The Epidemiology of Head and Neck Cancer Scott
 Doctoral Candidate June")
 • Head & neck cancer refers to")




")


 • Cervical nodal involvement is one")


: 1429 -35")

 • IARC classifies consumption of alcoholic beverages as causal for SCCHN")


 • 25% of SCCHN associated w/ HPV – 45 -60% of")



")
 • Arise from the epithelial lining of the nasal cavity/nasopharynx •")

")



 – Local: 80 -90%")
 & NPC • Member of the herpesvirus family • Transmitted chiefly")


 • Associated with")


 • Prior hx of chronic")






 • • Most common: 30 -35% of salivary tumors Usually involves")

 • 2 nd most common salivary cancer • Occurs in")


: – Basal cell adenocarcinoma – Clear")



- Slides: 54
The Epidemiology of Head and Neck Cancer Scott Langevin, MHA CT(ASCP) Doctoral Candidate June 5, 2009
Anatomy of the Upper Aerodigestive Tract (UADT) • Head & neck cancer refers to cancers of the UADT: – – – – Oral Cavity Pharynx Hypopharynx Larynx Nasopharynx Nasal cavity Paranasal sinuses Source: http: //utahhealthsciences. net/customer/image_gallery/332/ENT_drawing. jpg
Epidemiology • Head and neck cancer in the US, 2008: – 47, 560 new cases (3. 3% of US cancers) – 9 th most common cancer – 11, 260 deaths (2% of US cancer deaths) – 14 th most common cause of cancer death • Globally, head and neck cancer results in: – 563, 826 new cases (5. 2% of world cancers) – 301, 408 deaths (4. 5% of world cancer deaths
Survival • 60% overall 5 -year survival – Virtually unchanged over past 3 decades – Varies by site Site Lip Oral Cavity Oropharynx Hypopharynx Larynx Percent 5 -Year Survival Overall Local Regional Distant 85. 6 89. 6 82. 7 40. 0 56. 7 72. 0 43. 8 35. 2 50. 6 61. 0 50. 6 30. 2 33. 3 56. 0 34. 6 12. 9 62. 0 74. 3 53. 2 38. 3 Source: Carvalho et al. Trends in incidence and prognosis for head and neck cancer in the United States: a site specific analysis of the SEER database. 2005.
Stage at diagnosis by site 90. 0 80. 0 70. 0 Local 60. 0 Regional 50. 0 Distant 40. 0 30. 0 20. 0 10. 0 Larynx Hypopharynx Oral Cavity Lip 0. 0
Common Types of Head & Neck Cancer • Head and neck cancer is a heterogeneous category of malignancies • 90 -93% are head and neck squamous cell carcinomas (SCCHN) • 3 -6% are nasopharyngeal carcinomas (NPC) • 1 -3% are salivary cancers
Squamous Cell Carcinoma of the Head and Neck (SCCHN)
Clinical Presentation & Treatment • Currently no proven screening method except visual examination • Symptoms: hoarseness, dysphagia, odynophagia, ulcerations, bleeding • 1 st line treatment modalities: – Early stage: surgery (preferred) or radiation – Advanced stage: typically surgery + chemoradiation • Currently Cisplatin is treatment of choice, alone or in combination • EGFR inhibitors are in trials (cetuximab)
Epidemiology • 93% of head and neck cancers are SCCHN • Median age at diagnosis = 62 years – Although, incidence in adults < 45 increasing • Particularly for base of tongue and tonsillar SCC • Men are 2. 78 times as likely to develop SCCHN – 2. 59 times as likely to die from it • Higher incidence in African-Americans – Poorer 5 -year survival (16 -20% lower)
Prognostic Indicators • TNM stage (higher = worse) • Cervical nodal involvement is one of the strongest predictors (50% reduction in survival) – 2/3 SCCHN patients present with cervical mets – 10% present with distant mets – Extracapsular spread (ECS) further reduces survival • Other predictors – – – Nodal burden Perineural invasion Histologic grade Extent of necrosis Positive tumor margins
Recurrence and Second Primaries • > 50% of patients with locally advanced SCCHN experience recurrence within 2 years • 2 nd primaries occur in 15% of SCCHN patients at a rate of 3 -5% per year • Tumor recurrence or development of a second primary is a major reason for treatment failure and adversely impacts long-term survival
Tobacco • IARC classifies cigarette smoking as a Group 1 carcinogen and a causal factor for SCCHN • Linear dose-response for smoking & SCCHN – Duration > intensity, although both matter – 3 - to 10 -fold increase in risk for smokers vs. nonsmokers – 5 - to 25 -fold increase in risk for heavy smokers vs nonsmokers • Other forms of tobacco are also associated with SCCHN (pipe, cigar, chew) • Tobacco use also associated with 2 nd primary SCCHN
Source: Sturgis et al. Cancer. 2007. 110(7): 1429 -35
Carcinogenic Effect of Tobacco • > 60 carcinogens identified in tobacco smoke • Polycyclic aromatic hydrocarbons (PAH) are most potent in burnt tobacco • Nitrosamines and their metabolites are most potent in smokeless tobacco • Main effect is via DNA adduct formation -> mutations
Alcohol (Et. OH) • IARC classifies consumption of alcoholic beverages as causal for SCCHN • Contributive factor in ~75% of SCCHN • Dose-response effect – 50 g Et. OH/day is associated w/ 2 - to 3 -fold increased risk relative to non-drinkers – Heavy drinkers (> 100 g/day) = 4 - to 6. 5 -fold increase compared w/ non-drinkers • Also associated w/ 2 nd primary SCCHN
Carcinogenic Effect of Et. OH • Main effect derived from acetaldehyde, the primary metabolite – Forms DNA adducts and interferes w/ DNA synthesis and repair – High levels of acetaldehyde in saliva of alcoholics w/ SCCHN • Et. OH metabolized by bacterial enzymes – Poor oral health = increased acetaldehyde levels
Cigarette & Et. OH Synergy • There is an interaction between Et. OH and smoking, as it relates to SCCHN – The combined effect is multiplicative of the individual effects alone • Combined use accounts for 73% of SCCHN • Et. OH acts as a solvent for tobacco carcinogens • Smoking results in a shift in oral flora leading to increased acetaldehyde concentrations
Human Papillomavirus (HPV) • 25% of SCCHN associated w/ HPV – 45 -60% of oropharyngeal tumors, especially palatine and lingual tonsils • In contrast, 10% HPV+ in normal OP mucosa • 90 -95% of HPV+ tumors are HPV 16+ • HPV positive tumors represent a distinct clinical subset of tumors – Patients are younger, less likely to smoke/drink – Tumors are more likely basaloid and poorly diff – Better prognosis
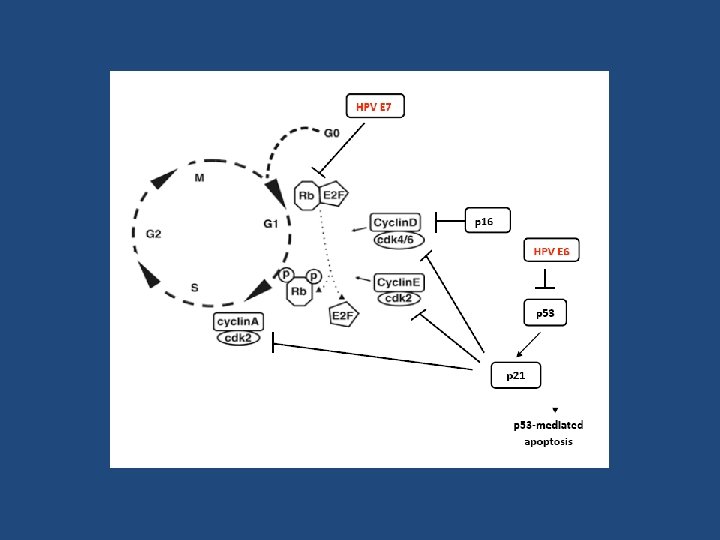
HPV Oncogenic Effect • Primarily stems from action of E 6 & E 7 viral oncoproteins – E 6 binds and inactivates p 53 tumor suppressor • Loss of p 53 mediated apoptosis – E 7 binds and inactivates p. Rb tumor suppressor • Loss of G 1 -S phase checkpoint • p 16 overexpression is a surrogate marker for HPV-mediated SCCHN
Other Risk Factors • Environmental/Occupational – Indoor air pollution • Wood smoke or heating/cooking with fossil fuels – Chronic second-hand tobacco smoke exposure • 1. 5 - to 5 -fold increase in risk – Metal working – Exposure to toxins during mustard gas production • Diet – High in animal fat, low in fruits and vegetables associated w/ increased risk of SCCHN – Low folate intake may also be associated • Gastroesophageal reflux
Field Cancerization • The epithelium is chronically exposed to environmental carcinogens – Particularly true of smokers/drinkers • Mutations that confer a growth/survival advantage are clonally selected – Gradually replace normal epithelium – New mutations occur within these fields giving rise to subclones; eventually can become malignant – Can give rise to distinct but clonally related tumors – Evidenced by mutations/alterations in “negative” margins • This helps explain high recurrence/second primary rate of SCCHN
Nasopharyngeal Carcinoma (NPC)
Nasopharyngeal Carcinoma (NPC) • Arise from the epithelial lining of the nasal cavity/nasopharynx • Results from the interplay of environmental, genetic and viral risk factors • 70 -75% present with ear & nasal symptoms • 75% present with painless, enlarged cervical nodes
Treatment • Radiation or chemoradiation is typically the 1 st line of therapy – NPC is radiosensitive – Difficult to operate on nasopharynx • thus surgery is not generally used as 1 st line therapy for primary tumor – Surgery is used to remove cervical nodes with metastatic disease
NPC Classification • WHO classifies NPC into 3 types: 1. Keratinizing SCC (type I) 1. • • Believed to be of a distinct etiology from types II & III Dominant type in low incident regions 39. 4% of US NPC 2. Non-keratinizing SCC (type II) • • 5% of high-incident regions 25. 0% of US NPC 3. Undifferentiated SCC (type III) • • 95% of high incident regions 14. 0% of US NPC * 21. 6% of US NPC are diagnosed as Carcinoma, NOS
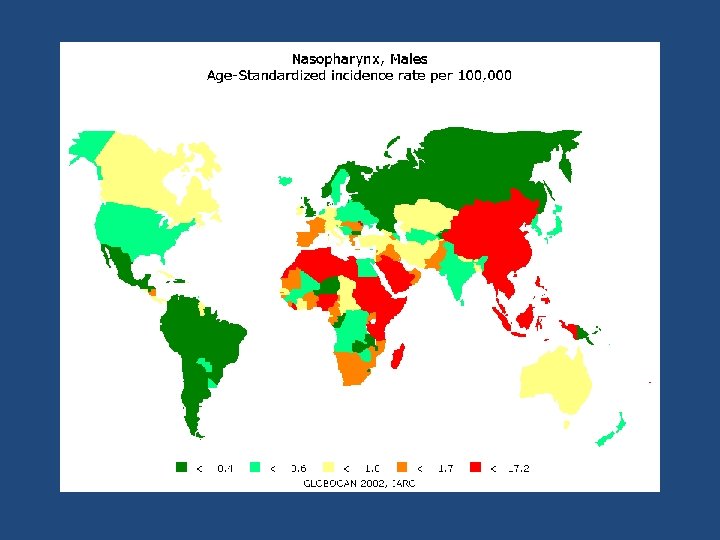
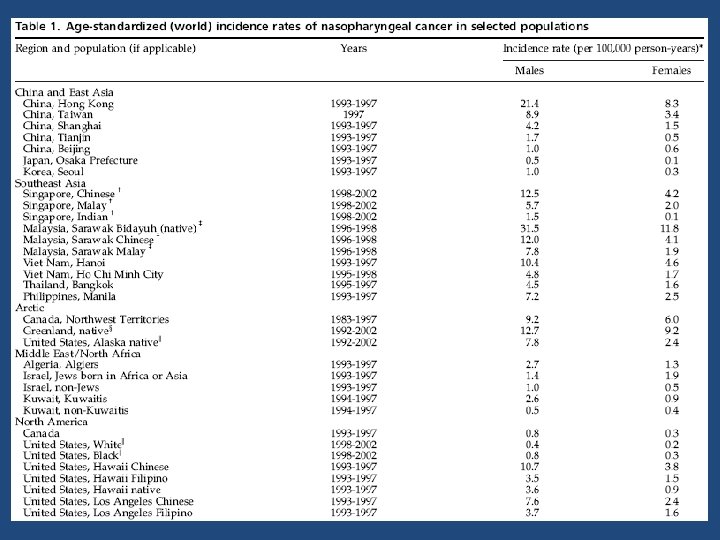
Incidence & Mortality • 80, 000 cases with 50, 000 deaths annually – < 1 per 100, 000/year incidence – 23 rd most common cancer in the world • 2 -3 fold higher risk for males: females • Broad racial/ethnic and geographic variation – 4 th most common cancer in Hong Kong • Highest incidence in Asian, N African/Mid east, and Arctic populations
Migrant Studies • After migration, risk remains high – Chinese in US have 10 -20 fold increased risk compared to US Whites and Blacks – However, Chinese immigrants have ½ the risk of their counterparts in China – Conversely, Whites born in China or Philippines have an increased risk for NPC compared with US • Suggests both environmental and genetic components
NPC Incidence and Age US incidence by age • Monotonic increase with age • Secondary peak from 55 -59 yo Hong Kong incidence by age • Peak age at 50 -59 yo Source: Chang et al. Cancer Epidemiol Biomarkers Prev. 2008; 15(10): 1765 -77
NPC Prognosis • Overall 5 -year survival of 65% (US) – Local: 80 -90% – Regional: 50 -70% – Advanced: poor • Varies by type: – Undifferentiated (type III) has best prognosis due to high radiosensitivity – Keratinizing (type I) have worst prognosis • more radioresistant
Epstein-Barr Virus (EBV) & NPC • Member of the herpesvirus family • Transmitted chiefly via saliva • Primarily targets B lymphocytes but also infects oropharyngeal tissue • EBV DNA detected in ~100% of type II and III NPC – Type I is not as consistent – Also detected in NP dysplasia
EBV Prevalence • > 90% of the world population is EBV seropositive (mostly latent infection) • Geographic variability in when infection occurs – Hong Kong: • 80% of kids infected by age 6 • ~100% by age 10 – US: • 50% of kids infected by age 5 • 95% of adults infected by age 40 • Tends to occur earlier in developing countries – Likely due to crowding and less hygienic conditions • 30 -50% adults develop mononucleosis after primary infection – Usually latent in children
EBV & NPC • Early-life EBV infection increases risk • EBV appears to be a necessary but insufficient cause of cancer – Most people are infected; only a small minority get the disease • EBV most likely interacts with genetic and environmental risk factors in NP carcinogenesis Environment EBV Genetics NPC
Salt-Preserved Fish & Meat • Strongest non-viral risk factor (especially fish) • Associated with type II & III – Weekly consumption: 1. 4 -3. 2 fold increased risk – Daily consumption: 1. 8 -7. 5 fold increased risk • Childhood exposure increases risk > adult – Traditional weaning food in China • Salt is an ineffective preservative – Partial putrification – Contains: • • Nitrosamines (also found in tobacco) Bacterial mutagens Genotoxins EBV reactivating compounds
Smoking • 2 -6 fold increased risk of NPC – Particularly true for Type I – 2/3 of Type I attributable to smoking • IARC classifies smoking as a Group I carcinogen – Sufficient causal evidence for NPC
Occupational Exposures • Nasal cavity is the primary initial site of fume exposure • Difficult to study due to (relatively) rare exposures • Occupational exposures associated with NPC: – Formalin • 2 -4 fold increase in risk • Although not consistent across all studies • Supported by evidence from animal studies – Heat/combustion exposures – Wood dust – Chlorophenols
Other Risk Factors • Fruit & vegetable consumption (protective) • Prior hx of chronic ENT or respiratory infection – 2 -fold increase in risk • Family hx of NPC – 4 -10 fold increased risk for 1 st degree relative hx • Some HLA and xenobiotic metabolism alleles have been associated with NPC
Salivary Gland Cancers
Salivary Gland Cancers • 1 -3% of head and neck cancers • Incidence: 2 per 100, 000 people/yr – Incidence is rising in US • Mean age is 64 yo – 2/3 occur in people > 55, although occur at all ages • Heterogeneous group of malignancies – WHO lists 18 histologies
Site of Origin • Major salivary glands: 95% of cancers – 80% occur in the parotid • 20% of parotid tumors are malignant – 10% occur in the submandibular gland • > 50% are of submandibular tumors are malignant – 5% occur in the sublingual glands • > 50% of sublingual tumors are malignant • Minor salivary glands – Cancers mostly occur in the oral cavity, nasopharynx or nasal cavity
Clinical Presentation & Treatment • Present as fixed, painless lumps or swelling, with trismus, or facial nerve weakness – May present with or without lymphadenopathy • Surgery is the primary treatment modality – May be combined with radiation • Stage and grade correlate well with prognosis • After primary treatment, 50% experience local, regional, or distant mets
5 -year Survival by Stage at Diagnosis 100% 96% 90% 77% 80% 73% 70% 60% 50% 37% 40% 30% 20% 10% 0% I II IV
Salivary Gland Cancers • Major risk factors: – Radiation – Mixed results for occupational exposures • Because it is relatively rare, there are few epidemiologic studies available with adequate statistical power to identify associations
Mucoepidermoid Carcinoma (MEC) • • Most common: 30 -35% of salivary tumors Usually involves major salivary glands 3: 2 female: male ratio Mean age of diagnosis is in 5 th decade – Occurs at all ages – Most common salivary malignancy in children
MEC Prognosis • 30 -70% present with nodal involvement • 10 -20% present with distant mets • Grade correlates well with prognosis – High grade: < 50% 5 -year survival – Low grade: 95% 5 -year survival • Recurrences are mostly locoregional but can metastasize (lung, bone)
Adenoid Cystic Carcinoma (ACC) • 2 nd most common salivary cancer • Occurs in both major and minor glands – Most common minor salivary malignancy • 3: 2 female: male ratio • 4 th – 6 th decade is the peak occurance – But occurs at all ages
ACC Prognosis • Patients initially do well but do poorly long term – 5 -year survival = 89% – 15 year survival = 40% • Local control w/ surgery & radiation = 85% • Tends to recur up to several years later as systemic mets – 30 -50% experience distant mets – Rarely mets to regional lymph nodes • Often associated with perineural invasion
Adenocarcinomas • Acinic cell carcinoma – Most occur in the parotid – Generally slow growing – Usually low grade but depth of invasion into adjacent tissue is a better predictor of prognosis • Polymorphous low-grade adenocarcinoma – Occurs in minor glands; good prognosis • Adenocarcinoma, NOS – Poor 5 -year survival (< 50%)
Rare Adenocarcinomas • Typically low grade (good prognosis): – Basal cell adenocarcinoma – Clear cell adenocarcinoma – Cystadenocarcinoma – Sebaceous adenocarcinoma – Mucinous adenocarcinoma • Typically high grade (poor prognosis) – Oncocytic adenocarcinoma – Salivary duct carcinoma
Malignant Mixed Tumors • Tend to occur in the major glands • Prognosis depends upon grade 1. Carcinoma ex pleomorphic adenoma – Account for the majority of MMTs 2. Carcinosarcomas 3. Metastasizing mixed tumor very, very rare
Other Salivary Malignancies • Squamous cell carcinoma • Epithelial-myoepithelial carcinoma • Anaplastic small cell – Minor glands; quick growing • Undifferentiated carcinoma (poor outcome) – Large cell undifferentiated – Lymphoepithelial carcinoma • Higher incidence in Inuits
Questions