ORAL CANCER What is cancer What is oral









")










 – Well differentiated squamous cell carcinoma with keratin")

 INVOLVES THREE PARAMETERS")





 Site- Intraoral Ca categorized into different anatomical sites S 1 :")
 Tumour T 1 : Less than 2 cm T 2 : More than")

 Nodal Involvement N 0 : No palpable nodes N 1 : Epithelial node")
 Nodal Involvement N 0 : No palpable nodes N 1 : Epithelial node")








Intraoral approach B)extraoral Segmental")









 Brachytherapy –")
 Locally advanced lesions (T 3, T")







- Slides: 72
ORAL CANCER
What is cancer What is oral cancer Etiology Tumurogensis Presentation Diagnosis Staging Treating options
POTENTIALLY LIFE THREATENING CONDITION DISFIGUREMENT OF THE FACE FUNCTIONAL INHIBITIONS DIFFICULT TO TREAT
Neoplasia : “is an abnormal mass of tissue the growth of which exceeds and is un coordinated with that of the normal tissues and persists in the same excessive manner even after the cessation of the stimuli which evoked the change”. Willis
Sites Oral cavity extends from the skin-vermillion junction of the lips to the junction of soft and hard palate above and to the line of circumvallate papillae on the tongue below Divided into specific sites – Lip Buccal mucosa Lower alveolus Upper alveolus Retromolar region Floor of the mouth Hard palate Anterior 2/3 rd of tongue
Epidemiology Incidence – oral cancer is one of the 10 leading cancers in the world Histological types �Squamous cell carcinoma – 90. 6% �Verrucous carcinoma – 6% �Others – 5% Sites – � Buccal mucosa - 70% �Alveolus – 20% �Tongue – 7% �Floor of mouth – 5% �Lip – 2%
Age- 90% in persons above 40 years M: F – 7: 3 Stage at presentation 65% - stage 3 75% - had lymph node metastases
Aetiology 1. Tobacco Smoking Chewing Arecanut chewing without tobacco Mixed habit of chewing and smoking 2. Alcohol
Aetiology Others 3. Syphilis 4. Orodental factors 5. Diet & deficiency states 6. Candida infections 7. Viruses 8. Sunlight
Etiology Tobacco Alcohol Malnutrition Trauma Immune deficiencies Candidiasis Viruses Sunlight (actinic radiation)
Clinical evaluation & diagnosis Non-healing ulcers, white or red patches – early symptoms. Ulceroproliferative growth covered with slough, indurated base and everted margins. Pain, bleeding, difficulty in swallowing, speech defect, trismus, lump in the neck – late symptoms.
Intra-oral examination Growth Endophytic Exophytic Ulcer and white patches Number, site, extent, shape, size, margins, floor & base, degree of soft tissue, bone and skin involvement, surrounding induration Degree of mouth opening, restriction of tongue movements Confirmation – incisional biopsy/bone biopsy
How do they look ?
Neck examination Thorough examination for palpable lymphnodes in the neck should be made Check for size, shape, tenderness, consistency, mobility/fixity FNAC of suspected lymphnodes
Spread of tumor Local spread Regional spread Distant spread
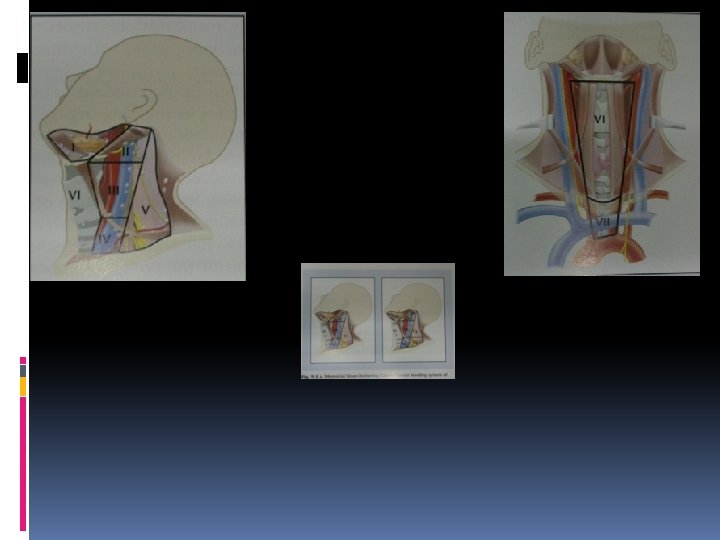
Lymphatics of oral cavity Level 1 – submental and submandibular groups Level 2 – upper deep cervical groups along the upper 1/3 rd of I. J. V. Level 3 – mid-deep cervical lymphnodes along the middle 1/3 rd of I. J. V. extending upto superior belly of omohyoid muscle Level 4 – the lower deep cervical lymphnodes along I. J. V. from superior belly of omohyoid Level 5 – Lymphnodes in the postrior triangle of the neck mainly along the spinal acc. n
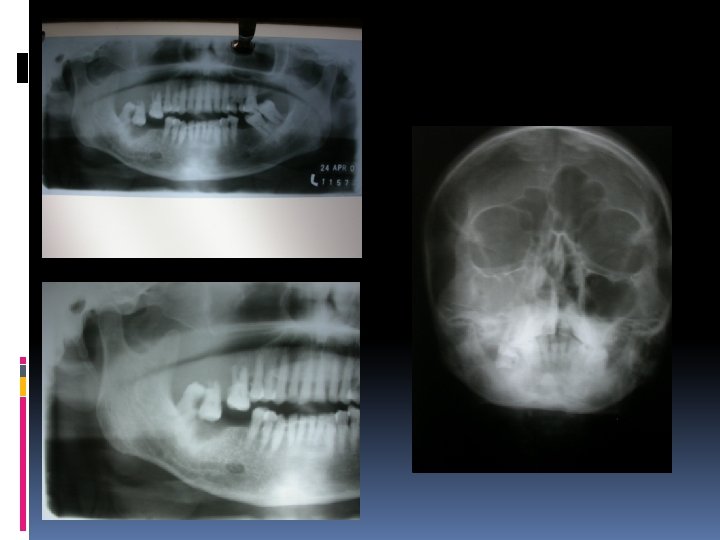
Imaging PA Mandible, Opg, Occlusal, PNS CT-Scan MRI Radio-nuclide scanning Chest PA
DIAGNOSIS FULL HISTORY PROPER DESCRIPTION OF THE LESION DIAGRAMMATIC ORIENTATION OF THE SPECIMEN RELEVANT RADIOGRAPHS PREVIOUS LABORATORY REPORTS IF ANY BIOPSY OF THE LESION PROVISIONAL DIAGNOSIS Findings recorded to be confirmed with the help of Biopsy
Most intraoral lesions (80 -90%) – Well differentiated squamous cell carcinoma with keratin formation INDURATION OF SURROUNDING TISSUES INDICATES NEOPLASTIC INFILTRATION REGIONAL SPREAD OCCURS ALONG Ø LYMPHATICS Ø NEUROVASCULAR CANAL OF THE MANDIBLE
STAGING EFFECTIVE PROGNOSTIC INDICATOR ACCURATELY DESCRIBES THE TUMOUR WIDELY USED METHOD IS TNM SYSTEM OFFERS TO CATEGORIZE DESCRIPTION OF LESION TO FACILITATE TREATMENT PLANNING TO COMPARE VARIOUS MODALITIES OF TREATMENT PREDICT PROGNOSIS
TNM CLASSIFICATION STAGING GIVEN BY AMERICAN JOINT COm. MITTE ON CANCER(AJCC) INVOLVES THREE PARAMETERS T INDICATES TUMOUR SIZE AND INVASION N INDICATES PRESENCE OR ABSENCE OF LYMPH NODES M INDICATES PRESENCE OR ABSENCE OF METASTASIS
TX PRIMARY TUMOUR CANNOT BE ASSESSED T 0 THERE IS NO EVIDENCE OF PRIMARY TUMOUR Tis CARCINOMA IN SITU T 1 TUMOUR IS 2 CM OR LESS IN GREATEST DIMENSION T 2 TUMOUR IS MORE THAN 2 CM BUT NOT GREATER THAN 4 CM GREATEST DIMENSION IN T 3 TUMOUR IS MORE THAN 4 CM IN GREATEST DIMENSION T 4 TUMOUR INVADES THROUGH CORTICAL BONE, INFERIOR ALVEOLAR NERVE, FLOOR OF MOUTH, OR SKIN OF FACE-i. e OR NOSE T 4 a TUMOUR INVADES ADJACENT STRUCTURES(e. g. , THROUGH CORTICAL BONE, INTO DEEP[EXTRINSIC] MUSCLE OF TONGUE[GENIOGLOSSUS, HYOGLOSSUS, PALATOGLOSSUS, STYLOGLOSSUS], MAXILLARY SINUS, SKIN OF FACE) T 4 b TUMOUR INVADES MASTICATOR SPACE, PTERYGOID PLATES, OR SKULL BASE AND/OR ENCASES THE INTERNAL CAROTID ARTERY CHIN
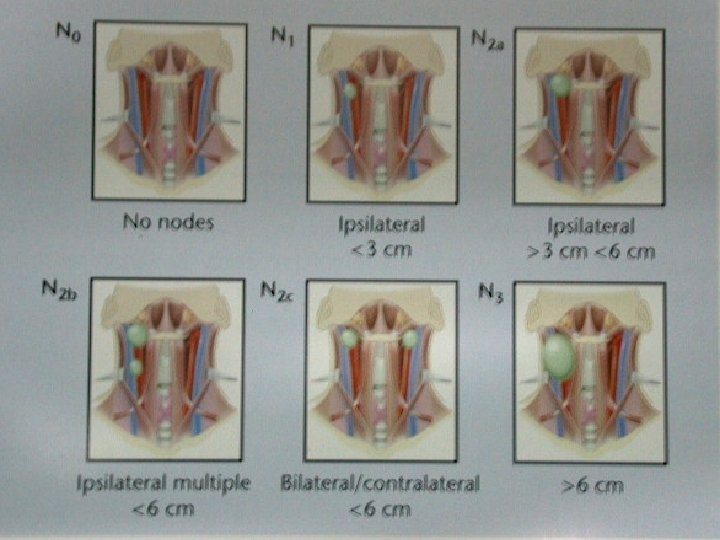
NX REGIONAL LYMPH NODES CANNOT BE ASSESSED N 0 THERE IS NO REGIONAL NODES METASTASIS N 1 METASTASIS IS IN A SINGLE IPSILATERAL LYMPH NODE, 3 CM LESS IN GREATEST DIMENSION OR N 2 METASTASIS IS IN A SINGLE IPSILATERAL LYMPH NODE, MORE THAN 3 CM BUT NOT MORE THAN 6 CM IN GREATEST DIMENSION; OR METASTASIS IS IN MULTIPLE IPSILATERAL NODES, NONE MORE THAN 6 CM IN GREATEST DIMENSION; OR METASTASIS IS IN BILATERAL OR CONTRALATERAL LYMPH NODES, NONE GREATER THAN 6 CM IN GREATEST DIMENSION N 2 a METASTASIS IS IN A SINGLE IPSILATERAL LYMPH NODE, MORE THAN 3 CM BUT NOT MORE THAN 6 CM IN GREATEST DIMENSION N 2 b METASTASIS IS IN MULTIPLE IPSILATERAL LYMPH MORE THAN 6 CM IN GREATEST DIMENSION NODES, NONE N 2 c METASTASIS IS IN BILATERAL OR CONTRALATERAL LYMPH NODES, NONE MORE THAN 6 CM IN GREATEST DIMENSION N 3 METASTASIS IS IN A LUMPH NODE MORE THAN 6 CM IN GREATEST DIMENSION
MX DISTANT METASTASIS CANNOT BE ASSESSED M 0 THERE IS NO DISTANT METASTASIS M 1 THERE IS DISTANT METASTASIS
STAGE GROUPING STAGE 0 STAGE III STAGE IVA STAGE IVB STAGE IVC Tis T 1 T 2 T 3 T 4 a T 4 b ANY T N 0 N 0 N 1 N 1 N 0 N 1 N 2 N 2 ANY N M 0 N 3 ANY N M 1 M 0 M 0 M 0 M 0
PROGNOSTIC INDICATORS WIDELY USED METHOD OF STAGING IS TNM TO EVALUATE PROGNOSTIC INDICATORS IT WAS EXTENDED TO STNMP “S” REFERS TO SITE OF THE LESION “P” REFERS TO HISTOPATHOLOGY
STNMP Staging (s) Site- Intraoral Ca categorized into different anatomical sites S 1 : lip skin S 2 : Lip mucous membrane S 3 : Tongue S 4 : Cheek S 5 : Palate S 6 : Floor of mouth S 7 : Alveolar process S 8 : Maxillary antrum S 9 : Central Ca of bone
(T) Tumour T 1 : Less than 2 cm T 2 : More than 2 but less than 4 cm T 3 : More than 2 but less than 6 cm and extending beyond the primary region T 4 : More than 6 cm snd extend to involve adjacent structures
Based on presence or absence of residual tumours after treatment: ‘R’ was introduced (R) Residual Tumour Rx : Presence of residual tumour cannot be assessed R 0 : No residual tumour R 1 : Microscopic residual tumour R 2 : Macroscopic residual tumour
(N) Nodal Involvement N 0 : No palpable nodes N 1 : Epithelial node enlargement N 2 : Clinically palpable homolateral regional node not fixed N 3 : Same as N 2 but fixed N 4 : Clinically palpable contra lateral or bilateral node not fixed N 5 : Same as N 4 but fixed (M) Distant Metastasis Mx : Distant mtastasis cannot be assessed M 1 : No distant metastasis M 2 : Distant metastasis
(N) Nodal Involvement N 0 : No palpable nodes N 1 : Epithelial node enlargement N 2 : Clinically palpable homolateral regional node not fixed N 3 : Same as N 2 but fixed N 4 : Clinically palpable contra lateral or bilateral node not fixed N 5 : Same as N 4 but fixed (M) Distant Metastasis Mx : Distant mtastasis cannot be assessed M 1 : No distant metastasis M 2 : Distant metastasis
Pathology P 0 : Hyperkeratotic Lesion showing atypia P 1 : Carcinoma insitu P 2 : Basal cell carcinoma P 3 a : Verrucous Carcinoma P 3 b : Well differentiated SCC P 3 c : Moderately differentiated SCC P 3 d : Poorly differentiated SCC
Differentiation Well differentiated. Moderately differentiated. Poorly differentiated. Squamous cell carcinoma Verrucous Carcinoma
Management Surgery Radiotherapy Chemotherapy Combination of above Palliative treatment
PRINCIPLES OF MANAGEMENT OF ORAL CANCER IS A TEAM APPROACH WHICH INVOLVES GENERAL SURGEON ORAL SURGEON RADIOTHERAPIST CHEMOTHERAPIST
MODALITIES OF TREATMENT AVAILABLE SURGERY IRRADIATION CHEMOTHERAPY ELECTROCOAGULATION CRYOSURGERY LASER VAPORIZATION ANY COMBINATION OF THESE METHODS
CHOICE OF TREATMENT DEPENDS ON THE FOLLOWING FACTORS EXTENT OF THE LESION INVOLVEMENT OF BONE EXTENSION/INFILTRATION INTO THE UNDERLYING TISSUES INCLUDING MUSCLES OF MASTICATION STATUS OF DENTITION HISTOPATHOLOGY AND STAGING PREVIOUS TREATMENT, IF ANY AVAILABILITY OF EXPERTISE AND FACILITIES GENERAL HEALTH OF THE PATIENT
SURGICAL THERAPY GOAL IS COMPLETE REMOVAL OF PRIMARY TUMOUR WITH ADEQUATE MARGIN ALONG WITH REGIONAL LYMPH NODES, DEPENDING ON THEIR INVOLVEMENT IN S. C. C SURGERY IS PRIMARY MODE OF TREATMENT IF BONE IS INVOLVED THEN SURGERY IS THE TREATMENT OF CHOICE
Surgery is carried out depending on variable factors 1. Size and location of tumor 2. Duration 3. Benign vs malignant Histopathological study- i)well differentiated ii)moderately iii) poorly 4. Invasion into bone 5. Diagnosis
Different surgical procedures done are Curettage En-bloc marginal madibular resection A)Intraoral approach B)extraoral Segmental mandibularresection (partial mandibular resection, hemimandibulectomy) 6. Partial /Subtotal maxillectomy 7. Maxillectomy 1. 2. 3. 4. 5.
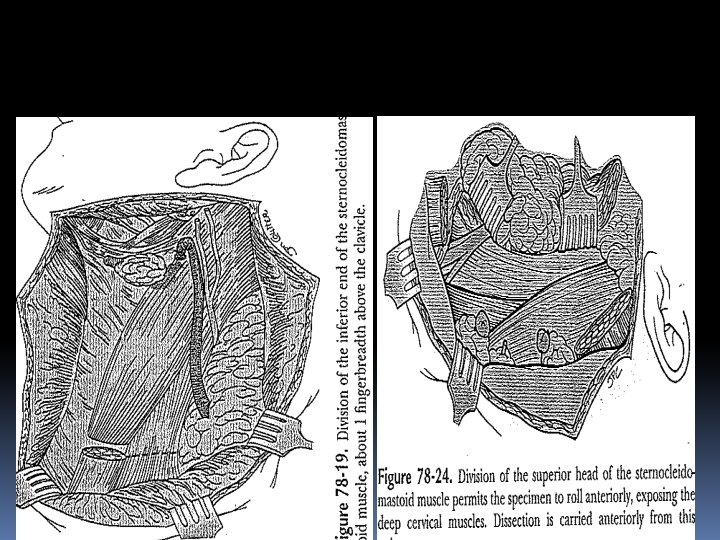
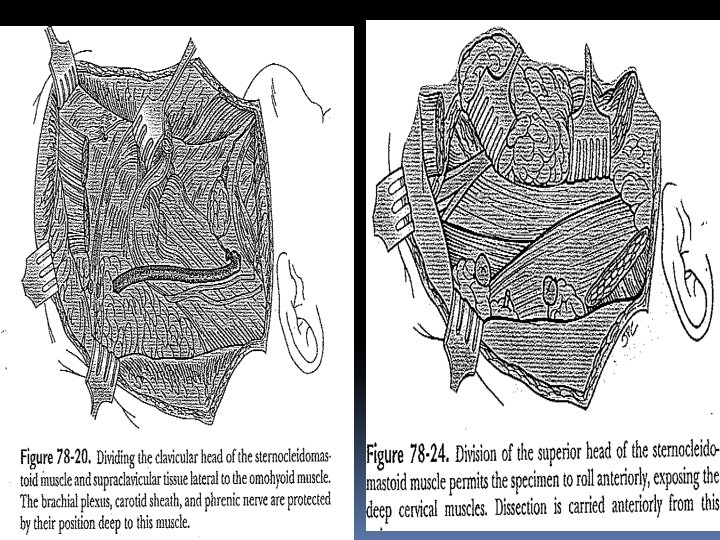
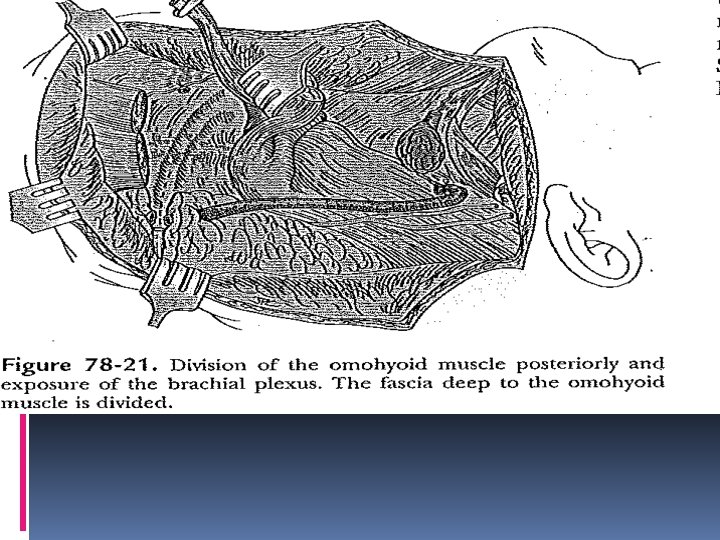
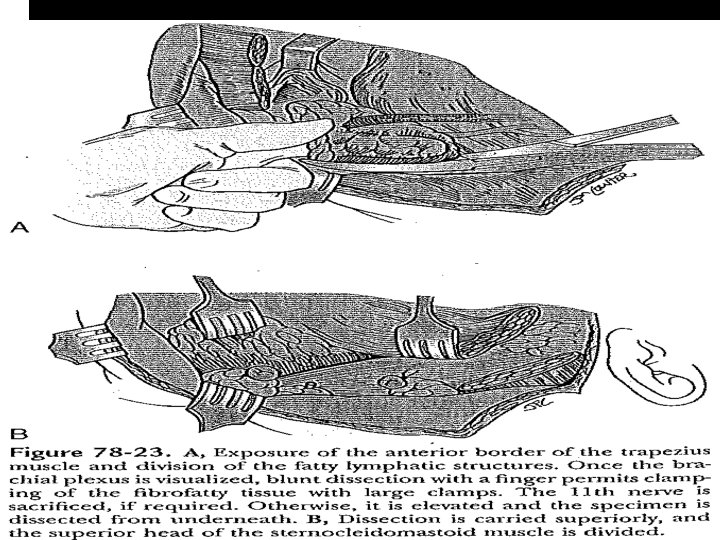
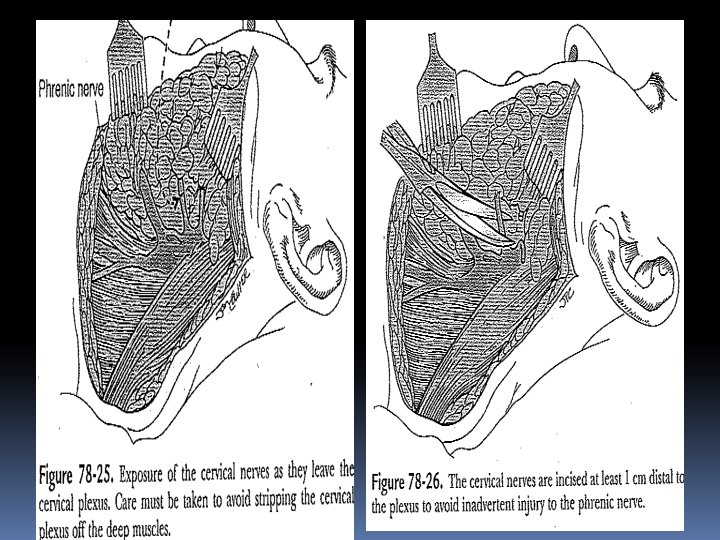
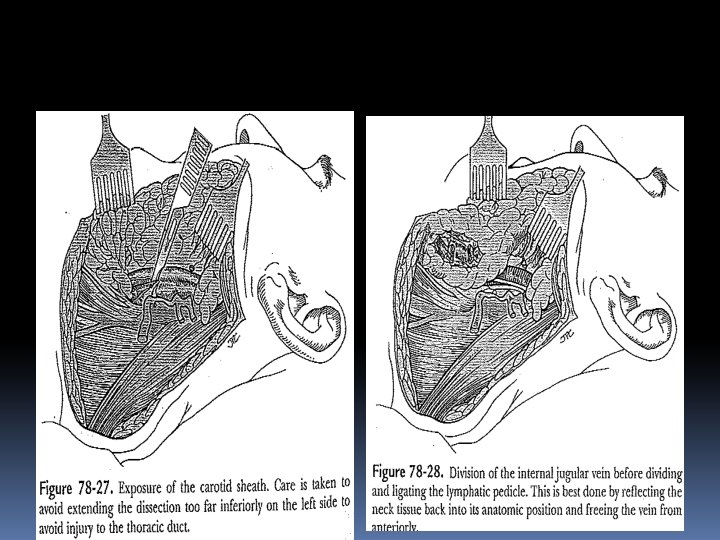
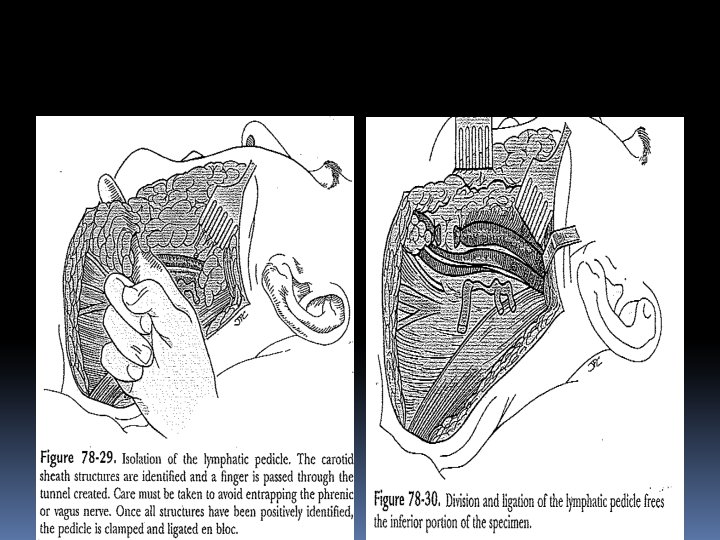
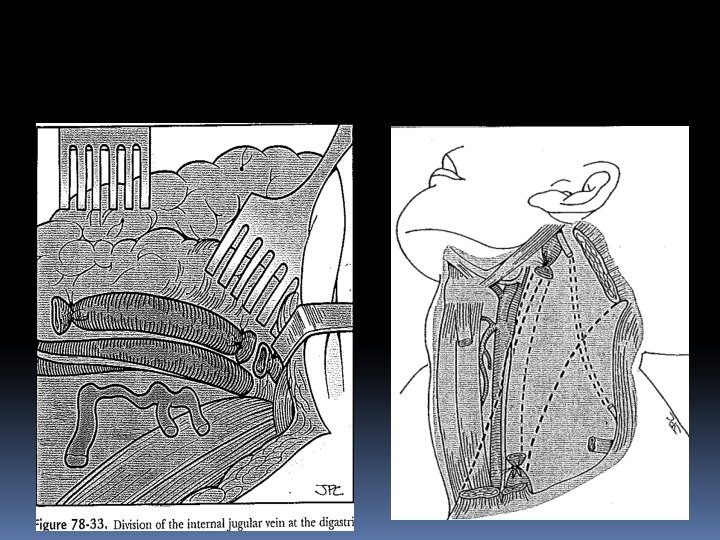
NECK DISSECTION RECONSTRUCTION MANAGEMENT OF PAIN
IN CASE OF EXTENSIVELY INVOLVED LYMPH NODES NECK DISSECTION IS INDICATED LYMPH NODES IN THE NECK ARE CLASSIFIED AS LEVELS I TO VII LEVEL IA SUBMENTAL GROUP LEVEL IB SUBMANDIBULAR GROUP LEVEL II UPPER JUGULAR GROUP LEVEL III MID-JUGULAR GROUP LEVEL IV LOWER JUGULAR GROUP LEVEL V POSTERIOR TRIANGLE GROUP LEVEL VI CENTRAL COMPARTMENT GROUP LEVEL VII SUPERIOR MEDIASTINAL GROUP
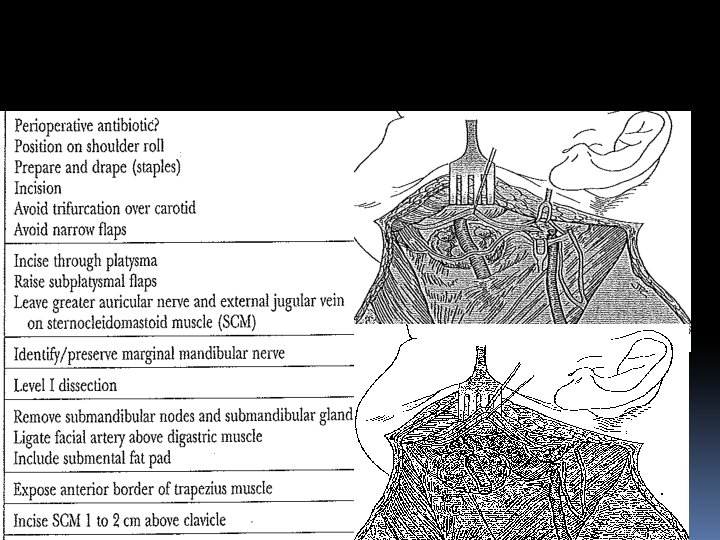
INCISIONS
RND
MRND TYPE I SPINAL ACESSORY NERVE PRESERVED
MRND TYPE II Spinal acessory nerve and IJV preserved
MRND TYPE III All 3 structures preserved
Supraomohyoid neck dissection
RADIOTHERAPY DESTROYS CELLS BY IONIZATION AIM IS TO GIVE MAXIMUM DOSE THAT NORMAL TISSUES CAN TOLERATE SO THAT CHANCES OF KILLING MALIGNANT CELLS ARE MORE TWO PRINCIPAL FORMS OF RADIOTHERAPY �EXTERNAL BEAM MEGAVOLTAGE THERAPY �INTERSTITIAL TECHNIQUES
Tele-radiation – external beam of X-rays/Gamma rays (cobalt 60, caesium 137) Brachytherapy – internally implanted sources of gamma rays (irridium 191, iodine 125) Daily dose of 2 grays (1 gray=100 rads) , 5 days a week for 6 weeks Fractionization – allows repair of cellular injury, repopulation by surviving viable cells, redistribution within the division cycle and re-oxygenation of tumor
Post-operative radiation therapy Positive cut margins (frozen section) Locally advanced lesions (T 3, T 4) High grade anaplastic lesions Peri-neural invasion Multiple lymphnode metastases Extracapsular spread
CHEMOTHERAPY USED AS AN ADVUVANT TO SURGERY OR RADIOTHERAPY OR AS A SINGLE AGENT ACTIVE CHEMOTHERAPEUTIC AGENTS CISPLATINUM BLEOMYCIN 5 -FLUOROURACIL METHOTREXATE
Chemotherapeutic agents Cis-platin 5 -fluorouracil Methotrexate Bleomycin -Interferon
Hazards of therapies. Mucosities. Xerostomia. Trismus. Radiation caries. Fibrosis of the tissues. Osteoradionecrosis. Alopasia. Immune suppression. Anorexia.
Immunotherapy Inhibition of tumour cell growth can occur on attaching a specific monoclonal antibody to a suitable white cell. Antibodies on the tumour specific killer cells thus produced react with target tumour cell antigen , destroying the tumour cell.
Rehabilitation Restoration of appearance and function obturators/feeding plates, partial dentures, implants Jaw physiotherapy Speech therapy Nutritional support Counseling
PREVENTION ABUSE OF TOBACCO IN ALL FORMS TO BE AVOIDED WHENEVER AN ULCER OR WOUND OR SWELLING IN ORAL CAVITY DOES NOT RESPOND IN 2 -3 WEEKS IT SHOULD BE FULLY INVESTIGATED PUBLIC MOTIVATION AVOID PAN CHEWING MASS SCREENING OF POPULATION
Prognosis Disease free life ? 5 year survival rate. Eventual recurrence and death !!!