URINARY SYSTEM By Sindhu Priya E S Introduction

URINARY SYSTEM By - Sindhu Priya E S

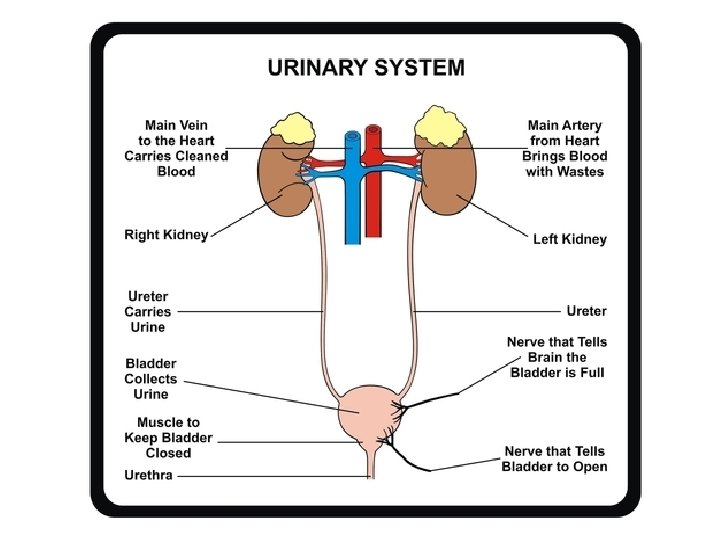
Introduction Urinary system is the main excretory system of the body 2 kidneys, which secrete urine 2 ureters, which convey the urine from the kidneys to the urinary bladder 1 urinary bladder where urine collects and is temporarily stored 1 urethra through which the urine is discharged from the urinary bladder to the exterior.

kidneys Bean shaped organs 11 cm long, 6 cm wide, 3 cm thick and weigh 150 g They held in position by a mass of fat Right kidney is usually slightly lower than the left Renal fascia

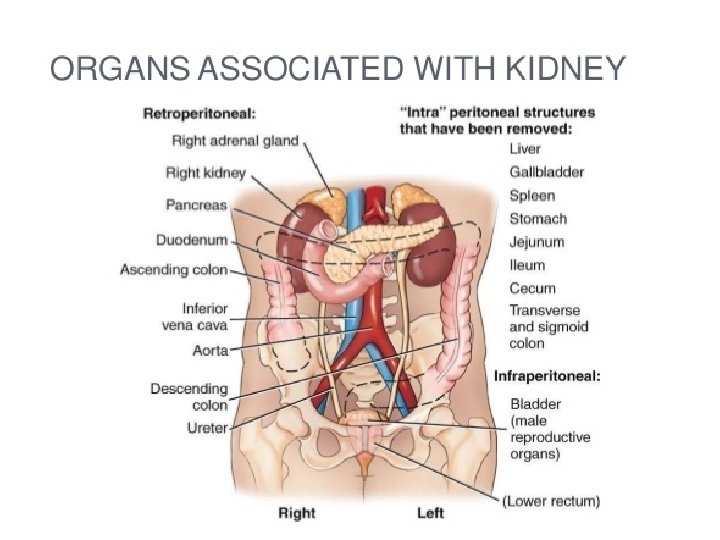
Organs associated with kidneys Right kidney Superiorly — the right adrenal gland Anteriorly —the right lobe of the liver, the duodenum and the hepatic flexure of the colon Posteriorly —the diaphragm, and muscles of the posterior abdominal wall Left kidney Superiorly — the left adrenal gland Anteriorly —the spleen, stomach, pancreas, jejunum and splenic flexure of the colon Posteriorly —the diaphragm and muscles of the posterior abdominal wall

Gross structure of kidney Fibrous capsule – Outer covering of kidney Cortex – Outer Reddish brown layer Medulla –Inner layer with Pyramids Hilum - Notch Renal pelvis Calysis

Section of human kidney

Microscopic structure of kidney Nephron: Functional unit � Renal corpuscle Glomerulus Glomerular � Renal capsule tubule Proximal convoluted tubule Loop of henley (AL & DL) Distal convuluted tubule

Juxtaglomerular Apparatus

Cell types present in nephron

Cell types present in nephron

Ureters 25 -30 cm long tubes connecting kidneys to urethra Three layers � Adventitia – Outer fibrous connective tissue � Muscularis – Middle muscle layer � Mucosa- Inner mucosal layer Function � propels urine from kidney to uethra

Urinary bladder Hollow, pear shaped distensible organ Holds 700 -800 ml of urine Structure � Adventitia – Outer areolar connective tissue � Muscularis – Middle detrusor muscles � Mucosa- Inner mucosal epithelium

Urethra Terminal canal portion of the urinary bladder extending from the neck to the exterior that drains urine It also contains three layers Urine passes from External urethral orifice guarded by external urethral sphincter

Functions of the kidneys Removal of metabolic wastes : urea, uric acid, creatinine, bilirubin Regulation of fluid and electrolyte balance : Electrolytes and water Regulation of acid-base balance : H+ and HCO 3 - Maintenance of blood pressure : Renin release Regulation of erythropoiesis : Erythropoietin release

Blood flow in kidney

Physiology of urine formation Three stages � Glomerular filtration � Selective reabsorption � Tubular secretion

a. Filtration takes place through the semipermeable walls of the glomerulus and glomerular capsule Water and large number of small molecules pass through, although some are reabsorbed later Glomerular filtrate is formed by pressure gradient The volume of filtrate formed by both kidneys per minute is termed the glomerular filtration rate (GFR) – 125 m. L/min

Constituents of Glomerular filtrate GFR – 125 m. L/min; 180 L per day But 1 -1. 5 L urine excreted per day What happens to 178. 5 – 179 L ?

b. Reabsorption Selective reabsorption is the process by which the useful substances and nutrients of the glomerular filtrate are selectively reabsorbed into the blood Water, Na, Cl, glucose, aminoacids, vitamins, hormones are reabsorbed by active and passive process from PCT, Loop of Henley, DCT and Collecting duct

Reabsorption
, K+ , H+ are secreted into the")
c. Tubular secretion Foreign materials (penicillin, aspirin), K+ , H+ are secreted into the DCT/collecting duct to form urine

Summary of urine formation

Reabsorption • PCT - Glucose, AA, Proteins, vitamins, Na +, Cl -, HCO 3 - , Urea, K +, Ca +, Mg 2+, water • Loop of Henley - Na +, K +, Cl-, water • DCT - Na +, Cl-, HCO 3 - , Water • CD - water, urea Secretion • PCT - Urea, uric acid, creatinine, drugs, H+ , NH 4 + • Loop of Henley - Urea • DCT - H+ , K+ , NH 4+

Composition of Human urine Water Urea Uric acid Creatinine Ammonia Sodium Potassium Chlorides Phosphates Sulphates Oxalates 96% 2% Clear amber colour Urobilin p. H- 6 (4. 5 -8) SG- 1020 -1030 Volume-1 to 1. 5 L per day

Micturition is the discharge of urine from the urinary bladder to the outside of the body through urethra It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters
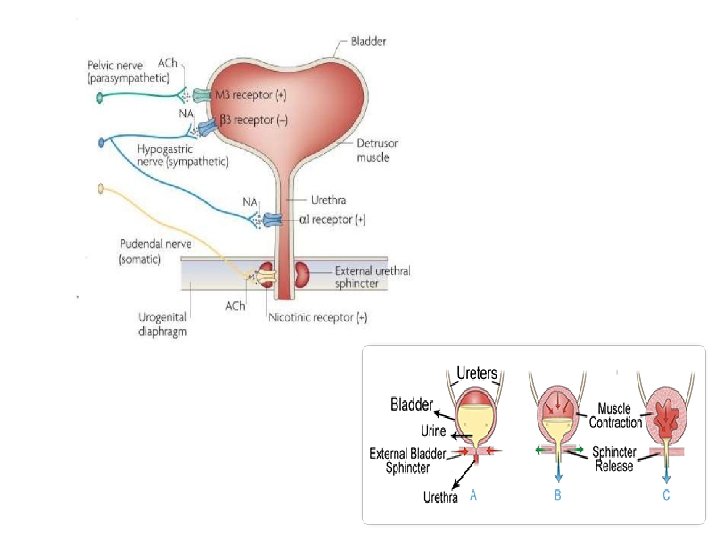

Regulation of micturition

Role of Kidneys in Acid Base Balance � Excretion of H+ and Formation of NH 4+ H+ + HPO 32 H 2 PO 3 H+ + NH 3+ NH 4+ � Reabsorption H+ + HCO 3 - H 2 O of HCO 3 H 2 CO 3 CO 2 + H+ excreted as H 2 PO 3 - and NH 4+ HCO 3 - absorption regulates blood CO 2

Absorption of HCO 3 -

Feedback mechanism of kidneys to regulate Acid-Base balance Acidosis � Reabsorption of HCO 3� Secretion of H+ from CD � Formation of NH 3+ Alkalosis � Excretion of HCO 3� Reducing secretion of H+ from CD � Reducing glutamate metabolism and Formation of NH 3+
")
Renin Angiotensin system (RAS)

Regulation of blood volume and blood pressure by RAAS

Renal function tests Glomerular function tests or clearance tests Inulin clearance test Creatinine clearance test Urea Clearance test Tubular function tests Urea Concentration Urine acidification Analysis of blood / serum Estimation of blood urea, serum creatinine, protein & electrolyte

Urine examination Volume, p. H, Specific gravity, Osmolality, Presence of certain abnormal constituents ( Proteins, blood, ketone bodies, glucose) Clearance tests C= uxv p Creatinine clearance (145 ml/minute) Urea clearance (75 ml/minute)

Symptoms of Kidney Failure Weakness Lethargy Shortness of breath Widespread edema Anemia Metabolic acidosis / Metabolic alkalosis Heart arrhythmias Uremia (high urea level in the blood) Loss of appetite Fatigue Excessive urination / Oliguria

Disorders of kidneys 1. 2. 3. 4. 5. 6. 7. 8. 9. Glomerulonephritis Nephrotic syndrome Acute renal failure Diabetic kidney Acute pyelonephritis Chronic renal failure Urolithiasis Renal tumours Urinary Tract Infections (UTI)

Glomerulonephritis It is the inflammatory condition of the glomerulus. In many cases immune complexes lodge in the walls of the glomeruli they often cause an inflammatory response that impairs glomerular function Effects: Hematuria, asymptomatic proteinuria, acute nephritis, chronic renal failure, nephrotic syndrome

Nephrotic syndrome This is not a disease in itself but is an important feature of several kidney diseases. The main characteristics are: • Marked proteinuria • Hypoalbuminaemia • Generalised oedema • Hyperlipidaemia.

Diabetic kidney Renal failure is the cause of death in 10% of all diabetics and up to 50% of cases of the insulindependent (type I) diabetes mellitus. There is damage to large and small blood vessels in many parts of the body. The effects include � progressive glomerulosclerosis followed by atrophy of the tubules � acute pyelonephritis with papillary necrosis � atheroma of the renal arteries and their branches, leading to renal ischaemia and hypertension � nephrotic syndrome

Acute renal failure It is the condition where there is a sudden and severe reduction in the glomerular filtration rate and kidney function that is usually reversible over days or weeks when treated Causes: prerenal: the result of reduced renal blood flow, especially severe and prolonged shock � renal, or parenchymal: damage to the kidney itself due to, e. g. , acute tubular necrosis, glomerulonephritis � post-renal: obstruction to the outflow of urine, e. g. tumour of the bladder, uterus or cervix, large calculus in the renal pelvis. �

Chronic renal failure It is the condition when irreversible damage occurs to nephrons which is so severe that 75% of renal function has been lost and the kidneys cannot function effectively. Causes: glomerulonephritis, diabetes mellitus, chronic pyelonephritis and hypertension. Effects: Uraemia, polyuria, acidosis, electrolye imbalance, anaemia, hypertension
 form in the kidneys and bladder when")
Renal calculi or kidney stones Calculi (stones) form in the kidneys and bladder when urinary constituents normally in solution are precipitated. The solutes involved are oxalates, phosphates, urates and uric acid. Stones usually consist of more than one substance, deposited in layers. Causes: Dehydration, p. H of urine, Infection, metabolic conditions such as gout
- Slides: 44