PERIPHERAL ARTERIAL DISEASE Sadie T Velsquez M D












































, blood pressure 106/60 mm")


- Slides: 56
PERIPHERAL ARTERIAL DISEASE Sadie T. Velásquez, M. D.
A 68 -year-old man is evaluated for left calf pain that occurs after walking 2 -3 blocks, relieved with rest; he has had the pain for 6 months. He has a history of CAD with left ventricular systolic function of 30% treated with CABG 2 years ago and implanted cardiac defibrillator placement for primary prevention purposes. PMH: HTN, HLP Social: prior tobacco Meds: atorvastatin, aspirin, metoprolol, lisinopril
A 72 -year-old man is evaluated in the emergency department for acute severe pain during rest in the LLE that began 3 days ago. The patient has repeatedly used vicodin that he had at home for relief of pain. His pain is now much better, but he finds that he is having difficulty walking. + progressive exertional pain in the LLE x 1 year. PMH: HTN, HLP PSH: L fem-pop bypass for occlusive PAD with distal ulceration (5 yrs ago) Social: 50 pack-year tobacco Meds: aspirin, lisinopril, hydrochlorothiazide, simvastatin.
ACC/AHA 2005 GUIDELINES FOR THE MANAGEMENT OF PATIENTS WITH PERIPHERAL ARTERIAL DISEASE (with 2011 Update In Press)
Definitions “Peripheral arterial disease” - vascular diseases caused primarily by atherosclerosis and thromboembolic pathophysiological processes altering normal structure and function of the aorta, its visceral arterial branches, and the arteries of the lower extremity, exclusive of the coronary arteries
Today, we are just going to focus on lower extremity PAD…
Objectives 1. 2. 3. 4. Risks for lower extremity PAD Natural history of atherosclerosis Causes of PAD Clinical presentation of lower extremity PAD 5. Diagnose lower extremity PAD 6. Treatment of PAD
Objectives 1. 2. 3. 4. Risks for lower extremity PAD Natural history of atherosclerosis Causes of PAD Clinical presentation of lower extremity PAD 5. Diagnose lower extremity PAD 6. Treatment of PAD
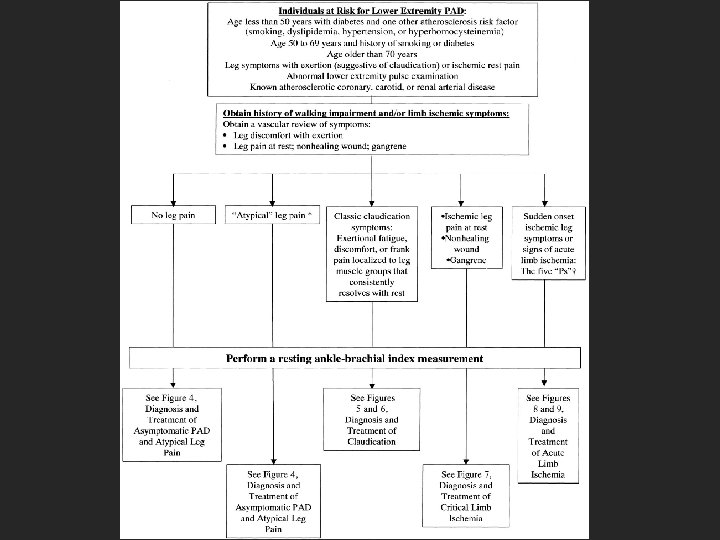
Risk factors • Age < 50 with DM and one other atherosclerosis risk factor • Age >50 years and h/o smoking or DM • Age >65 years • Leg symptoms • Abnormal pulse exam • Known atherosclerotic coronary, carotid or renal artery disease
Risk factors
History and physical Individuals at risk for lower extremity PAD: • Vascular review of symptoms – Exertional limitation of pain – Leg or foot wounds – Rest pain in LE/association with upright or recumbent positions – Postprandial pain provoked by eating and reproducible, weight loss – FH of AAA
Physical exam Vascular physical examination: • Bilateral UE blood pressure • Carotid pulses • Auscultation of the abdomen and flank • Aortic pulsation and its maximal diameter • Palpation of pulses at the brachial, radial, ulnar, femoral, popliteal, dorsalis pedis, and posterior tibial sites
• • • Allen’s test Auscultation of both femoral arteries Pulse intensity Foot inspection Distal hair loss, trophic skin changes, and hypertrophic nails
Why do we even care?
Other causes of PAD • • • Thromboembolic Inflammatory Aneurysmal disease Trauma Entrapment syndromes Congenital abnormalities
Objectives 1. 2. 3. 4. Risks for lower extremity PAD Natural history of atherosclerosis Causes of PAD Clinical presentation of lower extremity PAD 5. Diagnose lower extremity PAD 6. Treatment of PAD
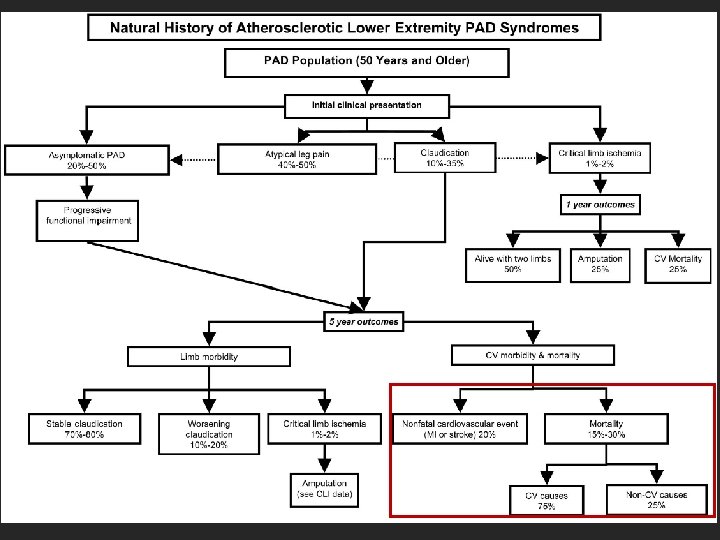
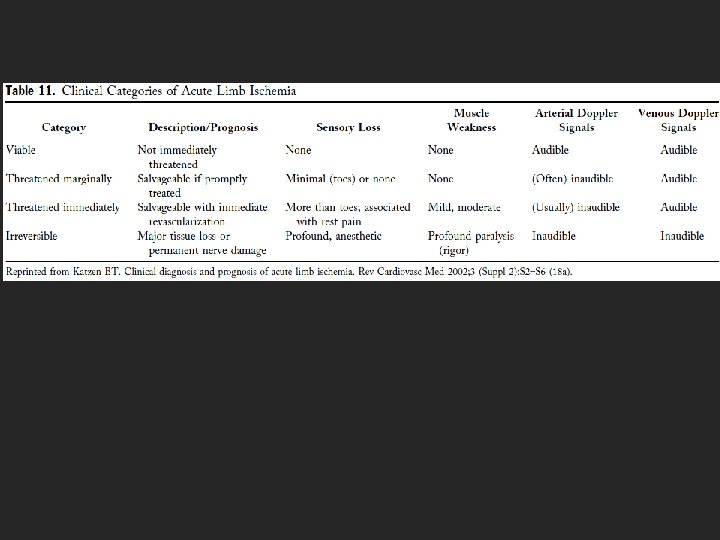
Clinical presentation 1. 2. 3. 4. 5. Asymptomatic Claudication Critical Limb Ischemia Acute Limb Ischemia Prior Limb Arterial Revascularization
Risk factors • Age < 50 with DM and one other atherosclerosis risk factor • Age >50 years and h/o smoking or DM • Age >65 years • Leg symptoms • Abnormal pulse exam • Known atherosclerotic coronary, carotid or renal artery disease
Asymptomatic • Vascular review of systems for those at risk – May have subtle impairments of LE function • Examination and ABI to identify PAD • Exercise ABI if ABI is normal
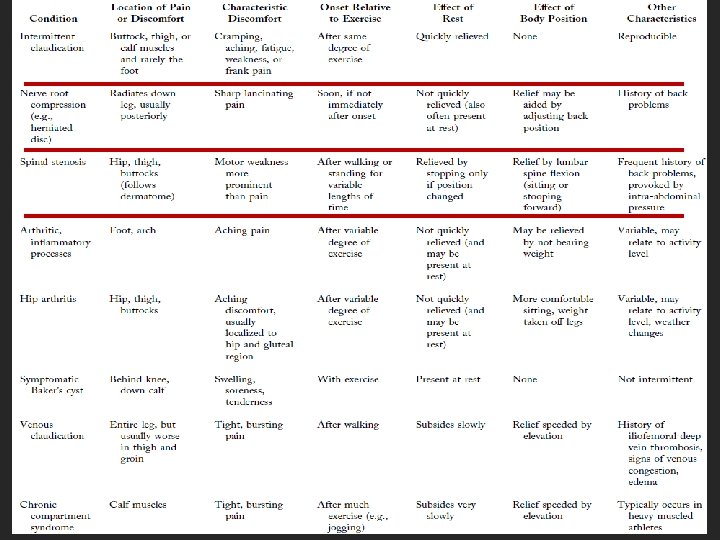
Claudication • Consistently produced by exercise => relieved by rest • Distinguish from ‘pseudoclaudication’ • Vascular physical exam, ABI measurement • Exercise ABI • Comprehensive medical approach
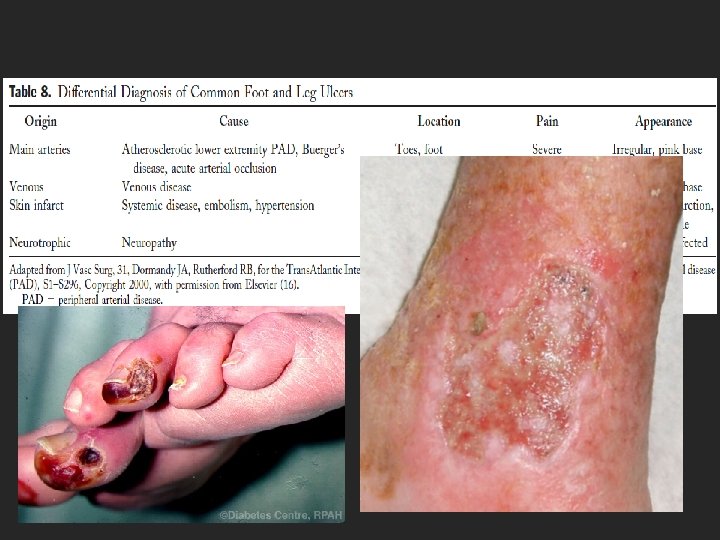
Critical Limb Ischemia • Limb pain at rest +/- trophic skin changes or tissue loss • Discomfort worse supine; less in the dependent position • Require narcotics for pain • Distinguish arterial vs venous or neurotrophic ulcers • CBC, chemistry, EKG and ABI for evaluation
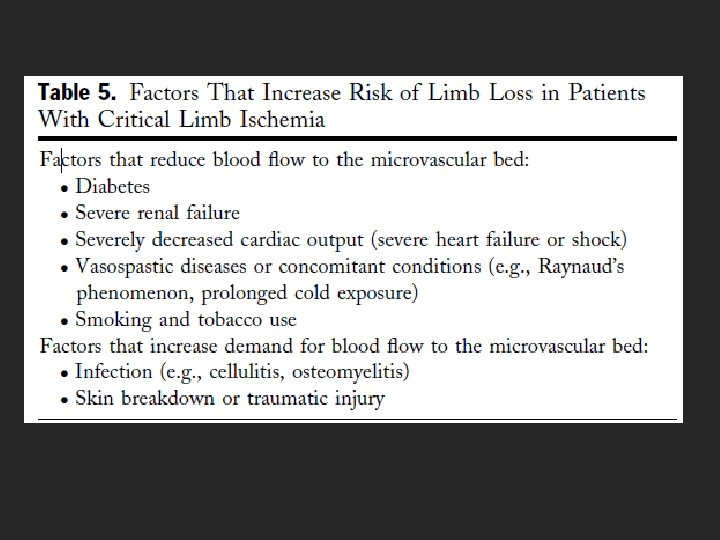
Critical Limb Ischemia • CV risk assessment • Evaluate for aneurysmal disease if suspicious • Systemic antibiotics • Refer to wound specialist Without revascularization, CLI requires amputation within 6 months
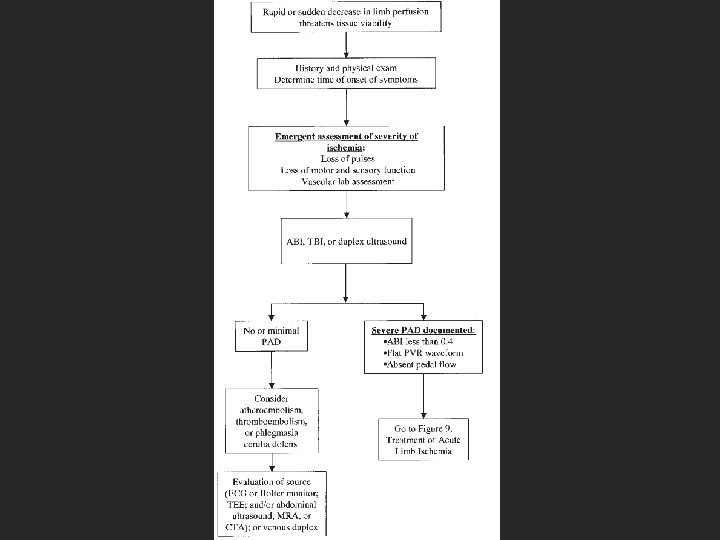
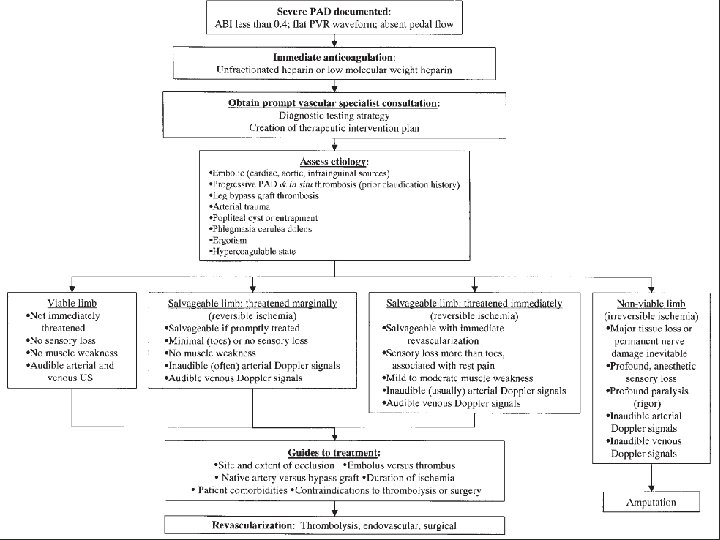
Acute Limb Ischemia • Rapid or sudden decrease in limb perfusion threatening tissue viability • 5 “P’s” – Pain – Paralysis – Paresthesias – Pulselessness – Pallor • 6 th “P”? Polar
Prior Limb Arterial Revascularization • Surveillance program for 2 years: – Interval vascular history – Resting ABIs – PE – Duplex ultrasound if venous conduit used • Timeframe by specialist or bypass type • Angiography if noninvasive methods suggest hemodynamically significant lesions J Vasc Surg, 31, Dormandy JA, Rutherford RB, for the Trans. Atlantic Inter-Society Consensus (TASC) Working Group, Management of peripheral arterial disease (PAD), S 1–S 296, Copyright 2000
Objectives 1. 2. 3. 4. Risks for lower extremity PAD Natural history of atherosclerosis Causes of PAD Clinical presentation of lower extremity PAD 5. Diagnose lower extremity PAD 6. Treatment of PAD
Diagnostic Methods 1. Ankle-Brachial and Toe-Brachial Indices 2. Treadmill Exercise Testing with and without ABI Assessments and 6 -Minute Walk Test 3. Duplex Ultrasound 4. CT Angiography 5. MRI Angiography
6. 7. 8. 9. Contrast Angiography Pulse Volume Recording Segmental pressure examination Continuous-wave Doppler ultrasound
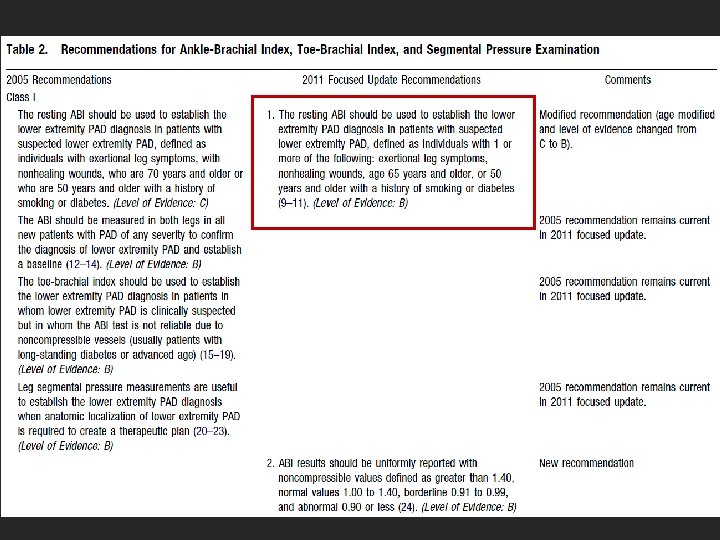
Ankle-Brachial Index • >1. 40: noncompressible • 1. 00 -1. 40: normal • 0. 91 to 0. 99: borderline • < 0. 90: abnormal Mayo Foundation
Ankle-Brachial Index • Patients at risk and those suspected of LE PAD • Bilateral LE • TBI if ABI is not reliable • Leg segmental pressure measurements useful for anatomic localization
Segmental Pressure Measurement
CT Angiography
Owen A R , Roditi G H Postgrad Med J doi: 10. 1136/pgmj. 2009. 082040 Copyright © The Fellowship of Postgraduate Medicine. All rights reserved.
MR angiograms show severe bilateral occlusive PAD below the knee Hodnett P A et al. Radiology 2011; 260: 282 -293 © 2011 by Radiological Society of North America
Primary Cardiology, 2 nd ed. , Braunwald E, Goldman L, eds. , “Recognition and management of peripheral arterial disease, ” Hirsch AT, 659– 71, Philadelphia, PA: WB Saunders.
Objectives 1. 2. 3. 4. Risks for lower extremity PAD Natural history of atherosclerosis Causes of PAD Clinical presentation of lower extremity PAD 5. Diagnose lower extremity PAD 6. Treatment of PAD
Treatment • Cardiovascular Risk Reduction • Claudication • Critical Limb Ischemia and Treatment for Limb Salvage
CV Risk Reduction • • • Lipid-lowering Drugs Antihypertensive Drugs DM Therapies Smoking Cessation * Homocysteine-Lowering Drugs Antiplatelet and Antithrombotic Drugs
Smoking Cessation • Ask about smoking status at every visit • Provide counseling and development smoking cessation plan • Pharmacotherapy should be offered to all smokers
Claudication • Exercise and LE PAD Rehabilitation • Medical and Pharmacologic Treatment for Claudication – Cilostazol – Pentoxifylline • Endovascular Treatment for Claudication • Surgery
Critical Limb Ischemia and Treatment for Limb Salvage • Prostaglandins may be considered • Endovascular treatment • Thrombolysis for acute and chronic limb ischemia • Surgery
Questions A 68 -year-old man is evaluated for left calf pain that occurs after walking 2 -3 blocks, relieved with rest; he has had the pain for 6 months. He has a history of CAD with left ventricular systolic function of 30% treated with CABG 2 years ago and implanted cardiac defibrillator placement for primary prevention purposes. PMH: HTN, HLP Social: prior tobacco Meds: atorvastatin, aspirin, metoprolol, lisinopril.
Physical examination: blood pressure 110/70 mm Hg, pulse 68/min and regular, respiration rate 16/min. Peripheral pulses are diminished. There is no skin breakdown or ulceration and no abdominal or femoral bruits. Ankle-brachial index is 0. 7 on the left and 1. 0 on the right. Segmental plethysmography demonstrates a pressure drop of 20 mm Hg below the left knee.
Which of the following is the most appropriate treatment for this patient? A. Femoral-popliteal bypass B. Medical treatment with cilostazol C. Percutaneous intervention D. Supervised exercise program
A 72 -year-old man is evaluated in the emergency department for acute severe pain during rest in the LLE that began 3 days ago. The patient has repeatedly used vicodin that he had at home for relief of pain. His pain is now much better, but he finds that he is having difficulty walking. + progressive exertional pain in the LLE x 1 year. PMH: HTN, HLP PSH: L fem-pop bypass for occlusive PAD with distal ulceration (5 yrs ago) Social: 50 pack-year tobacco Meds: aspirin, lisinopril, hydrochlorothiazide, simvastatin.
Physical examination: temperature is 37. 8 °C (100. 1 °F), blood pressure 106/60 mm Hg, pulse 100/min, respiration rate is 20/min. Left lower extremity is pale and cool from the toes to the mid shin, and there is a small ulceration on the ball of the left foot. The left posterior tibialis and dorsalis pedis pulses are not palpable and cannot be identified by Doppler ultrasonography. Venous Doppler signals are audible. The left foot and calf feel stiff, and the patient can only weakly flex the foot. Toe movement on the left side is minimal, and sensation to light touch is absent.
Which of the following is the most appropriate treatment for this patient? A. Emergent surgical revascularization B. Intravenous heparin C. Intra-arterial thrombolytic therapy D. Prompt amputation
References • MKSAP • ACC/AHA 2005 Guidelines for the Management of Patients With Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic): Executive Summary. • Rooke et al. 2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (Updating the 2005 Guideline). J. Am. Coll. Cardiol. published online Sep 29, 2011. In Press.