Thyroid Cancer A CaseBased Approach Lab Evaluations T

Thyroid Cancer A Case-Based Approach


Lab Evaluations § T 3 : 0. 7 nmol/L Normal : 0. 8 – 1. 9 § T 4 : 7. 7 nmol/L Normal : 4 – 13 § TSH : 0. 65 μIU/ml Normal : 0. 25 – 5. 3 7. 7. 1394

THYROID SCAN Fining of upper lobe may be due to previous surgical resection or a cold nodule of the left upper lobe 7. 7. 1394

NECK MRA Lt lobe of thyroid is enlarged and heterogenous with multiple nodule , multiple large LAPs are seen in the Lt anterior cervical chain. 5. 7. 1394

NECK MRA Multiple large LAPs are seen in the Lt anterior cervical chain. 5. 7. 1394

NECK CT SCAN 12. 1. 1395

Pathologic Report Left thyroid lobe Specimen size : 6 x 3 x 2 cm , 5 x 3 x 2 cm , weight : 35 gr Tumor focality : Multifocal Dominant tumor : Tumor size : 5 x 3 x 2 cm Histologic type : PTC Histologic grade : G 1 , well differentiated Tumor capsule : Partially encapsulated Tumor capsular invasion : Tumor touches thyroid capsule , but not passing through that. Lymph – vascular invasion : not identified Perineural invasion : not identified Exterathyroidal extension : not identified

Pathologic Report Left thyroid lobe Dominant tumor : Tumor size : 2. 5 x 2 x 1. 5 cm Histologic type : PTC Histologic grade : G 1 , well differentiated Tumor capsular invasion : Tumor touches thyroid capsule , but not passing through that. Lymph – vascular invasion : not identified Perineural invasion : not identified Exterathyroidal extension : not identified Parathyroid tissue also included

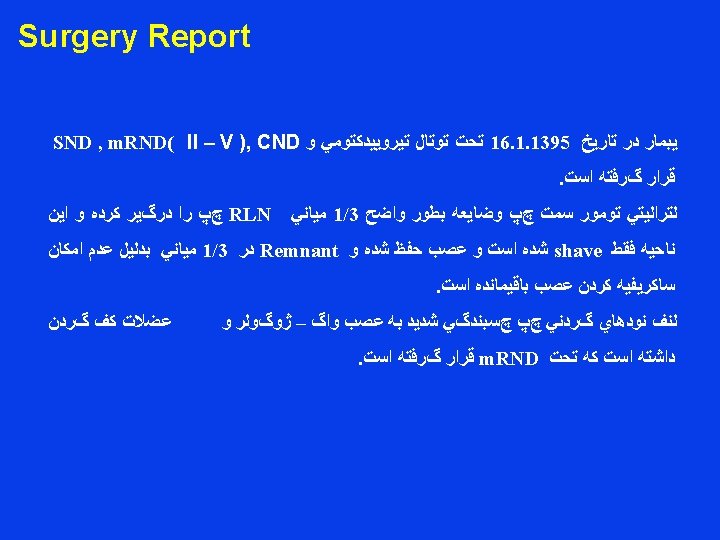
Pathologic Report Left thyroid lobe adhesion site : Involvement by papillary carcinoma Left cervical lymph nodes : Eight out of 44 dissected lymph nodes are involved by tumor , three with extranodal extension.
 involved by tumor Right cervical")
Pathologic Report Right thyroid lobe Thyroid tissue focally (isthmus) involved by tumor Right cervical lymph nodes( level II – IV ) Three out of 15 dissected lymph nodes are involved by tumor Right paratracheal lymph node : One lymph node involved by tumor

Lab Evaluations § T 3 : 0. 6 nmol/L Normal : 0. 53 – 1. 85 § T 4 : 44. 8 nmol/L Normal : 60 – 120 § TSH : 18. 2 μIU/ml Normal : 0. 3 – 6 § Ca : 9. 4 mg/dl Normal : 8. 6 – 11 § P : 4. 6 mg/dl Normal : 0. 3 – 6 23. 1. 1395
 After")
A Case of Locally Invasive PTC with Residual Disease (p. T 4) After Surgery

Epidemiology Thyroid cancer is a rare malignancy but it is the most common endocrine malignancy 2 to 4 times more frequent in females than in males PTC is most common DTC– 50 -90% Incidence increased from 20, 000 to 62, 800 1992 5/100, 000 2014 15/100, 000 Almost all of increase is papillary thyroid cancer Most likely Increasing use of imaging technologies (Overdiagnosis ) Deaths n=1850 , Not changed

Overdiagnosis of thyroid cancer At one center : PTC <1 cm: 14% to 56% in 10 years

Possible Causes of Increasing Incidence Radiation Exposure Iodine intake Obesity/Diabetes Autoimmune Disease Estrogen/Progesterone Reduced smoking But most likely Increasing use of imaging technologies – Overdiagnosis

Epithelial Thyroid Tumors THYROID CANCER FREQUENCY MORTALITY Papillary 85% 1 -2% at 20 years Follicular 11% 10 -20% at 10 years Medullary 3% 25 -50% at 10 years Anaplastic 1% 90% at 5 years 1 patient in 100 with PTC will die due thyroid cancer at 20 years Surveillance Epidemiology and End Results. http: //seer. cancer. gov/statfacts/html/thyro. htm

Presenting Features PTC is frequently multifocal when it occurs in a single lobe PTC is bilateral in 20% to 80% of cases Extrathyroidal invasion : 15% of patients at primary surgery Clinically evident lymphadenopathy at presentation : one third of PTC Histologic evidence of lymphadenopathy : between 35% and 50% PTC patients have distant metastases at diagnosis : 1% to 7% PTC patients present with Stage I (60%) Stage II (22%) Stage III fewer than 20% Stage IV (1% to 7%)

Factors Associated with Adverse Prognosis Older age Distant metastases Less well-differentiated histologic variant , widely invasive, tall cells, columnar cells, oxyphilic cells, insular. . . Large tumor size Extrathyroidal invasion Multicentricity Lymph node metastases High tumor grade and DNA aploidy Male gender BRAF(V 600 E) mutation

Locally Invasion DTC

DTC accounts for 54– 94% of all locally advanced thyroid cancers. Invasive DTC has been reported to occur in 10 -15% of patients at the time of diagnosis. Although, in general, DTC is more common in women, locally advanced DTC is more common in men. The presence of extrathyroidal invasion is one of the main risk factors for developing DTC recurrence , distant metastasis and mortality from DTC. Locally advanced DTC may involve the central neck, lateral neck and/or mediastinum by direct tumor invasion or by lymphatic invasion. E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99

The most commonly involved structures in the central neck are the recurrent laryngeal nerve, laryngotracheal tree, esophagus and strap muscles. In the lateral neck compartment, locally advanced DTC either by direct tumor extension from a primary thyroid tumor or extracapsular invasion from lymph node metastasis invade the carotid artery, internal jugular vein, nerves(e. g. vagus, spinal accessory and phrenic) and sternocleidomastoid muscle. E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99

Clinical features Clinical evidence of a palpable neck mass in the central or lateral neck compartments. Neck pain and/or stiffness but rarely otodynia. Voice fatigue or hoarseness this usually indicates involvement of the recurrent laryngeal nerve(s). Dysphagia, cough, hemoptysis, and a recent episode of pneumonia or even frank stridor, this usually indicates laryngotracheal involvement. The presence of dysphagia may be due to esophageal invasion or extrinsic compression. Superior vena cava syndrome should be suspected in patients with advanced DTC when a positive Pemberton’s sign. Some patients with locally advanced DTC may have no local symptoms. E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99

preoperative evaluation
 Preoperative neck US for cervical (central and especially lateral neck")
RECOMMENDATION 32 A) Preoperative neck US for cervical (central and especially lateral neck compartments) lymph nodes is recommended for all patients undergoing thyroidectomy for malignant or suspicious for malignancy cytologic or molecular findings. (Strong recommendation, Moderate-quality evidence) B) US-guided FNA of sonographically suspicious lymph nodes > 8 -10 mm in the smallest diameter should be performed to confirm malignancy if this would change management. (Strong recommendation, Moderate-quality evidence) C) The addition of FNA-Tg washout in the evaluation of suspicious cervical lymph nodes is appropriate in select patients, but interpretation may be difficult in patients with an intact thyroid gland. (Weak recommendation, Low-quality evidence) 2015 American Thyroid Association

Neck and chest imaging with a CT scan or an MRI should be obtained preoperatively in all patients with locally advanced DTC. These imaging studies are useful for defining the extent of disease in the neck and mediastinum and identifying involved surrounding structures. E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99
 Preoperative use of cross-sectional imaging studies (CT, MRI) with intravenous")
RECOMMENDATION 33 A) Preoperative use of cross-sectional imaging studies (CT, MRI) with intravenous contrast is recommended as an adjunct to ultrasound for patients with clinical suspicion for advanced disease including invasive primary tumor, or clinically apparent multiple or bulky lymph node involvement. (Strong recommendation, low-quality evidence) B) Routine preoperative 18 FDG-PET scanning is not recommended. (Strong recommendation, low-quality evidence) 2015 American Thyroid Association

RECOMMENDATION 34 Routine preoperative measurement of serum Tg or Tg antibodies is not recommended. (Weak recommendation, Low-quality evidence) 2015 American Thyroid Association

Patients with locally advanced DTC or any change in their voice should have direct laryngoscopy to evaluate their vocal cord function. We recommend preoperative direct laryngoscopy in all patients undergoing cervical or mediastinal reoperation for recurrent DTC regardless of the presence or absence of local symptoms. E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99
 Preoperative")
RECOMMENDATION 41 Preoperative laryngeal exam should be performed in all patients with: A) Preoperative voice abnormalities (Strong recommendation, Moderate-quality evidence) B) History of cervical or upper chest surgery, which places the RLN or vagus nerve at risk (Strong recommendation, Moderate-quality evidence) C) Known thyroid cancer with posterior extrathyroidal extension or extensive central nodal metastases. (Strong recommendation, Low-quality evidence) 2015 American Thyroid Association

The risk of distant DTC metastasis is higher in patients with locally invasive DTC. These patients should have a work up for metastatic disease before considering surgical resection. The most common sites of DTC metastases are to the lung and bone and less frequently to the liver and brain. When the tumor traps radioiodine, whole body radioiodine scanning with 131 I is best for detecting possible sites of tumor metastases. In patients who have positive serum thyroglobulin levels but negative radioiodine scans, PET scanning may be useful for identifying metastatic disease instead of obtaining multiple imaging studies (CT and MRI scanning of the chest and abdomen and bone scan). E. Kebebew, O. H. Clark / Surgical Oncology 12 (2003) 91– 99

Operative approach
 For patients with thyroid cancer >4 cm, or with gross")
RECOMMENDATION 35 A) For patients with thyroid cancer >4 cm, or with gross extrathyroidal extension (clinical T 4), or clinically apparent metastatic disease to nodes (clinical N 1) or distant sites (clinical M 1), the initial surgical procedure should include a near-total or total thyroidectomy and gross removal of all primary tumor unless there are contraindications to this procedure. (Strong Recommendation, Moderate-quality evidence) 2015 American Thyroid Association

Lymph node dissection
 Therapeutic central-compartment (level VI) neck dissection for patients with clinically")
RECOMMENDATION 36 A) Therapeutic central-compartment (level VI) neck dissection for patients with clinically involved central nodes should accompany total thyroidectomy to provide clearance of disease from the central neck. (Strong Recommendation, Moderate-quality evidence) B) Prophylactic central-compartment neck dissection (ipsilateral or bilateral) should be considered in patients with papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes (c. N 0) who have advanced primary tumors (T 3 or T 4), clinically involved lateral neck nodes (c. N 1 b), or if the information will be used to plan further steps in therapy. (Weak Recommendation, Low-quality evidence) 2015 American Thyroid Association
 Thyroidectomy without prophylactic central neck dissection may be is appropriate for small (T")
C) Thyroidectomy without prophylactic central neck dissection may be is appropriate for small (T 1 or T 2), noninvasive, clinically node-negative PTC (c. N 0) and for most follicular cancers. (Strong Recommendation, Moderate-quality evidence) 2015 American Thyroid Association

RECOMMENDATION 37 Therapeutic lateral neck compartmental lymph node dissection should be performed for patients with biopsy-proven metastatic lateral cervical lymphadenopathy. (Strong Recommendation, Moderate-quality evidence) 2015 American Thyroid Association

post-operative staging systems and risk stratification in the management of DTC?

RECOMMENDATION 47 AJCC/UICC staging is recommended for all patients with DTC, based on its utility in predicting disease mortality, and its requirement for cancer registries. (Strong recommendation, Moderate-quality evidence) 2015 American Thyroid Association

AJCC 7 th edition/TNM Classification System for Differentiated Thyroid Carcinoma

AJCC 7 th edition/TNM Classification System for Differentiated Thyroid Carcinoma

T 4 a. N 1 b Mx Stage. II
 The 2009 ATA Initial Risk Stratification System is recommended for DTC")
RECOMMENDATION 48 A) The 2009 ATA Initial Risk Stratification System is recommended for DTC patients treated with thyroidectomy, based on its utility in predicting risk of disease recurrence and/or persistence. (Strong recommendation, Moderate-quality evidence) B) Additional prognostic variables (such as the extent of lymph node involvement, mutational status, and/or the degree of vascular invasion in follicular thyroid cancer), not included in the 2009 ATA Initial Risk Stratification system, may be used to further refine risk stratification for DTC as described below (and in Fig 4) in the Modified Initial Risk Stratification system. However, the incremental benefit of adding these specific prognostic variables to the 2009 Initial Risk Stratification system has not been established. (Weak recommendation, Low-quality evidence) 2015 American Thyroid Association
 While not routinely recommended for initial post-operative risk stratification in DTC, the mutational")
C) While not routinely recommended for initial post-operative risk stratification in DTC, the mutational status of BRAF, and potentially other mutations such as TERT, have the potential to refine risk estimates when interpreted in the context of other clinico-pathologic risk factors. (Weak recommendation, Moderate-quality evidence) 2015 American Thyroid Association

ATA 2009 Risk Stratification System with Proposed Modifications

ATA HIGH RISK

THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 NOVEMBER 1995

The 30 -year overall survival, disease-specific survival, an disease-free survival for all 1, 012 patients were 66%, 81%, an 63%, respectively. Patients with ETE had significantly poor survival. Thirty-year disease-specific survival was reduce from 87% to 29% (P <0. 0001), and disease-free survival w as reduced from 66% to 23% (P <0. 0001) among patients with ETE versus without ETE. Actuarial disease-specific survival for all patients and for patients without and with extrathyroidal extension (ETE) of thyroid carcinoma

The local, regional, and distant failure rates for all 1, 012 patients were 11%, 17%, and 12%, respectively, at 30 years. The patients with ETE had markedly poorer disease control after 30 years compared with patients without ETE. The local failure rate increased from 9% to 48% (P <0. 0001), whereas the regional failure rate increased from 15% to 41% (P <0. 0001). The rate of distant metastasis increased from 11% to 37% (P <0. 0001). The 30 -year actuarial treatment failure rates for lo- cal, regional, and distant metastases stratified for extrathyroidal extension (ETE) of thyroid carcinoma.

Univariate Analysis of Factors Affecting Survival Among 79 Patients With Extrathyroidal Extension The Effect of Complete Excision, Distant Metastasis, Nonpapillary Histology, and Tumor Size on Survival Compared By Age Range A

Multivariate analysis showed that age greater than 45 years, nonpapillary histology, distant metastasis at presentation and tumor size greater than 4 cm had an adverse impact on survival. Gender was not found to have an impact on survival. On multivariate analysis, incomplete tumor excision did not adversely affect survival among patients older than 45 years. Incomplete excision was found to be an adverse prognostic factor for patients 45 years old or younge.
")
radioactive iodine (RAI)
")
radioactive iodine (RAI)
 Post-operative disease status (i. e. the presence or absence of")
RECOMMENDATION 50 A) Post-operative disease status (i. e. the presence or absence of persistent disease) should be considered in deciding whether additional treatment (e. g. radioactive iodine, surgery, or other treatment) may be needed. (Strong recommendation, Low-quality evidence) B) Post-operative serum thyroglobulin (on thyroid hormone therapy or after TSH stimulation) can help in assessing the persistence of disease or thyroid remnant and predicting potential future disease recurrence. The Tg should reach its nadir by 3 -4 weeks post-operatively in most patients. (Strong recommendation, Moderate-quality evidence) C) The optimal cut-off value for post-operative serum thyroglobulin or state in which it is measured (on thyroid hormone therapy or after TSH stimulation) to guide decision-making regarding RAI administration is not known (No Recommendation, Insufficient evidence) 2015 American Thyroid Association
 Post-operative diagnostic radioiodine whole-body scans may be useful when the extent of the")
D) Post-operative diagnostic radioiodine whole-body scans may be useful when the extent of the thyroid remnant or residual disease cannot be accurately ascertained from the surgical report or neck ultrasonography, and when the results may alter the decision to treat, or the activity of RAI that is to be administered. Identification and localization of uptake foci may be enhanced by concomitant SPECT/CT. When performed, pretherapy diagnostic scans should utilize 123 I (1. 5– 3 m. Ci) or a low activity of 131 I (1– 3 m. Ci), with therapeutic activity optimally administered within 72 hours of the diagnostic activity. (Weak recommendation, Low-quality evidence) 2015 American Thyroid Association
 in our patient RAI therapy (intended to improve")
goal of post-operative administration of (RAI) in our patient RAI therapy (intended to improve disease-specific and disease free survival by treating persistent disease in higher risk patients) 100 – 200 mci 2015 American Thyroid Association

appropriate degree of initial TSH suppression
 For high-risk thyroid cancer patients, initial TSH suppression to below 0.")
RECOMMENDATION 59 A) For high-risk thyroid cancer patients, initial TSH suppression to below 0. 1 m. U/L is recommended. (Strong recommendation, Moderate-quality evidence) B) For intermediate-risk thyroid cancer patients, initial TSH suppression to 0. 1 - 0. 5 m. U/L is recommended. (Weak recommendation, Low-quality evidence) C) For low risk patients who have undergone remnant ablation and have undetectable serum Tg levels, TSH may be maintained at the lower end of the reference range (0. 5– 2 m. U/L) while continuing surveillance for recurrence. Similar recommendations hold for low-risk patients who have not undergone remnant ablation and have undetectable serum Tg levels. (Weak recommendation, Low-quality evidence) 2015 American Thyroid Association

External beam irradiation
 remains controversial. A number of retrospective")
The role of external beam radiotherapy (EBRT) remains controversial. A number of retrospective studies have demonstrated that EBRT potentially improves locoregional control in patients with nonanaplastic thyroid cancer who have high risk features for locoregional recurrence, such as p. T 4, lymph node involvement, micro-/macroscopic positive surgical margins, extensive extrathyroidal or extranodal extension at recurrence, or RAI-resistant recurrent disease. Kim et al. Radiation Oncology 2010 The British Thyroid Association recommends XRT in patients over 60 years of age with extensive extranodal spread after optimal surgery, even in the absence of evident residual disease Journal of Thyroid Research. Volume 2010. Young patients with gross residual or microscopic disease who are capable of concentrating tumoricidal doses of RAI are less likely to benefit from postoperative EBRT. Int. J. Radiation Oncology Biol. Phys. , Vol. 73, No. 3, pp. 795– 801, 2009

Int. J. Radiation Oncology Biol. Phys. , Vol. 73, No. 3, pp. 795– 801, 2009

Journal of Thyroid Research. Volume 2010

RECOMMENDATION 60 There is no role for routine adjuvant external beam radiation therapy to the neck in patients with DTC after initial complete surgical removal of the tumor (Strong recommendation, Low-quality evidence). 2015 American Thyroid Association

The use of chemotherapy concurrent with EBRT in patients with DTC is another area of controversy. In a report from Memorial Sloan Kettering Cancer Center , there was no major difference in acute or late toxicity between the two, but there was a nonstatistically different improvement in local progression-free survival (90. 0 % with chemoradiation and 73. 0 % with radiation alone). Despite local control in the neck, there was a high distant relapse rate of 47 %. Springer International Publishing Switzerland 2016

Thank you
- Slides: 70