Physiology of CNS Somatic Motor System By Dr

Physiology of CNS Somatic Motor System By Dr. Abdel Aziz M. Hussein Assist Prof of Medical Physiology

Inverse Stretch Reflex
 of a ms")
Inverse Stretch Reflex • It is a reflex relaxation (or lengthening) of a ms in response to excessive stretch or contraction of that ms.

Inverse Stretch Reflex

Inverse Stretch Reflex

Inverse Stretch Reflex

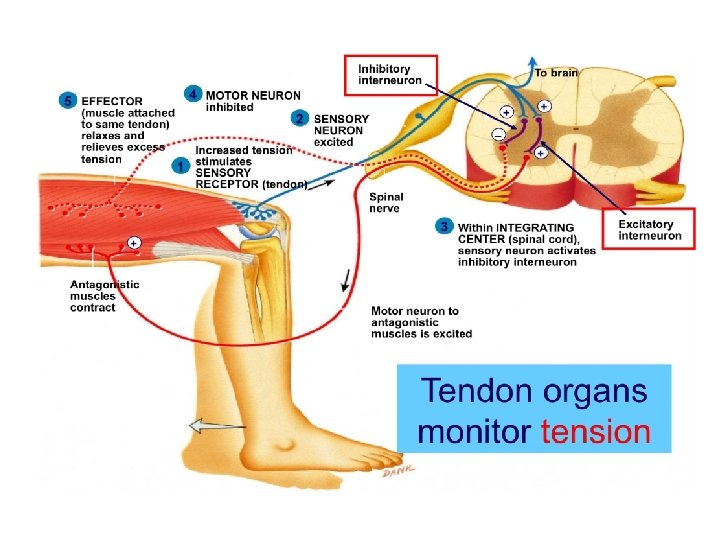
Inverse Stretch Reflex Neural pathway: • Stimulus: ↑ed ms tension by; 1. Overstretch or 2. Severe contraction • Receptors: Golgi tendon organs 1) Site: • tendons of skeletal ms in series with ms fibers 2) Structure: • Are encapsulated sensory receptor • 6 -20 elastic fibers 3) Innervations: • Type Ib or A alpha afferent fibres
 Receptors: GTOs • Stimulated by ↑ed ms tension caused by")
Golgi Tendon Organs (GTOs) Receptors: GTOs • Stimulated by ↑ed ms tension caused by passive overstretch or active contraction of the ms Afferents: • A alpha or Ib Center : a)inhibitory interneurons→ inhibit the α-MNs supplying the same ms b)excitatory interneurons→ excite the αMNs supplying the antagonistic ms Response: • Relaxation of the same ms • Contraction of antagonistic group of ms.
Physiological significance: • Protective reaction which prevent tearing of")
Inverse Stretch Reflex Significance GTR: a)Physiological significance: • Protective reaction which prevent tearing of the ms or avulsion of its tendon from its bony attachment when the ms is overstretched.
Clinical significance: (clasp knife effect) • Demonstrated clinically by")
Inverse Stretch Reflex Significance GTR: b)Clinical significance: (clasp knife effect) • Demonstrated clinically by passive flexion of a spastic limb (e. g. in upper motor neuron lesions) at its main joint. • As the limb is flexed, an initial resistance occurs due to contraction of this ms a result of the stretch reflex. • With persistent flexion, at a certain point, GTR is excited→ sudden disappearance of the initial resistance → the limb flexes easily, as occurs during closing-of a pocket knife→ clasp knife effect. • E. g. Flexion of knee and ankle

Tendon Jerk

Tendon Jerks Def. , • Rapid contraction followed by relaxation of a ms due to sudden stretching of that ms by tapping on its tendon using a medical hammer Mechanism: • It is a dynamic type of the stretch reflex

The Tendon Reflex To brain 6 Primary afferent neuron stimulates inhibitory interneuron 4 Primary afferent neuron stimulates alpha motor neuron to extensor muscle 1 ry endings 3 Primary afferent neuron excited Nuclear bag Alpha MNs 7 Interneuron inhibits alpha motor neuron to flexor muscle 5 Alpha motor neuron stimulates extensor muscle to contract Ms contraction Sudden stretch 2 Muscle spindle stimulated 1 Extensor muscle stretched Flexor muscle 8 (antagonist) relaxes

Tendon Jerks
 Stoppage")
Tendon Jerks • Cause of relaxation after contraction in the tendon jerk: a) Stoppage of discharge from the ms spindles. b) Stimulation of the Golgi tendon organs. c) Stimulation of the Renshaw’s Cells.

Examples of Tendon Jerks Jerk Biceps jerk Triceps jerk Knee jerk Ankle jerk Jaw jerk Center Limb position Tendon Response C 5, 6 The elbow is Tapping on biceps Flexion of 120° tendon the forearm C 6, 7 The elbow is Tapping on triceps Extension of 90° tendon directly the forearm L 2, 3 & 4 knee is semi Tapping on Extension of flexed by patellar tendon the knee seating with the leg to be tested crossing over other S 1, 2 feet slightly Tapping dorsiflexed tendoachilles on Plantar flexion. Trigemin Mouth slightly Tapping on chin al nerve opened Closure mouth of


Biceps Jerk

Triceps Jerk

Knee Jerk

Ankle Jerk

Tendon Jerk Reinforcement of the tendon jerks • Response of the tendon jerks can be reinforced by facilitating the spinal centers. • Can be done by either; a) Jendrassik's maneuver → ask the patient to hook his fingers or to clench his teeth→ send signals from the contracted ms which stimulating γ-MNs. b) Distracting patient’s attention→ prevents any voluntary inhibition of the reflex.

Clinical Significance of TJ 1. Localization of spinal cord lesions: • Loss of TJ means the lesion in its center e. g. ankle jerk is lost in sacral region lesion. 2. Assessment of the ms tone : • In hyperreflexia (exaggerated tendon jerks) → hypertonia (↑ms tone). • In hyporeflexia (↓ed tendon jerks) → hypotonia (↓ms tone). • In areflexia (lost tendon jerks) → atonia (lost ms tone).

Clinical Significance of TJ 3. Assessment of the integrity of pathway of stretch reflex: so areflexia or absent tendon jerk may be due to; Site of lesion Condition • Afferent lesion Tabes dorsalis • Center (AHC) lesion Poliomyelitis • Efferent lesion Trauma or neuritis 4. Assessment of the state of Supraspinal centers: Hyperactive(exaggerated) TJ Hypoactive (decreased) TJ Physiological causes Anxiety and nervousness Sleep and anaesthesia Pathological causes UMNL Lesion in area 6 Tetany and hyperthyroidism Paleocerebellum lesion LMNL Lesion in area 4 Hypothyroidism Neocerebellar syndrome

Pendular Knee Jerk • Occurs in the neocerebellar syndrome and chorea. • Characterized by hyporeflexia & hypotonia • Knee jerk is weak than normal and during relaxation of the quadriceps ms, the leg falls like a dead weight(due to hypotonia) & swings for sometime like a pendulum before resting.

Clonus Def. • Alternating regular rhythmic contractions with incomplete relaxations of a ms (its MNs is in a state of facilitation) in response to sudden maintained stretch. Cause: • UMNL
 Ankle Clonus: • Produced by sudden maintained dorsiflexion of the foot")
Clonus Types 1) Ankle Clonus: • Produced by sudden maintained dorsiflexion of the foot leads to regular rhythmic planter flexions due to rhythmic contractions of soleus and gastrocnemius muscles. 2) Knee Clonus: • Produced by the sudden downward displacement of the patella rhythmic oscillations of the patella.


Clonus Mechanism of clonus: • Clonus is the result of a stretch reflex - inverse stretch reflex sequence, which occurs as follows : • Sudden stretch of the ms results in its contraction through the stretch reflex. • This is followed by relaxation due to; a) Stoppage of impulse discharge from the ms spindles. b) Initiation of an inverse stretch reflex due to stimulation of the GTOs. • As stretch is maintained, a new stretch reflex occurs (helped by the state of excessive spinal facilitation), and the cycle is repeated.

Somatic Motor System

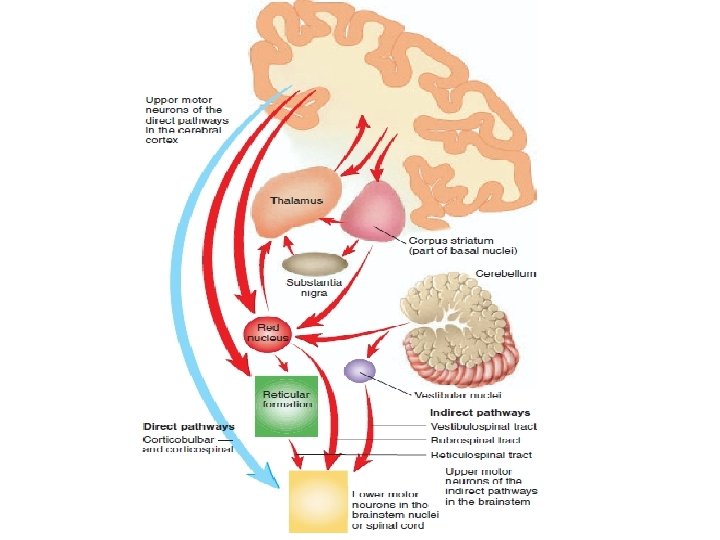
Somatic Motor System Higher Motor Centers in CC Midbrain Descending Motor Tracts L A Lower MNs In Brain Stem Pons Medulla Motor centers in brain stem e. g. RF Lower MNs in AHCS Spinal Cord

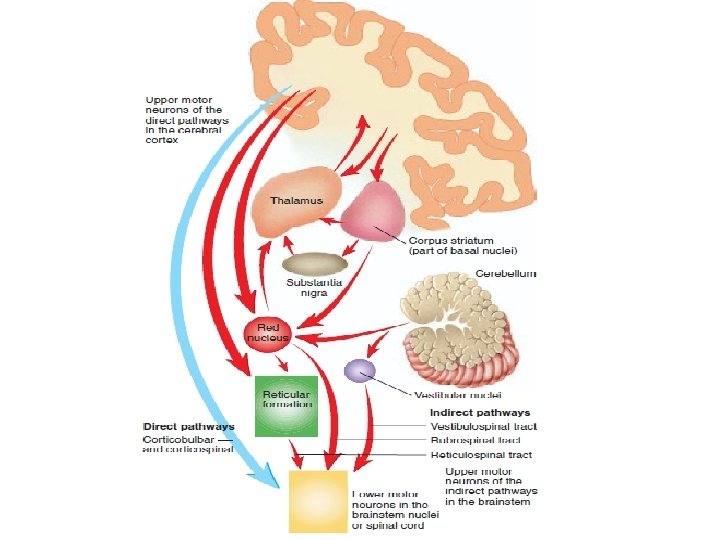
Somatic Motor System • Consists of 2 sets of motor neurons; 1. Upper Motor neurons: • Cell bodies are present in motor areas of cerebral cortex and other motor centers in brain stem • Axons form descending motor tracts 2. Lower motor neurons: • Cell bodies are present in AHCs of spinal cord or motor nuclei of cranial nerves • Axons form peripheral nerves that supply skeletal ms

Upper Motor Neuron Higher Motor Centers in CC Midbrain Upper Motor Neuron L A Brain Stem Nuclei Pons Medulla Motor centers in brain stem e. g. RF AHCS Spinal Cord

Lower Motor neurons Left Internal Capsule Midbrain L A Somatic Motor nuclei of cranial nerves Pons Medulla AHCs Spinal Cord
")
Cortical Motor Areas (Motor Cortex)

Motor Cortex • Initiation and performance of voluntary movements are the result of motor commands signals from the motor cortex to the lower motor centers via the descending motor tracts • Motor cortex is located in the frontal lobe, and comprises; 1. Primary motor area (area 4) 2. Premotor area (area 6) 3. Supplemental motor area

Area 4 Premotor area 4 6
")
Primary Motor Area (4)
 Site: §Precentral gyrus in frontal lobe Precentral gyrus Central sulcus")
Primary Motor Area (MI) Site: §Precentral gyrus in frontal lobe Precentral gyrus Central sulcus
 Body representation: 1. Contralateral: i. e. Body ms from the")
Primary Motor Area (MI) Body representation: 1. Contralateral: i. e. Body ms from the Rt side of the body is represented in the left hemisphere and Lt half of body is represented in Rt hemisphere N. B. some facial muscles are represented bilaterally

Primary Motor Area Body representation: 2. Inverted: i. e. the ms of the face are controlled by the lowermost part of area 4 & muscles of the lower limbs controlled by the upper most part of area 4

Primary Motor Area Body representation: 3. Ms involved in fine voluntary movements are represented by relatively large areas than those involved in gross movements Homunculus
 Connections: Premotor and supplemental motor areas. a) Afferents: Area 4")
Primary Motor Area (MI) Connections: Premotor and supplemental motor areas. a) Afferents: Area 4 Visual and auditory areas Prefrontal area Proprioceptors (Sensory Feedback) Basal ganglia and cerebellum.
 Efferents: Area 4 on opposite side Red nucleus and")
Primary Motor Area Connections: b) Efferents: Area 4 on opposite side Red nucleus and RF (moderate No. of fibers) Corticobulbospinal tract (30%) Basal ganglia and cerebellum (Large No. of fibers.

Primary Motor Area Functions: 1. Initiation of voluntary movements done by the distal limb muscles 2. Facilitatory to the tone of the distal muscles
 of the distal limb")
Primary Motor Area Lesion: 1. loss of voluntary movements (paralysis) of the distal limb muscles on opposite side 2. Hypotonia and inhibition of tendon jerks 3. Babinski’s sign with dorsiflexion of the big toe only
")
Premotor Area (6)
 Site: • Frontal lobe in front of area 4 Premotor area")
Premotor Area (6) Site: • Frontal lobe in front of area 4 Premotor area
 Body representation: Contralateral and inverted")
Premotor Area (6) Body representation: Contralateral and inverted
 Connections: Area 4 Supplemental area Area 6 Basal ganglia and cerebellum.")
Premotor Area (6) Connections: Area 4 Supplemental area Area 6 Basal ganglia and cerebellum. Corticobulbospinal tract (30%)

Premotor Area • 1. Functions: shares in planning of complex movements together with area supplemental motor area 2. initiates the gross movements as those done by the trunk 3. with B. G. involved in postural adjustment during voluntary distal movements 4. inhibitory effect on muscle tone 5. with basal ganglia, initiate & control the automatic associative movements

Premotor Area Functions: contains special areas in area 6

Premotor Area Broca’s area

Premotor Area Hand skills Head rotation Eye movements area

Primary Motor Area • Lesion: 1. impairment of complex movements or paresis 2. Hypertonia and exaggeration of tendon jerks 3. Loss of automatic associative movements 4. Babinski’s sign with fanning of the lateral four toes only 5. Motor aphasia 6. Motor apraxia

Supplemental Motor Area

Supplemental Motor Area Site: • Upper medial side of frontal lobe above area 6 supplemental area

Supplemental motor Area Connections: Sup p. Area 4 Premotor area Basal ganglia and cerebellum. Corticobulbospinal tract
Evokes complex movements which often involve both sides of the")
Supplemental Motor Area Functions: 1)Evokes complex movements which often involve both sides of the body e. g. : causing both hands to perform a motor act together. 2) With the premotor area (6) in providing suitable background for the performance of the fine skilled movements by hands and fingers that are mediated by the C. B. S tract. 3)Shares in the planning and programming of the complex movements with area 6.

Descending Motor Tracts
 Pyramidal and extrapyramidal tracts: •")
Descending Motor Tracts Classified by 2 ways ; a) Pyramidal and extrapyramidal tracts: • If the tract passes through the pyramids of the medulla→ pyramidal tract. • If the tract does not pass through the medullary pyramids→ extrapyramidal tract.

Pyramidal Tract

Extrapyramidal Tracts

Medial and Lateral Motor System Medial motor system Lateral motor system
 Medial and lateral motor system: • i) Medial motor")
Descending Motor Tracts • b) Medial and lateral motor system: • i) Medial motor system→ system composed of tracts that terminate primarily on the ventromedial neurons → innervate axial and girdle ms → concerned with postural control. • ii) Lateral motor system→ system composed of tracts that terminate primarily on the lateral neurons → innervate distal ms of the limbs → concerned with control of fine voluntary movements.

Descending Motor Tracts q 5 important sets of descending motor tracts, named according to the origin of their cell bodies and their final destination: 1) Corticobulbospinal tract (= Pyramidal tract) 2) Rubrospinal tract, 3) Reticulospinal tracts, 4) Vestibulospinal tracts 5) Tectospinal tract Extrapyramidal tracts

Pyramidal Tract or Corticobulbospinal Tract

Pyramidal Tract Motor areas, somatic sensory areas Corticonuclear tract Left Internal Capsule Midbrain L A Corticobulbar tract Pons Medulla Corticospinal tract Spinal Cord
 → 30% 2. Premotor")
Pyramidal Tract • Origin: 1. Primary motor area (area 4) → 30% 2. Premotor and supplemental areas → 30% 3. Somatic Sensory areas → 40%

Pyramidal Tract • Origin: Area 4 Premotor area and supplemental motor area 30 % Area 3, 1, 2 and Area 5, 7, 30 % 40 %
 Corticospinal tract : from cortex to spinal cord")
Pyramidal Tract • Divisions: • 1) Corticospinal tract : from cortex to spinal cord • 2) Corticonuclear tract: from cortex to cranial nerves nuclei (3, 4, 6) that supply extraocular muscles • 3) Corticobulbular tract: from cortex to other cranial nerves (5, 7, 9, 10, 11, 12) of brain stem

M 1 Pyramidal Tract 4 Genu Anterior Limb Corticospinal Tract Posterior Limb Left Internal Capsule Midbrain Pons Pyramidal Decussation Mid Medulla Caudal Medulla Spinal Cord
 90% cross to the opposite side and descend in the")
Corticospinal Tract • (a) 90% cross to the opposite side and descend in the lateral column of the spinal cord as lateral corticospinal tract→ terminate on lateral AHCs →innervate the distal ms • (b) 10% not cross → descend ipsilaterally as ventral corticospinal tract. • About 9% of these fibers cross and terminate on medial AHCs → innervate the axial muscles of the opposite side. • Only 1% of the fibers terminate on the A. H. Cs of the same side (bilateral innervations as respiratory muscles).

CC • Pathway: Internal capsule Medulla Lateral CST Ventral or medial CST Spinal cord

M 1 Pyramidal Tract Corticobulbar Tract FA L Left Internal Capsule VMidbrain PONS Upper Face Lower Face MEDULLA F V VII Pons VII IX IX X X XII Ipsilateral Side Corticobulbar Tract is crossed and uncrossed EXCEPT to lower motor neurons which control lower half of the face and tongue are crossed only. Mid Medulla Contralateral Side LOWER MOTOR NEURON NUCLEI Caudal Medulla Spinal Cord

Area 8 Pyramidal Tract Corticonuclear Tract FA L Left Internal Capsule Midbrain PONS III Midbrain IV VI F III IVPons VI LMN Supplying eye muscles Mid Medulla Caudal Medulla Spinal Cord Ipsilateral Side Contralateral Side

Pyramidal Tract • Functions: • The C. B. S tract is primarily concerned with the mediation of voluntary motor commands from the cerebral cortex to lower motor centers: • a- Corticonuclear tract controls the extraoccular ms. • b- Corticobullar tract controls the ms of lower part of the face and tongue which are involved in articulate speech. • c-Lateral corticospinal tract controls distal ms that subserve skilled movements as those used in manipulation by hands and fingers.
 Medial C. B. S tract controls axial ms")
Pyramidal Tract • Functions: • 2) Medial C. B. S tract controls axial ms concerned mainly with regulation of posture. • 3) C. B. S tract is also facilitatory to the tone of the distal limb muscles.

Descending Motor Tracts
Pyramidal and extrapyramidal tracts:")
Descending Motor Tracts They are classified by 2 ways ; a)Pyramidal and extrapyramidal tracts: • If the descending motor tract passes through the pyramids of the medulla→ pyramidal tract. • If the descending motor tract does not pass through the medullary pyramids→ extrapyramidal tract.

Pyramidal Tract

Extrapyramidal Tracts

AHCs Medial motor system Lateral motor system
 Medial and lateral motor system: • i) Medial motor")
Descending Motor Tracts • b) Medial and lateral motor system: • i) Medial motor system→ system composed of tracts that terminate primarily on the ventromedial neurons → innervate axial and girdle ms → concerned with postural control. • ii) Lateral motor system→ system composed of tracts that terminate primarily on the lateral neurons → innervate distal ms of the limbs → concerned with control of fine voluntary movements.

q. There are 5 important sets of descending motor tracts, named according to the origin of their cell bodies and their final destination: 1) Corticobulbospinal tract (= Pyramidal tract) 2) Rubrospinal tract, 3) Reticulospinal tracts, 4) Vestibulospinal tracts 5) Tectospinal tract Extrapyramidal tracts

Pyramidal Tract or Corticobulbospinal Tract

Pyramidal Tract Motor areas, somatic sensory areas Corticonuclear tract Left Internal Capsule Midbrain L A Corticobulbar tract Pons Medulla Corticospinal tract Spinal Cord
 → 30% 2. Premotor")
Pyramidal Tract • Origin: 1. Primary motor area (area 4) → 30% 2. Premotor and supplemental areas → 30% 3. Somatic Sensory areas → 40%

Pyramidal Tract • Origin: Area 4 Premotor area and supplemental motor area 30 % Area 3, 1, 2 and Area 5, 7, 30 % 40 %
 Corticospinal tract : from cortex to spinal cord")
Pyramidal Tract • Divisions: • 1) Corticospinal tract : from cortex to spinal cord • 2) Corticonuclear tract: from cortex to cranial nerves nuclei (3, 4, 6) that supply extraocular muscles • 3) Corticobulbular tract: from cortex to other cranial nerves (5, 7, 9, 10, 11, 12) of brain stem

M 1 Pyramidal Tract 4 Genu Anterior Limb Corticospinal Tract Posterior Limb Left Internal Capsule Midbrain Pons Pyramidal Decussation Mid Medulla Caudal Medulla Spinal Cord
 90% cross to the opposite side and descend in the")
Corticospinal Tract • (a) 90% cross to the opposite side and descend in the lateral column of the spinal cord as lateral corticospinal tract→ terminate on lateral AHCs →innervate the distal ms • (b) 10% not cross → descend ipsilaterally as ventral corticospinal tract. • About 9% of these fibers cross and terminate on medial AHCs → innervate the axial muscles of the opposite side. • Only 1% of the fibers terminate on the A. H. Cs of the same side (bilateral innervations as respiratory muscles).

CC • Pathway: Internal capsule Medulla Lateral CST Ventral or medial CST Spinal cord

M 1 Pyramidal Tract Corticobulbar Tract FA L Left Internal Capsule VMidbrain PONS Upper Face Lower Face MEDULLA F V VII Pons VII IX IX X X XII Ipsilateral Side Corticobulbar Tract is crossed and uncrossed EXCEPT to lower motor neurons which control lower half of the face and tongue are crossed only. Mid Medulla Contralateral Side LOWER MOTOR NEURON NUCLEI Caudal Medulla Spinal Cord

Area 8 Pyramidal Tract Corticonuclear Tract FA L Left Internal Capsule Midbrain PONS III Midbrain IV VI F III IVPons VI LMN Supplying eye muscles Mid Medulla Caudal Medulla Spinal Cord Ipsilateral Side Contralateral Side

Pyramidal Tract • Functions: • The C. B. S tract is primarily concerned with the mediation of voluntary motor commands from the cerebral cortex to lower motor centers: • a- Corticonuclear tract controls the extraoccular ms. • b- Corticobullar tract controls the ms of lower part of the face and tongue which are involved in articulate speech. • c-Lateral corticospinal tract controls distal ms that subserve skilled movements as those used in manipulation by hands and fingers.
 Medial C. B. S tract controls axial ms")
Pyramidal Tract • Functions: • 2) Medial C. B. S tract controls axial ms concerned mainly with regulation of posture. • 3) C. B. S tract is also facilitatory to the tone of the distal limb muscles.

THANKS
- Slides: 103