannot present to work until 1000 hours No formations No 24 -hour duty No PT before 0800 hours
Behavioral Health Profiles OTSG/MEDCOM Policy Memo 15 -045 (Behavioral Health Profiling): • Most current guidance pending Medical Readiness policy publication. • Contains specific guidance for BH profiling actions and situations. • Describes and standardizes how to write BH-related duty limitations. Reasons to profile: • BH disorders that cause functional impairment in mission capability. • BH medications with significant potential side effects. • Deployability is compromised based on COCOM guidance. Not all BH conditions or use of medications warrant a profile: • Soldiers whose symptoms do not impair occupational functioning. • No requirement for enhanced commander support. • Examples include low dose, routine medications, with low risk of side effects
Behavioral Health Profiles Temporary BH profiles medication stabilization affect • Deployment (when new treatment regimen started in the last 90 days prior to deployment) • PCS (when determined to be medically unstable by a provider) • Refer also to AR 40 -501 Mental Status Evaluations (DA 3822) provide Commanders with current mental status for administrative actions – i. e. , schools, separations, Command directed evaluations, etc. • DA 3822 should not be used for detailing BH duty limitations • DA 3822 is not a profile substitute For any BH duty limitations lasting longer than 72 hours the provider will complete a DA 3349 (Profile) • Sick slip may be used for <72 hours
PHA Profiles (PULHES) reviewed annually
MAR 2 = MOS Administrative Retention Review Replaced the MMRB • Serves as administrative process for Soldiers who meet retention standards per AR 40 -501, chapter 3, but may be not able to satisfactorily perform their primary military occupational specialty or area of concentration (PMOS/AOC). To qualify for MAR 2, Soldiers with the permanent 3 & 4 profile • Perform all functional activities on the permanent profile • Complete an APFT aerobic event. • Meet AR 40 -501, chapter 3 retention standards. • Do NOT meet the PULHES requirements of their MOS/AOC per DA PAM 611 -21.
Medical Evaluation Board Non-Duty PEB MEB – Medical Evaluation Board • A Soldier must be referred to a MEB when he/she reaches the Medical Retention Determination Point (MRDP) with a PULHES of 3 or 4 • As soon as there is a single condition that fails retention standards (without expectation of recovery within 12 months) NDR-PEB – Non-duty Related Physical Evaluation Board • Any Reserve Component Soldier who fails retention standards for a condition that is not duty-related may request a non-duty related PEB determination of fitness.
How does each service handle? • Ankle Sprain/Fracture- Temporary condition that requires activity/duty modification • Chronic Back Pain with permanent inability to do sit-ups or run • Asthma- permanent condition requiring daily controller medication for maximal performance
Ankle Fracture/Sprain • Ankle Sprain/Fracture- Temporary condition that requires activity/duty modification
Navy • Ankle Sprain – Expected RTD < 60 days • Light Duty (NAVMED 6310 -1) – Expected RTD > 60 days • Limited Duty (NAVMED 6100(5)) • Ankle Fracture – Expected RTD > 60 days – Limited Duty (NAVMED 6100(5))
Air Force • 469 Completed for DLC (Ankle Sprain) • 469 Completed for DLC/MLC (Ankle Fracture) • Both would contain DR/FR • Definitive Endpoint based on surgeon/PCM • Upon completion of 469, member has 42 days to rehab/refit before can be PT tested
Army • Temporary Profile • PT Test?
Chronic Low Back Pain • Chronic Back Pain with permanent inability to do sit-ups or run
Navy • Initial Evaluation – Limited Duty • Up to 6 months • May repeat once • Follow Up Evaluation – Determine if member has had LIMDU previously – If so, refer to PEB – May seek permanent limited duty via PEB process
Air Force • 469 completed for DR and FR, +/- MR • Referral to DAWG after 365 cum days of DR/FR • Sooner if appears chronic, provider desire • DAWG evaluates and determines – As previously mentioned
Army • Permanent 2 profile with No Run and No Sit. Up Profile with alternate aerobic event
Moderate Persistent Asthma • Asthma- permanent condition requiring daily controller medication for maximal performance
Navy Requires referral to PEB
Air Force • MEB required per 48 -123 • i. RILO/Narrative Summary completed by PCM • Forwarded to DAWG • DAWG dispositions as previously mentioned
Army • Refer to AR 40 -501 Ch 3 -27 P 2 if need daily meds but can do all Army Functions P 3 and MEB if cannot
Profiling 101 Army Physical Profiling Basics – Special Situations ve • Pregnancy it n r e t a ea l y – Standardized approach at MTFs maximizes consistency among m s k pregnant Soldiers e e w – Additional details from applicable 2 1 regulations and ACOG Guidance e iv g provides medically-sound and t s consistent information m tou w supervisors and patients o n s – Allows (and encourages) e c i v Pregnancy & Postparticipation in r e S Partum Physical Training Program ll A (PPPPTP) – Serves as basis to update MEDPROS that Soldier is nondeployable Slide 63
Additional Material
Profiling 101 Physical Profiling Basics – Special Situations • APFT coming up ht g i e – Be suspect < 30 days of APFT d w an t – Check for “q-6 -month” pattern igh he t ee e ll n om t d e ti S – If a condition has come up that limits safe (NOT necessarily successful) performance on the APFT, then consider a temporary profile (with no APFT allowed) until the problem is properly evaluated and treated to standard • Exception: If Soldier is at MRDP, then conduct a FFRE to decide P 2 versus P 3 MEB Slide 65
Medical MOS Retention Board (MMRB) to MOS Administrative Retention Review (MAR 2) The MAR 2 program replaced the MOS Medical Retention Board MMRB effective 1 September 2011 UNCLASSIFIED
Profiling 101 Physical Profiling Basics – Profiles & Readiness Slide 67
Profiling 101 Physical Profiling Basics – MRDP Concept • • The Medical Retention Determination Point (MRDP) is agreed to occur when a Soldier’s progress appears to have stabilized, the course of further recovery is relatively predictable, and where it can be reasonably determined that further treatment will not cause the Soldier to meet retention standards or render them capable of performing the duties required by their office, grade, rank or rating. MRDP will be made within one year of being diagnosed with a medical condition that does not appear to meet retention standards, and may be made earlier if the examiner determines that the member will not be capable of returning to duty within one year. The one-year time starts when the injury occurred, or in the case of illnesses, when the diagnosis was first thought to have manifest itself A Soldier that has met MRDP for at least one (1) condition must be sent to the MEB. Other conditions that have not caused the Soldier to meet his or her MRDP on their own will be addressed only to the extent necessary to allow the MEB to decide if the condition/s meet or fail retention standards. Slide 68
Profiling 101 Physical Profiling Basics – MRDP Concept 0 d • • • Point of Injury (POI) or Onset of Illness Focus on establishing diagnosis and treatment 90 -day temporary profile (e. Profile date establishes timeline now) GOAL is RTD Keys to Success: (1) Ensure best clinical care possible; (2) Emphasis on RTD 90 d • • • Re-evaluate SM Focus on treatment; Consider other opinions, consults, etc. Continue 2 nd 90 -day temporary profile GOAL is still RTD Keys to Success: (1) Consideration of all available and appropriate treatment options; (2) Keep unit informed 180 d • • • Re-evaluate SM Continue to focus on treatment but also shift focus to way-ahead and work needed to build IDES case file Continue 3 rd 90 -day temporary profile GOAL is still RTD, but also establish groundwork for possible MRDP; Ascertain stability of secondary diagnoses Keys to Success: (1) Unit cooperation and tracking; (2) Use of VA Checklists to identify IDES requirements 270 d • • • Re-evaluate SM Focus is on completing evaluation of other conditions to be ready for MRDP Continue 4 th (and last) temporary 90 -day profile GOAL is being ready for MRDP at the 365 -day mark Keys to Success: (1) MRDP Coordination; (2) Enhanced access for specialty consults; (3) Engagement with MEB experts 365 d MRDP Slide 69
Select SLIDE MASTER to Insert Briefing Title Here PERIODIC & DEPLOYMENT HEALTH ASSESSMENTS The periodic (PHA) and deployment health assessments (DHA) should be coded with the alphanumeric ICD-9 V code in AHLTA (first diagnosis), not a numeric ICD-9 diagnosis code. PHAs are an ANNUAL requirement (with 3 months leeway until 15 months before the SM goes 'red'). DHAs are associated with deployments and their primary purpose is screening (NOT diagnosis) and identification of conditions for referral and further evaluation (where any 'new' diagnoses may or may not be considered). In the future, as the AMEDD implements improved electronic tracking of referrals from the DHAs and PHA diagnostic codes entered by MEDCOM, FORSCOM, and other healthcare providers become critical for tracking compliance reporting to unit leadership. a. Periodic Health Assessment (PHA): V 70. 5_2 b. Pre-deployment health assessment (DD Form 2795): V 70. 5_D c. Post-deployment heath assessment (DD Form 2796): V 70. 5_E d. Post deployment health re-assessment (DD Form 2900): V 70. 5_F 70 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address COL Bilynsky/DASG-HSZ/703 -681 -0102 / roman. bilynsky@us. army. mil FOUO 02 -Mar-21
Select SLIDE MASTER to Insert Briefing Title Here Overseas Screening • All Soldiers requesting dependent family travel for OCONUS travel (to include Alaska and Hawaii) must have their family member’s medical records screened by the EFMP clinic, IAW AR 608 -75. • Your EFMP OCONUS screen appointment is to ensure that all Family members who will potentially be traveling OCONUS with their sponsor will have access to all required medical and educational needs. Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address COL Bilynsky/DASG-HSZ/703 -681 -0102 / roman. bilynsky@us. army. mil FOUO 02 -Mar-21
Select SLIDE MASTER to Insert Briefing Title Here http: //efmp. amedd. army. mil/ Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address COL Bilynsky/DASG-HSZ/703 -681 -0102 / roman. bilynsky@us. army. mil FOUO 02 -Mar-21