THE SKIN COLOUR DISORDERS OF PIGMENTATION Skin Colour




, X linked recessive (ocular type) Defect or failure of")




















 Tiny (<0. 5 cm), discrete brown macules Common in fair skinned Appear")



. Acquired hypermelanosis of the sun exposed skin.")






- Slides: 45
THE SKIN COLOUR & DISORDERS OF PIGMENTATION
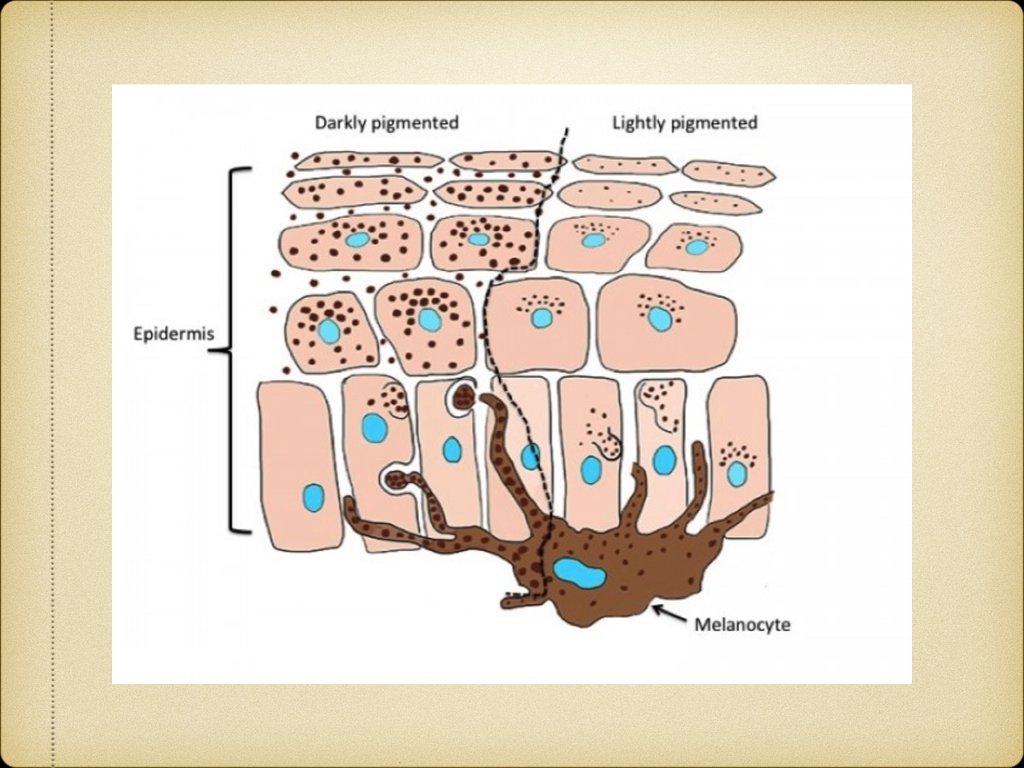
Skin Colour Determined by 1. Melanin 2. Hemoglobin 3. Carotenoids Constitutive skin colour Facultative skin colour
HYPOMELANOTIC DISEASES CLASSIFICATIONS: Congenital/Acquired Diffuse/Focal Hypopigmented/Depigmented Melanopenic/Melanocytopenic Etiological classification
Classification of hypopigmented diseases Genetic & Developmental: Nevus anemicus, nevus depigmentosus, albinism Endocrine: Hypothyroidism, hypopituitarism Nutritional: Kwashiorkor Infectious: P. versicolor, leprosy Post-Inflammatory: Psoriasis, P. alba Drugs & Chemicals: Hydroquinone, Steroids, Arsenic Miscellaneous: Vitiligo, Burns, Trauma
ALBINISM Autosomal recessive (oculocutaneous type), X linked recessive (ocular type) Defect or failure of synthesis in melanin synthesis Involves skin, hair & eyes Absence of pigmentation since birth Photophobia Sunburns & skin cancers common
TUBEROUS SCLEROSIS Autosominal dominant, neurocutaneous syndrome Skin lesions, mental retardation and epilepsy Skin lesions are ash-leaf macules, angiofibromas and shagreen patches Ash-leaf macules - present at birth in>90% cases, so important in early diagnosis Oval or ash-leaf shaped, hypopigmented macules, made prominent in Wood’s lamp
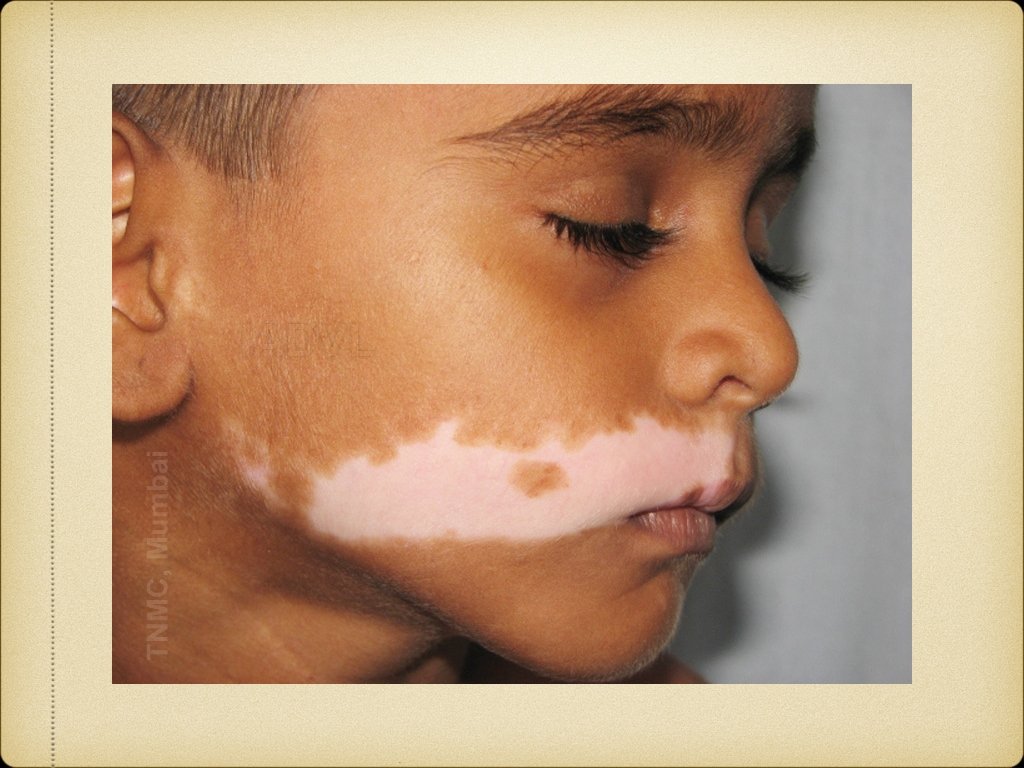
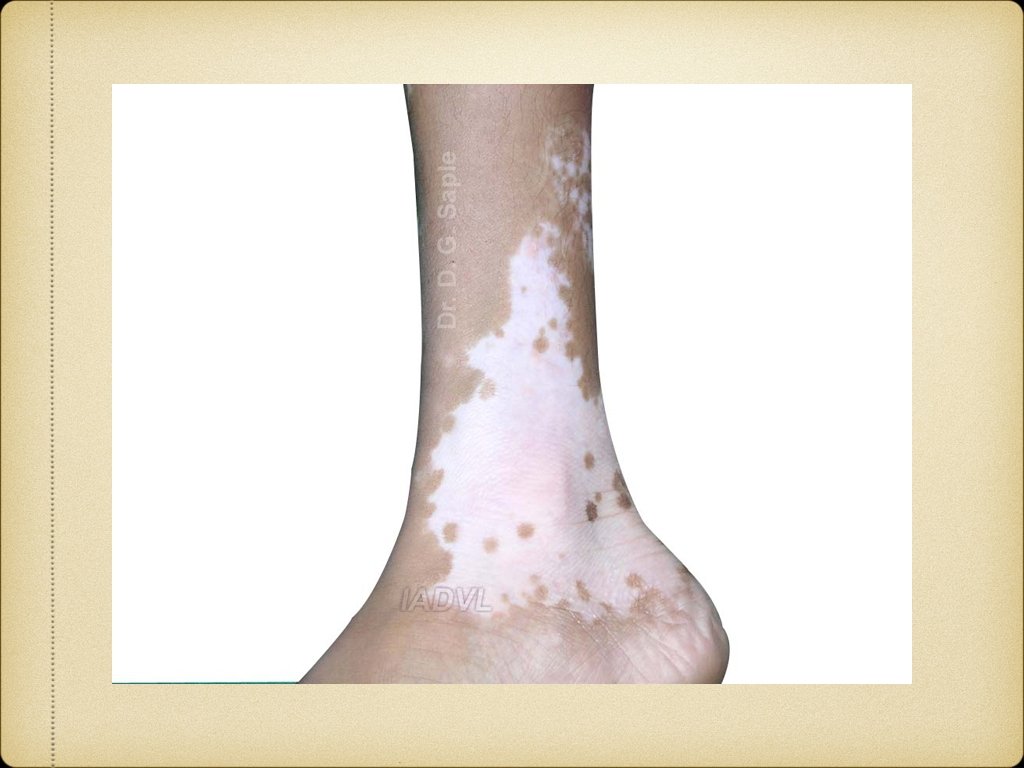
VITILIGO Acquired primary, usually progressive, melanocytopenia of unknown etiology Degeneration and disappearance of melanocytes Clinically manifested by circumscribed achromic macules associated with leukotrichia Common sites include the extensor body surfaces as the pretibial regions, sides of ankles, knees, elbows and skin overlying digits and periorificial areas. Local exacerbating factors include causes like trauma, itching and friction with presence of Koebner’s phenomenon.
Etiopathogenesis of Vitiligo Autoimmune hypothesis Neural hypothesis Free radical hypothesis Antioxidant reduction hypothesis Composite hypothesis
Classification 1. Generalized Vitiligo vulgaris Vitiligo universalis 2. Localised Focal Segmental Acrofacial Mucosal
Course of disease & prognosis Unpredictable course and slow progression Poor prognostic factors 1. Lesions on resistant sites 2. Long duration 3. Family history 4. Leucotrichia 5. Old age 6. Associated autoimmune diseases 7. Injudicious use of photo chemotherapy
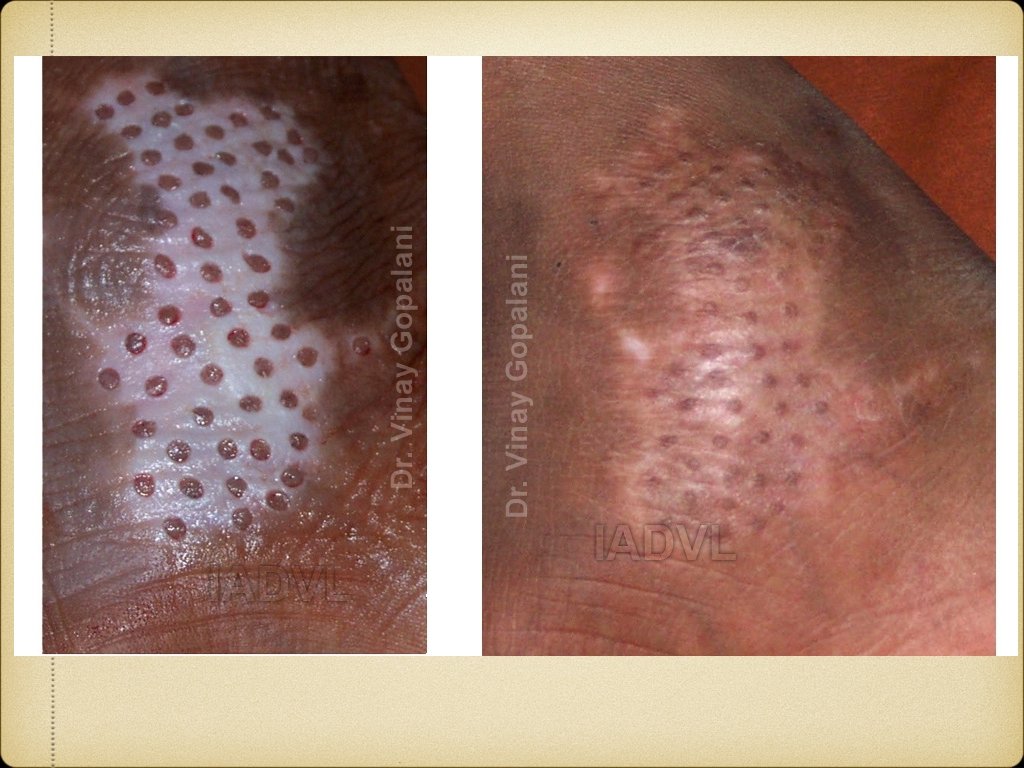
Management 1. Medical Topical agents: Steroids, tacrolimus, calcipotriol Systemic agents: Steroids, Azathioprine, Cyclosporine Phototherapy: PUVA, PUVAsol, NB-UVB 2. Surgical Tattooing, therapeutic wounding Grafting: Split thickness, punch, blister 3. Cosmetic camouflage 4. Destruction of hyperpigmented area
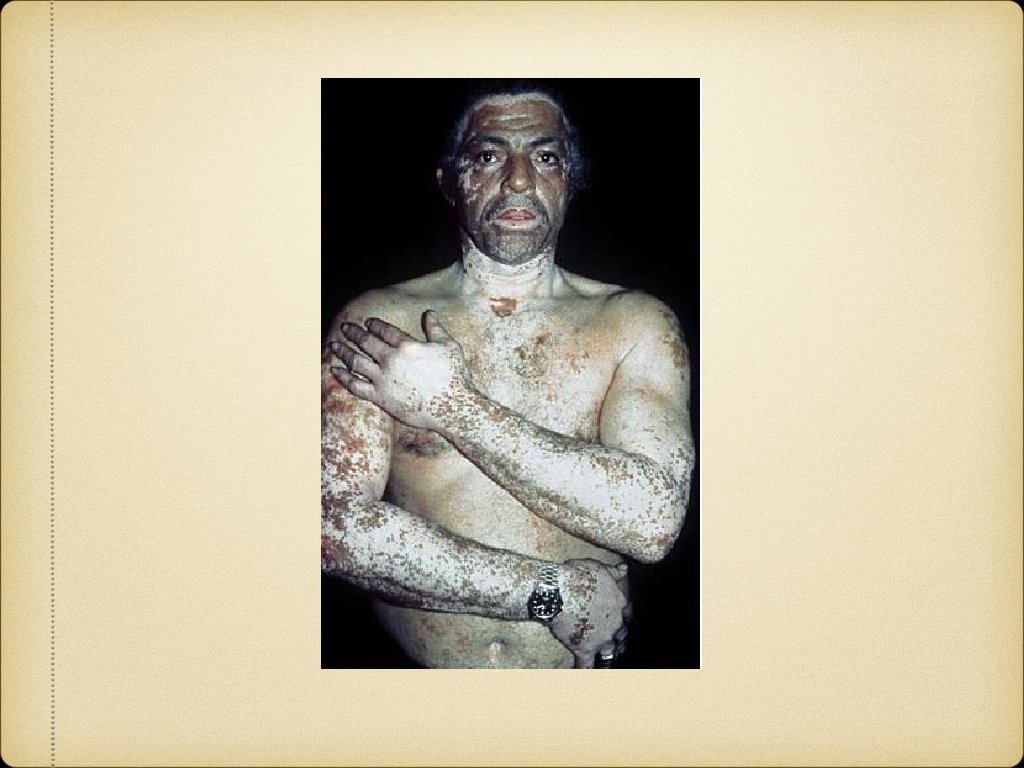
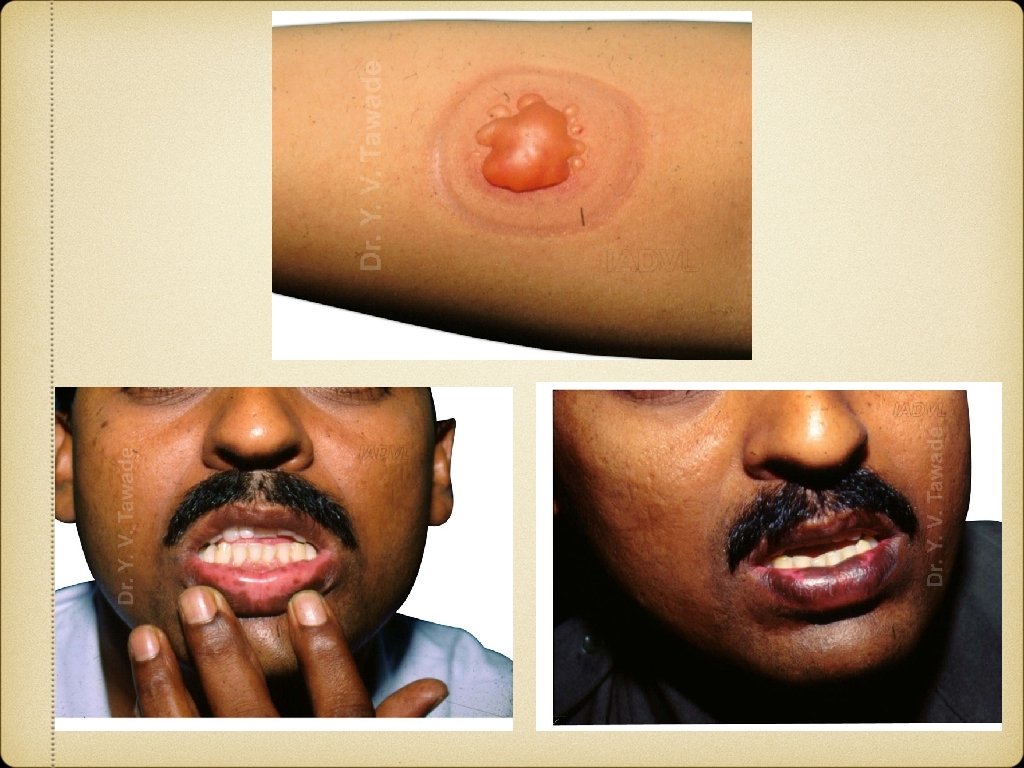
CHEMICAL LEUCODERMA
IDIOPATHIC GUTTATE HYPOMELANOSIS
POST INFLAMMATORY HYPO PIGMENTATION
DISORDERS OF HYPERPIGMENTATION Epidermal: dark brown Increase in melanin Increase in melanocyte Dermal: blue-grey Epidermal melanin in dermis Melanin from dermal melanocytes
Epidermal pigmentation Physiological: Tanning Genetic & Developmental: Melanocytic nevus, Lentigines, Ephelides, Xerodermal pigementosum Post inflammatory: LP, Psoriasis Infection: P. versicolor Nutritional: Pellagra, Vit B 12 deficiency Endocrine: Addison’s disease, Melasma, Acromegaly Neoplastic: Melanoma, Pigmented BCC Physical: Trauma, Radiodermatitis
Dermal pigmentation Genetic & Developmental: Mongolian spots, Nevus of Ota Inflammatory: Fixed drug eruption Drugs & Chemicals: Minocycline, OCPs, Clofazamine Endocrine: Melasma Infections: Syphilis Neoplastic: melanoma mets Physical: Post traumatic, burns Metabolic: Amyloidosis Miscellaneous: Chronic nutritional deficiency
EPHELIDES (FRECKLES) Tiny (<0. 5 cm), discrete brown macules Common in fair skinned Appear in childhood on sun exposed parts; lighten in absence of sun exposure Melanocytes are not increased in number but are hyperactive
FIXED DRUG ERUPTION NSAIDs, antibiotics, barbiturates etc. Reddish brown macule → edematous → desquamation → pigmentation Recurs at same site on rechallenge May become generalised or blistering Melanin is increased in epidermis and dermis (melanophages)
POST INFLAMMATORY HYPERPIGMENTATION After resolution of specific eruptions Common after lichen planus, atopic dermatitis, acne vulgaris, contact dermatitis, psoriasis, pyodermas etc. Discrete macules exactly on the sites previously affected by eruptions May persist for months
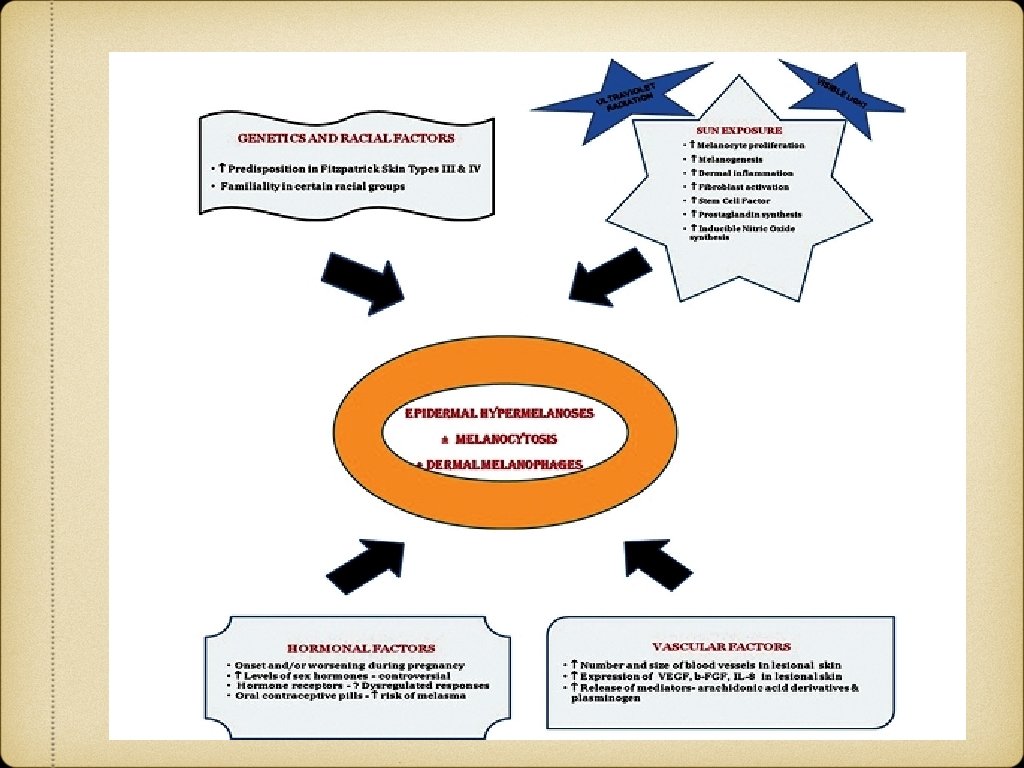
MELASMA Greek “melas” = black, “chloazein” (green). Acquired hypermelanosis of the sun exposed skin. M: F=1: 9 Much more common in constitutionally darker skin types Most common pigmentary disorder among Indians
Clinical Features Presents as symmetric, hyperpigmented macules having irregular, serrated, and geographic borders. Distribution: Centrofacial (63%), Malar (21%), Mandibular (16%) Woods lamp examination: Epidermal, Dermal, Mixed and Indeterminate. Natural history: Transient, Permanent
Treatment Sun protection Topicals: Hydroquinone, Retinoids, Steroids, Glycolic acid, Kojic acid, Arbutin etc Systemic agents: Glutathione, Tranexemic acid, Vitamin A, C, E Chemical peels Lasers
CONGENITAL MELANOCYTIC NEVUS
NEVUS OF OTA
MONGOLIAN SPOTS