Alterations and Management of Renal and Urinary Tract




 – Maintain acid urine (ph")



,")











































 – A nephrostomy tube may be")















































- Slides: 103
Alterations and Management of Renal and Urinary Tract Function Reviewed 2015
Cystitis / Urinary Tract Infections • Inflammation of the bladder from infection or obstruction of the urethra • Most common causative agents – – Eschericha coli Enterobacter Pseudomonas Serratia • More common in women – Shorter urethra – Location, location • Sexually active or pregnant women most vulnerable • Your patient who has had a foley catheter in place
Cystitis / Urinary Tract Infections • Assessment – – – Frequency and burning Burning on urination Voiding in small amounts Inability to void Incomplete emptying of the bladder Lower abdominal discomfort or back discomfort Cloudy, dark, foul-smelling urine Hematuria Bladder spasms Malaise, chills, fever Nausea and vomiting
Cystitis / Urinary Tract Infections • Nursing Implementation – Obtain a urine specimen for C&S, if prescribed, to identify bacterial growth prior to prescribing antibiotics – Instruct to force fluids (up to 3, 000 mls/day) especially if taking sulfonamide (can cause crystals in concentrated urine) – Administer meds as prescribed • • Antibiotics Analgesics Antispasmodics Antimicrobials
Cystitis / Urinary Tract Infections • Nursing Implementation (continued) – Maintain acid urine (ph 5. 5) by an acid-ash diet – Note that if on aminoglycoside, sulfonamide, or nitrofurantoin, the actions of these meds are diminished by acidic urine – Use strict aseptic technique when inserting and maintaining indwelling foley catheter (and intermittent catheterizations). – Discourage caffeine products – Avoid alcohol – Provide heat to abdomen or sitz bath for C/O discomfort – Instruct to take meds JUST as prescribed including schedule and take ENTIRE course – Instruct importance of follow-up culture following treatment
Cystitis / Urinary Tract Infections • Preventive Measures – – – – Good perineal care Avoid bubble baths; vaginal sprays/ deodorants Void frequently 2 -3 hours Hydration! Cotton panties Partners hands clean Menopausal women-estrogen vaginal creams to restore p. H
Urosepsis • A gram-negative bacteremia originating in the urinary tract • Mostly caused by E. coli • Most common cause is the presence of an indwelling catheter or untreated UTI who is medically compromised • Major problem is the ability of this bacterium to develop resistant strains • May lead to shock if not treated aggressively
Urosepsis • Assessment – Fever is the most common and earliest manifestation • Nursing Implementation – Obtain urine specimen for C&S – Administer IV antibiotics as prescribed, usually until patient has been Afebrile for 3 to 5 days – Administer oral antibiotics as prescribed after the 3 to 5 day afebrile period
Urethritis • An inflammation of the urethra commonly associated with sexually transmitted diseases (STD), and may be seen with cystitis • In men, it is most often caused by gonorrhea or chlamydial infection • In women, it is most often caused by feminine hygiene products or sanitary napkins, gels, sprays, spermicidal jellies or changes in vaginal mucosal lining
Urethritis • Females • Assessment – Males • Burning on urination frequency • Urgency • Nocturia • Difficulty voiding discharge from penis – – – Frequency Urgency Nocturia Painful urination Difficulty voiding Lower abdominal discomfort
Urethritis • Nursing Implementation Encourage fluids Prepare for testing to determine STD Administer antibiotics Administration of sitz baths If stricture occurs, prepare for dilation of urethra and instillation of antiseptic solution – Instruct to avoid intercourse until symptoms resolve – Instruct to avoid intercourse until STD resolved – Avoid perfumed TP or sanitary napkins and feminine hygiene sprays – – –
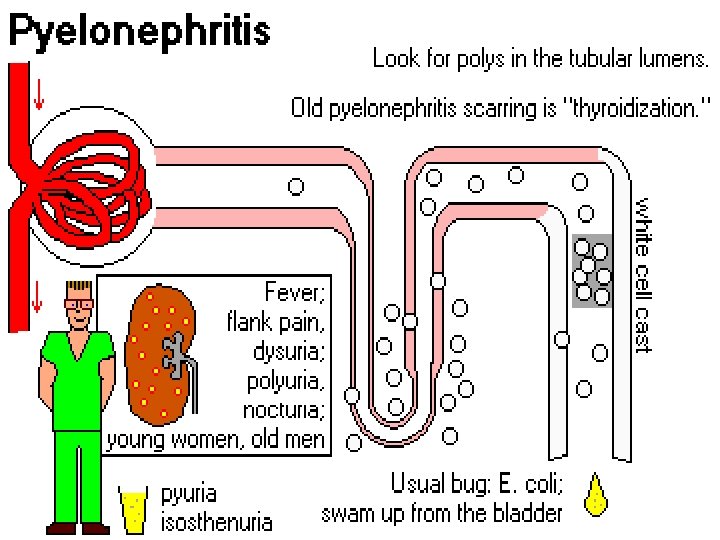
Ureteritis and Pyelonephritis • Ureteritis – Inflammation of the ureter, commonly associated with pyelonephritis – Chronic pyelonephritis causes the ureter to become fibrotic and narrowed by strictures • Pyelonephritis – Inflammation of the renal pelvis and the parenchyma, commonly by bacterial invasion – Often occurs after bacterial contamination of the urethra or following invasive procedure of the UT – Chronic pyelonephritis most commonly occurs following chronic obstruction with reflux or chronic disorders – E. coli is the most common bacterial causative organism
Acute Pyelonephritis • Usually a short course that recurs as a relapse of a previous infection or as a new infection • Can progress to bacteremia or chronic pyelonephritis
Acute Pyelonephritis • Assessment – – – – – Fever and chills Nausea Flank pain on affected side Costovertebral angle tenderness H/A Muscular pain Dysuria Frequency and urgency Cloudy, bloody, or foul-smelling urine Increased WBC in urine
Chronic Pyelonephritis • A slow, progressive disease that is usually associated with recurrent acute attacks • Causes contraction of the kidney and dysfunctioning of the nephrons, replaced with scar tissue • Can eventually lead to renal failure
Chronic Pyelonephritis • Assessment – Frequently diagnosed incidentally when client is evaluated for HTN – Poor urine-concentrating ability – Pyuria – Azotemia – Proteinuria – Anemia – Acidosis
Chronic Pyelonephritis • Nursing Implementation Monitor I and O Monitor vital signs Monitor weight Encourage fluids up to 3 liters/day Encourage adequate rest Instruct in a high-calorie, low-protein diet Provide warm moist compresses to flank area Encourage warm baths Administer analgesics, antipyretics, antibiotics, urinary antiseptics, and antiemetics as prescribed – Monitor for signs of renal failure – – – – –
Glomerulonephritis • A term that includes a variety of disorders, most of which are caused by an immunological reaction • Results in proliferative and inflammatory changes within the glomerular structure • Destruction, inflammation, and sclerosis of the glomeruli of both kidneys occur • The inflammation of the glomeruli results from an antigen-antibody reaction produced from infection elsewhere in the body • Loss of kidney function develops
Glomerulonephritis • Causes – Immunological or autoimmune diseases – Streptococcal infection, group A beta-hemolytic – History of pharyngitis or tonsillitis 2 to 3 weeks prior to symptoms • Types – Acute: occurs 2 to 3 weeks after Strep infection – Chronic: can occur after the acute phase or slowly over time
Glomerulonephritis • Complications – Heart failure – Hypertensive encephalopathy – Pulmonary edema – Renal failure
Glomerulonephritis • Assessment – Gross hematuria – Dark, smoky, cola-colored or red-brown urine – Proteinuria that produces a persistent and excessive foam in the urine – Urinary debris – Moderately elevated to high Sp Gr – Low urinary p. H – Oliguria or anuria – Headache, chills, fever – Fatigue, weakness
Glomerulonephritis • Assessment – Anorexia, nausea, vomiting – Pallor – Edema of the face, especially the periorbital area, feet, or generalized – SOB, ascites, pleural effusions and CHF – Abdominal or flank pain – Hypertension – Reduced visual acuity – Increased BUN; Creatinine – Increased antistreptolysin O titer (used to diagnose disorders caused by strep infections)
Glomerulonephritis • Nursing Implementation Monitor vital signs Monitor I and O and urine closely Monitor daily weights Monitor for edema Monitor fluid overload, ascities, pulmonary edema, and CHF – Restrict fluid intake as prescribed – Provide high-calorie, low-protein diet – Restrict sodium intake as prescribed if edema is present – – –
Glomerulonephritis • Nursing Implementation – Provide bed rest and limited activity – Instruct to obtain treatment for infections, specifically sore throats and URI – Administer diuretics, antihypertensives, and antibiotics as prescribed – Monitor for signs of renal failure, cardiac failure, hypertensive encephalopathy – Instruct to report signs of bloody urine, headache, or edema
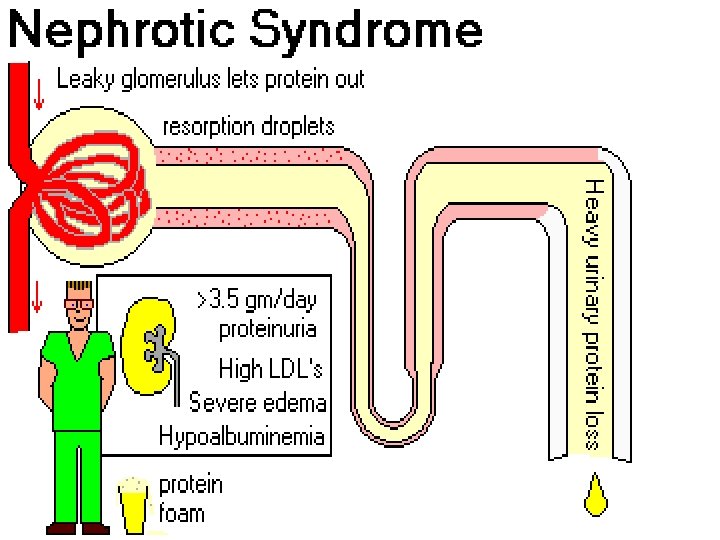
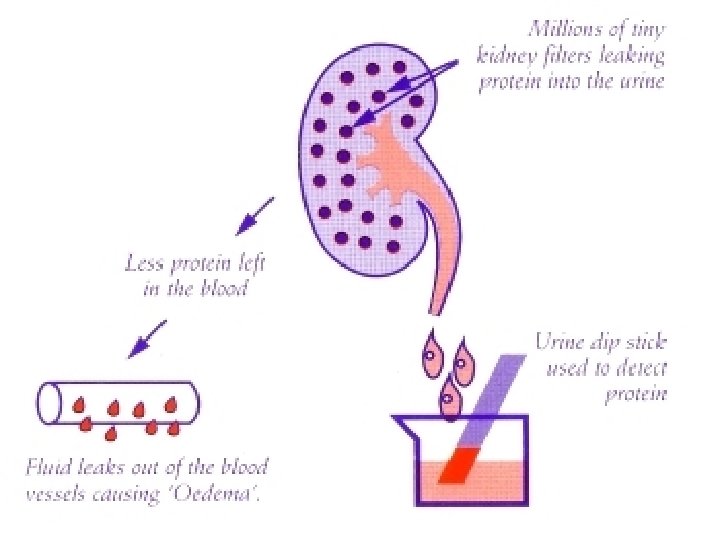
Nephrotic Syndrome • A set of clinical manifestations arising from protein wasting secondary to diffuse glomerular damage • Assessment – Proteinuria – Hypoalbuminemia – Edema – Hyperlipidemia – Waxy pallor to the skin – Anemia – Anorexia
Nephrotic Syndrome • Assessment – Malaise – Irritability – Amenorrhea or abnormal menses – Hematuria may be present – hypertension
Nephrotic Syndrome • Nursing Implementation Monitor I and O Monitor vital signs Bed rest if severe edema is present Normal to low-protein diet as prescribed with adequate carbohydrates and calorie intake – Monitor daily weights – Provide a mild sodium restriction as prescribed – –
Nephrotic Syndrome • Nursing Implementation – Monitor potassium level; potassium may be restricted from the diet if the potassium rises – Administer diuretics as prescribed – Administer corticosteroids and cytoxic medications as prescribed – Administer plasma volume expanders, such as albumin, plasma, and dextran, to raise the osmotic pressure – Administer anticoagulants as prescribed for those patients who develop renal vein thrombosis
Hydronephrosis • Distention of the renal pelvis and calices, caused by an obstruction of normal urine flow • The urine becomes trapped proximal to the obstruction • The causes include calculus, tumors, scar tissue, and kinks in the ureter
Hydronephrosis • Assessment – – Hypertension Headache Flank pain Electrolyte imbalances • Nursing Implementation – Monitor vital signs frequently – Monitor fluid and electrolyte imbalances, including dehydration after the obstruction is relieved – Monitor for diuresis, which can lead to fluid depletion – Monitor daily weights – Monitor urine for Sp. Gr, albumin, and glucose – Administer fluid replacement as prescribed
Polycystic Kidney Disease • A cystic formation and hypertrophy of the kidneys, leading to cystic rupture, infection, formation of scar tissue, damaged nephrons • There is no known way to arrest the process of the destructive cysts • The ultimate result of this disease is renal failure
Polycystic Kidney Disease • Types – Infantile polycystic disease: an inherited autosomal recessive trait that results in the death of the infant within a few months after birth – Adult polycystic disease: an autosomal dominant trait that results in end-stage renal disease
Polycystic Kidney Disease • Assessment – Flank, lumbar, or abdominal pain – Fever and chills – UTIs – Hematuria, proteinuria, pyuria – Calculi – Hypertension – Palpable abdominal masses and enlarged kidneys
Polycystic Kidney Disease • Nursing Implementation – Monitor for gross hematuria, indicating cystic rupture – Increase sodium and water intake because sodium loss rather than retention occurs – Provide bed rest if ruptured cysts and bleeding occur – Prepare patient for percutaneous cyst puncture for relief of obstruction, or for draining an abscess – Prepare the patient for dialysis or renal transplantation – Encourage patient to seek genetic counceling
Urolithiasis and Nephrolithiasis • Calculi or stones can form anywhere in the urinary tract; however, the most frequent site is the kidneys • The problems that can occur as a result – Pain – Obstruction – Tissue trauma – Hemorrhage – Infection
Urolithiasis and Nephrolithiasis • Determination – – – KUB IVP CT Renal ultrasound A stone analysis • Urolithiasis – Formation of urinary stones; urinary calculi formed in ureters • Nephrolithiasis – Formation of kidney stones – Formed in renal parenchyma
Urolithiasis and Nephrolithiasis • When a calculus occludes the ureter and blocks the flow of urine, ureter dilates, producing hydroureter • If obstruction is NOT removed, urinary stasis results • Infection ensues • Impairment of renal function on side of blockage • Resultant hydronephrosis • Irreversible kidney damage
Urolithiasis and Nephrolithiasis • Causes – Family history of stone formation – Diet high in calcium, vitamin D, milk, protein, oxalate, purines, or alkali – Diet high in urine-rich food – Obstruction and urinary stasis – Dehydration – Use of diuretics, causing volume depletion – UTIs and prolonged urinary catheterization – Immobilization – Hypercalcemia and hyperparathyroidism – Elevated uric acid, such as gout
Urolithiasis and Nephrolithiasis • Assessment – Renal colic originates in the lumbar region and radiates around the side and down toward the testicle in men, and to the bladder in the women – Ureteral colic radiates toward the genitalia and thigh – Sharp, severe pain of sudden onset – Dull, aching kidney – Nausea and vomiting, pallor, and diaphoresis during acute pain – Urinary frequency with alternating retention – Signs of a UTI – Low-grade fever – RBCs, WBCs, and bacteria in the urinalysis – hematuria
Urolithiasis and Nephrolithiasis • Nursing Implementation – Monitor vital signs – Monitor I and O – Assess for fever, chills, and infection – Monitor for nausea, vomiting, and diarrhea – Force fluids up to 3, 000 m. L/day unless contraindicated, to facilitate the passage of the stone and prevent infection – Strain all urine for the presence of stones
Urolithiasis and Nephrolithiasis • Nursing Implementation – Send stones to the laboratory for analysis – Provide warm baths and heat to the flank area – Administer analgesics at regularly scheduled intervals as prescribed to relieve pain and assess response – Administer IV fluids as prescribed to increase the flow of urine and facilitate the passage of the stone
Urolithiasis and Nephrolithiasis • Nursing Implementation – Assist in performing relaxation techniques to assist in relieving pain – Instruct in the diet specific to the stone composition – Maintain urinary p. H depending on the type of stone – Turn and reposition immobilized patients – Prepare the patient for surgical procedures if prescribed
Urolithiasis and Nephrolithiasis • Stone composition – Calcium phosphate stones • Caused by supersaturation of urine with calcium and phosphate • Diet includes acid ash foods because calcium stones have an alkaline chemistry • Dietary prescription may include to decrease intake of foods high in calcium and phosphate to reduce urinary calcium content, and to avoid excess vitamin D intake to prevent stones from forming
Urolithiasis and Nephrolithiasis • Stone composition – Calcium Oxalate stones • Caused by supersaturation of urine with calcium and oxalate • Diet includes acid ash foods because calcium stones have an alkaline chemistry • Dietary prescription may include decreasing intake of foods high in calcium • Dietary prescription may include avoiding oxalate food sources to reduce urinary oxalate content and the formation of stones • Oxalate-rich food sources include tea, almonds, cashews, chocolate, cocoa, beans, spinach, and rhubarb
Urolithiasis and Nephrolithiasis • Stone composition – Struvite stones • AKA triple phosphate stones and are composed of magnesium and ammonium phosphate • Caused by urea slitting by bacteria • Struvite stones tend to form in alkaline urine • Diet includes acid ash foods • Dietary prescription includes to limit high-phosphate foods such as dairy products, red and organ meats, and whole grains • Reduces urinary phosphate content
Urolithiasis and Nephrolithiasis • Stone composition – Uric acid stones • Caused by excess dietary purine or gout • Uric acid stones tend to form in acidic urine • Dietary prescription may include alkaline ash foods and decreased intake of purine sources, such as organ meats, gravies, red wines, and sardines • Reduces urinary purine content • Allopurinol (Zyloprim) may be prescribed to lower uric acid levels
Urolithiasis and Nephrolithiasis • Stone composition – Cystine stones Caused by cystine crystal formation Cystine stones tend to form in acidic urine Diet includes alkaline ash foods Dietary prescription may also include a low intake of methionine, an essential amino acid that forms cystine • Patient instructed to avoid meat, milk, cheese, and eggs • Dietary measures also focus on encouraging fluid intake up to 3 L/day unless contraindicated • Helps dilute urine and prevent crystals from forming • •
Mangement of Kidney Stones • Cystoscopy – May be done for stones located in the bladder or lower ureter – There is no incision – One or two urethral catheters are inserted past the stone – The stone may be manipulated and dislodged by the procedure
Mangement of Kidney Stones • Cystoscopy – The catheters may mechanically guide the stones downward as they are removed – Catheters are left in place for 24 hours to drain the urine trapped proximal to the stone and to dilate the ureter – A continuous chemical irrigation may be prescribed to dissolve the stone
Mangement of Kidney Stones • Extracorporeal shock wave lithotripsy – Noninvasive mechanical procedure for breaking up stones that are located in the kidney or upper ureter so that they can pass spontaneously or be removed by other methods – Flouroscopy is used to visualize the stone – There is no incision or drains – Ultrasonic waves are delivered through a bath of warm water to the areas of the stone to disintegrate it – Stones are passed in the urine within a few days
Mangement of Kidney Stones • Extracorporeal shock wave lithotripsy – Post-procedure Monitor vital signs Monitor I and O Monitor for bleeding Monitor for pain and signs of urinary obstruction • Instruct patient to increase fluid intake to wash out stone fragments • Inform patient that ambulation is important to facilitate process • •
Mangement of Kidney Stones • Percutaneous Lithotripsy – Performed for stones in the bladder, ureter, or kidney – An invasive procedure in which a guide is inserted under flouroscopy near the area of the stone – An ultrasonic wave is aimed at the stone to break into fragments – May be performed via cystoscopy or nephroscopy – No incision is required for cystoscopy; however a small flank incision is needed for nephroscopy – The patient may possibly have an indwelling catheter
Mangement of Kidney Stones • Percutaneous Lithotripsy (continued) – A nephrostomy tube may be placed to administer chemical irrigations to break up the stone; nephrostomy tube may remain in place for 1 to 5 days – Encourage patient to drink 3, 000 to 4, 000 m. L of fluid per day following procedure – Monitor for and instruct to monitor for complications of infection, hemorrhage, and extravasation of fluid into the retroperitoneal cavity
Ureterolithotomy • An open surgical procedure • Performed if lithotripsy not effective • Incision into ureter is made through lower abdominal or flank incision to remove stone • Patient will have Penrose drain, a urethral stent catheter, and an indwelling bladder catheter
Pyelolithotomy • A flank incision into the kidney is made to remove stones from the renal pelvis • A large flank incision is required • The patient will have a Penrose drain and an indwelling catheter
Nephrolithotomy • Incision into the kidney is made to remove the stone • A large flank incision is required • The patient may have a nephrostomy tube and an indwelling catheter
Partial or total Nephrectomy • Performed if there is extensive kidney damage, renal infection, or severe obstruction, and to prevent stone recurrence
Partial or total Nephrectomy • Postoperative Nursing Implementation – The plan of care will be focused based on incision location and type of drainage tubes present – Large amounts of urine will be draining – Place an ostomy pouch over the Penrose drain to protect skin if urinary drainage is excessive – Monitor nephrostomy tube, for free flow of urine – Do NOT irrigate urethral catheter!!
Partial or total Nephrectomy • Postoperative Nursing Implementation – Monitor indwelling Foley catheter for drainage – Encourage fluids to ensure urinary output (2500 to 3000 ml or more per day) – Monitor I and O closely – Determine composition of stone from Lab analysis – Instruct patient in dietary restrictions if required – Instruct patient about medications that may be needed for long term to reduce development of calculi
Partial or total Nephrectomy • Postoperative Nursing Implementation – Medications prescribed for calcium stones may include phosphates, thiazide diuretics, and allopurinol (Zyloprim) – Pyridoxine or magnesium oxide may be prescribed for patients with oxalate stones – Allopurinol (Zyloprim) may be prescribed for oxalate and uric acid stones – Long-term antibiotics may be prescribed for struvite or cystine stones
Kidney Tumors • May be benign or malignant, bilateral or unilateral • Common sites include bone, lungs, spleen or other kidney • The exact cause of renal carcinoma is unknown
Kidney Tumors • Assessment – Dull flank pain – Palpable renal mass – Painless gross hematuria
Kidney Tumors • Radial Nephrectomy – Removal of entire kidney, adjacent adrenal gland, and renal artery and vein – Radiation therapy and possibly chemotherapy may follow
Kidney Tumors • Post-operative Nursing Implementation Monitor vital signs Monitor I and O and daily weights Monitor abdomen for distention caused by bleeding Observe bed linens under patient for bleeding Monitor for hypotension, decrease in urinary output, and alterations in LOC, as signs of hemorrhage (hypovolemic shock) – Monitor for signs of adrenal insufficiency – – –
Kidney Tumors • Post-operative Nursing Implementation – In patient with adrenal insufficiency, a large urinary output followed by hypotension and subsequent Oliguria occurs – Administer IV fluids and PRBCs as prescribed – Monitor for urinary output of 30 to 50 mls an hour to ensure adequate renal function – Monitor urine for SPGr – Maintain Semi-Fowler’s position
Kidney Tumors • Post-operative Nursing Implementation – Monitor for signs of respiratory complications related to surgery – Encourage coughing and deep breathing exercises – Monitor bowel sounds for paralytic ileus – Apply antiembolism stockings as prescribed – Do not irrigate or manipulate nephrostomy tube if in place – Administer pain medications as prescribed
Bladder Trauma • Occurs following blunt or penetrating injury to lower abdomen • Penetrating wounds occur as a result of stabbing, gunshot wound, other missiles, or any objects piercing the abdominal wall • A fractured pelvis that causes bone fragments to puncture the bladder is the most common cause of bladder trauma • A blunt trauma causes compression of the abdominal wall and the bladder
Bladder Trauma • Assessment – Anuria – Hematuria – Pain over the Costovertebral area – Nausea and vomiting
Bladder Trauma • Nursing Implementation – Monitor vital signs – Monitor for hematuria, hemorrhage, and signs of shock – Promote bed rest – Monitor pain level – Prepare patient for insertion of a suprapubic catheter to aid in urinary drainage if prescribed – Prepare patient for surgical repair of the laceration
Kidney Transplant • Implantation of a human kidney from a compatible donor into a recipient • For irreversible kidney failure • Immunosuppressive drugs must be taken for the rest of the life
Kidney Transplant • Living related donors – Most desirable – Screened for ABO blood group, tissuespecific antigen, human leukocyte antigen (HLA) suitability, and mixed lymphocyte culture index (histocompatibility) – Donor must be in excellent health with 2 properly functioning kidneys – The emotional well-being of the donor is determined – Complete understanding of the donation process and outcome is necessary
Kidney Transplant • Cadaver donors Must meet criteria of brain death Must be under 60 years of age Must have normal renal function No malignant diseases outside the CNS No generalized infections No abdominal or renal trauma Must be hepatitis B negative (antigen) Must be HIV negative (antibody) Continuous ventilation and heartbeat maintain and Normal BP present until kidneys are “harvested” – Once potential donor has demonstrated cerebral death, it is crucial to restore IV volume, wean from vasopressors, and establish diuresis – – – – –
Kidney Transplant • Warm Ischemic Time – The time elapsed between the cessation of perfusion and cooling of the kidney, and the time required for anastomosis of the kidney – Max time is 30 to 60 minutes – Kidney is cooled, then max transplant time is 24 to 48 hours
Kidney Transplant • Preoperative Nursing Implementation – Verify histocompatability tests of identical twin or family member on chart – Administer immunosuppressive medications to recipient as prescribed, for 2 days before transplant – Maintain protective isolation – Verify hemodialysis of the recipient was completed 24 hours before transplant – Ensure patient is free of any infections – Assess renal function studies – Encourage discussion of feelings of both recipient and donor
Kidney Transplant • Postoperative Nursing Implementation – Kidney begins to function immediately (if its going to!) or be delayed a few days (not a great signs) – Hemodialysis is performed until adequate kidney function is established – Monitor vital signs – Monitor I and O – Monitor urine output every hour – Monitor daily lab studies • Urine for blood • Urine for Specific Gravity • BUN and creatinine
Kidney Transplant • Postoperative Nursing Implementation Daily weights, pulse Oximetry Maintain patient in semi-Fowler’s position Monitor for patency of the foley catheter Note that urine is pink and bloody initially but should gradually return to normal within several days to weeks – Monitor for gross hematuria and clots, which are not expected! And notify MD Immediately – –
Kidney Transplant • Postoperative Nursing Implementation – Monitor the three-way bladder irrigation if prescribed, to prevent blood clot formation – Note that the foley catheter should be removed as soon as possible to prevent infection – Maintain protective isolation precautions and monitor for infection – Monitor IV fluids closely and for fluid overload – Begin oral fluids as prescribed – Monitor for bowel sounds and initiate diet as prescribed when bowel sounds return
Kidney Transplant • Postoperative Nursing Implementation – Maintain good oral hygiene, monitoring for stomatitis and bacterial and fungal infections – Encourage coughing and deep breathing exercises – Maintain strict aseptic technique with wound care – Administer medications as prescribed, which may include antifungal medications, antibiotics, immunosuppressive agents and corticosteroids – Assess for organ rejection – Promote live donor and recipient relationship – Monitor patient and recipient for depression
Kidney Transplant • Graft Rejection: except for identical twin, this is major complication • Assessment – – – – Fever Malaise Elevated WBC count Graft tenderness Signs of deteriorating renal function Acute hypertension Anemia
Kidney Transplant • Hyperacute rejection – Occurs immediately after surgery to 48 hours postoperatively – Implementation: removal of rejected kidney • Acute rejection – Occurs within 6 weeks to 2 years – Potentially reversible with increased immunosuppression – Implementation: high doses of corticosteroids – If ineffective, monoclonal antibodies may be tried
Kidney Transplant • Chronic rejection – Occurs slowly over months to years after transplant – Can be irreversible – Mimics CHF • Nursing Implementation – Immunosuppressive medications
Patient discharge instructions following kidney transplant • • • Avoid prolonged periods of sitting Recognize S/S infection Recognize S/S of rejection Avoid contact sports Avoid exposure to people with infections Use medications as prescribed, and maintain immunosuppressive therapy for life
Urinary Diversions • A urinary diversion may mean a urostomy, which requires a pouch to be worn outside the body, or a continent diversion, which involves the creation of a pouch or bladder inside the body, usually using part of the digestive tract. The ileal conduit is made from a short segment of the small intestine. The ureters are attached to one end of the conduit. The other end is placed at the skin’s surface to create a stoma.
Urostomy • A surgeon creates a urostomy by redirecting urine to an opening created in the abdomen. • The opening is called a stoma. • Two main types of urostomy are available.
Ileal conduit • To create an ileal conduit, the surgeon takes a short segment of the small intestine and reconnects the remaining intestine so that it functions normally. • One end of the removed short segment of intestine is placed at the skin surface to create the stoma
Ileal conduit • The ureters, which normally carry urine from the kidneys to the bladder, are then attached to the other end of the segment of intestine. • The urine travels through the newly formed Ileal conduit and the stoma into an external collecting pouch. • The pouch has an outlet for releasing urine into a toilet without removing it from your stoma.
Ureterostomy • Very rarely, the surgeon connects the ureters directly to the abdominal wall to create a stoma. • Like the ileal conduit, a ureterostomy requires a collecting pouch placed over the stoma because there are no muscles around the stoma to control the flow of urine. In a ureterostomy, the ureters are connected directly to the abdominal wall to create two stomas.
Continent diversion • Another method of storing and eliminating urine • surgeon creates a pouch, or reservoir, inside the body from a section of the stomach or small or large intestine. • The ureters carry urine to the pouch, where it is stored. • Depending on the type of continent diversion, there may or may not have a stoma.
• Continent cutaneous This form of continent reservoir diversion does include a stoma. This method requires you to empty the reservoir, the internal pouch, regularly through the stoma using a catheter or thin plastic tube. If the urethra is preserved during the operation, may be able to have a urinary diversion that does not require a stoma or catheter. With a continent cutaneous reservoir, an internal pouch stores urine. The patient uses a catheter or plastic tube to empty urine through the stoma.
Bladder substitute • This method lets the patient urinate through his own urethra as he did with his original bladder, or may have to empty using a catheter through the urethra. • The surgeon creates an internal pouch that stores urine as the bladder did. • It is connected to the urethra so the patient may be able to empty the bladder in the normal way, although there will be a need to use different muscles to expel the urine. With a bladder substitute, the patient can urinate through the urethra
The Pouching System • The pouching system may consist of two pieces—a barrier that sticks to the skin and a pouch that attaches to the barrier. • In some systems, the barrier and pouch are a single unit. A two-piece pouch system. The square barrier sticks to the skin. The pouch attaches to the barrier.
Discharge Instructions • Using a Catheter – ‘If you have a continent reservoir, you will learn how to insert a catheter through the stoma or your urethra to drain your reservoir. ” – “You may do this either by standing in front of the toilet or by sitting on the toilet and then emptying the catheter between your legs. ” – “In the first few weeks, you will need to use the catheter every couple of hours. Soon, you will be able to go 4 to 6 hours between catheterizations. Wash your hands with soap and water each time you use a catheter. ”
Cleaning • ‘If you use a pouch, you can clean your skin with a wet towelette or washcloth as you change the pouch. ’ • ‘Let your skin dry completely before you apply the new pouch. ’ • ‘If your skin becomes irritated, you can use protective skin wipes or an ostomy powder designed to protect the skin around a stoma. ’ • ‘If you have a continent diversion, you will need to irrigate, or flush out, the reservoir using sterile water or normal saline and a syringe. ’ • ‘Since the reservoir may be made from a part of the intestine, it may produce mucus that normally lines the digestive tract. ” • “Irrigating or flushing the reservoir clears this mucus from the reservoir. ” • “Talk with your health care provider about how often you should irrigate the reservoir. ”
Recognizing Infection • Urostomies and continent urinary diversions can get infected. • Symptoms of infection include – dark urine or urine containing excess mucus – strong-smelling urine – pain in the back – poor appetite – nausea – vomiting • “Call your health care provider if you notice any of these warning signs. ” • Drinking eight full glasses of water every day can help prevent infection by flushing out bacteria.
Diet • “You probably will be able to eat your normal diet. ” • “You may find that some foods, such as asparagus and seafood, cause urine to have a stronger odor. ” • “Talk with your health care provider about your dietary needs. ”
Clothing • Wearing a urostomy pouch does not require special clothing. • Modern pouches are designed to lie flat against the body so they can’t be noticed. • “You may wear the pouch tucked inside your underwear or between your underwear and your outer clothing. ” • Women may wear a pouch under a girdle as long as it is made of stretchy material. • Men may wear the pouch inside an athletic supporter.
Activities • “You will need to restrict your activity during the first 2 to 3 weeks after surgery. ” • “Avoid driving and heavy lifting to help your stoma heal. ” • “Once healed, you should be able do most of the activities you enjoyed before your surgery. ” • “The only exceptions may be contact sports like football or karate. ” • “If your job includes hard physical labor, talk with your doctor and your employer about making adjustments to your job responsibilities. ”
Relationships • “You may worry that people will have negative reactions regarding your surgery. Most people will never know that you are wearing a pouch, unless you choose to tell them. Friends and relatives are likely to be aware of your health problems, but only a spouse, intimate partner, or primary care taker need know the details of your urinary diversion surgery. Still, many people find being open about their situation is easier than keeping it a secret. • You can choose how much you will share about your condition. ”
Relationships • “You can still maintain a satisfying sexual relationship with your partner. ” • “Your doctor or WOC nurse will tell you when you may safely resume sexual activity after your surgery. ” • “Talk with your health care provider about any concerns you have with maintaining intimate relations. “ • “Your nurse or doctor can give you information about ways to protect your stoma during sex. “ • “You may also want to ask about specially designed apparel to enhance intimacy for people with ostomies. ” • “Communicating with your partner is essential. ” • “Share your concerns and wishes, and listen carefully to your partner’s concerns. ”
Hope Through Research • The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) has many research programs aimed at finding and improving treatments for urinary disorders. • Researchers supported by the NIDDK are working to understand the growth of bladder tissue in order to find artificial methods of generating that kind of tissue. In an experimental setting, a patient whose bladder must be removed may be given a replacement bladder made from bioengineered tissues instead of from a segment of the patient’s bowel. • The bioengineered tissue would function much more like a natural bladder.