Septic Shock Current Management and New Therapeutic Frontiers




 guidelines for management of severe sepsis and septic shock Dellinger")



 • • • American Association of")

")
 •")




























")




 • Suggest use in patients with clinical")









 in Porcine Peritonitis Septic Shock")













- Slides: 77
Septic Shock: Current Management and New Therapeutic Frontiers R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director Critical Care Medicine Cooper University Hospital Camden, New Jersey
Personal Financial Disclosures • None relevant to presentation today
Background - Basic Definitions • Sepsis = known or suspected infection plus systemic manifestations of infection (SIRS and others) • Severe Sepsis = Sepsis + either – Acute organ dysfunction thought to be due to sepsis – Acute tissue hypoperfusion thought to be due to sepsis • • Hypotension Elevated lactate Oliguria (Altered mental status)
Background - Basic Definitions • Severe Sepsis Organ Dysfunctions – Acute lung injury – Acute kidney injury – Coagulopathy • Thrombocytopenia • Increased INR – Liver Dysfunction – (Cardiovascular) • Septic Shock – Vasopressors +/- organ dysfunction
Surviving Sepsis Campaign (SSC) guidelines for management of severe sepsis and septic shock Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM and the SSC Management Guidelines Committee Crit Care Med 2004; 32: 858 -873 Intensive Care Med 2004; 30: 536 -555
Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008 Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. Crit Care Med 2008; 36: 296 -327 Intensive Care Med 2008; 30: 536 -555
Sponsoring Organizations 2008 Guidelines • American Association of Critical Care Nurses • American College of Chest Physicians • American College of Emergency Physicians • Canadian Critical Care Society • European Respiratory Society • European Society of Clinical Microbiology and Infectious Diseases • European Society of Intensive Care Medicine • Indian Society of Critical Care Medicine • International Sepsis Forum • Japanese Society of Intensive Care Medicine • Japanese Association of Acute Medicine • Society of Hospital Medicine • Society of Critical Care Medicine • Surgical Infection Society • World Federation of Critical Care Nurses • World Federation of Societies of Intensive and Critical Care Medicine
SSC Update 2010/2011
Current Surviving Sepsis Campaign Guideline Sponsors (2010/11 Update) • • • American Association of Critical-Care Nurses American College of Chest Physicians American College of Emergency Physicians Australian and New Zealand Intensive Care Society Asia Pacific Association of Critical Care Medicine American Thoracic Society Brazilian Society of Critical Care(AIMB) Canadian Critical Care Society European Respiratory Society European Society of Clinical Microbiology and Infectious Diseases European Society of Intensive Care Medicine European Society of Pediatric and Neonatal Intensive Care • • • • German Sepsis Society Infectious Diseases Society of America Indian Society of Critical Care Medicine Japanese Association for Acute Medicine Japanese Society of Intensive Care Medicine Latin American Sepsis Institute Pan Arab Critical Care Medicine Society Pediatric Acute Lung Injury and Sepsis Investigators Society Academic Emergency Medicine Society of Critical Care Medicine Society of Hospital Medicine Surgical Infection Society World Federation of Critical Care Nurses World Federation of Societies of Intensive and Critical Care Medicine
Evidence Based Medicine Grading System
Grades of Recommendation, Assessment, Development and Evaluation (GRADE)
Grading Quality of Evidence • A- high quality – Randomized controlled trial (RCT) • B- intermediate – Downgraded RCT or upgraded observational • C- low – Observational or cohort • D- very low – Case series or expert opinion • Upgrade capability
Grading Strength of Recommendation • 1 - strong recommendation – Do it – We recommend • 2 - weak recommendation – Probably do it – We suggest • Determinants of strength – – Quality of evidence Relative importance of outcomes Risks and costs Absolute magnitude and precision of effect
Kumar A, et al. Crit Care Med 2006; 34: 1589 -1596
Antibiotic Therapy Ø We recommend beginning intravenous antibiotics within first hour of recognition of severe sepsis 1 B
• Broad antibiotic coverage initially • Narrow coverage after return of cultures • Source control as soon as possible and within 6 hours
Initial Resuscitation
Resuscitation of Sepsis Induced Tissue Hypoperfusion • Recommend MAP 65 mm Hg • Recommend urine output. 5 ml/kg/hr Grade 1 C
Fluid Therapy • Recommend fluid resuscitation may consist of natural or artificial colloids or crystalloids. Grade 1 B
Probability of Survival The SAFE Study Investigators, N Engl J Med 2004; 350: 2247
Relative Risk of Death from Any Cause among All the Patients and among the Patients in the Six Predefined Subgroups of Survival The SAFE Study Investigators, N Engl J Med 2004; 350: 2247
Sepsis Induced Hypotension • Fluid challenge – Minimum of 20 ml/kg crystalloid or colloid equivalent
Sepsis Induced Tissue Hypoperfusion Ø Requirement for Vasopressors after initial fluid challenge ØLactate ≥ 4 mg/d. L
Figure B, page 948, reproduced with permission from Dellinger RP. Cardiovascular management of septic shock. Crit Care Med 2003; 31: 946 -955.
Which two adrenergic agents are most appropriate to maintain acceptable blood pressure in a patient with septic shock? A. B. C. D. Dopamine or epinephrine Epinephrine or vasopressin Vasopressin or norepinephrine Norepinephrine or dopamine
Which two adrenergic agents are most appropriate to maintain acceptable blood pressure in a patient with septic shock? A. B. C. D. Dopamine or epinephrine Epinephrine or vasopressin Vasopressin or norepinephrine Norepinephrine or dopamine
During Septic Shock Diastole Systole 10 Days Post Shock Diastole Systole Images used with permission from Joseph E. Parrillo, MD
Effects of Dopamine, Norepinephrine, and Epinephrine on the Splanchnic Circulation in Septic Shock Figure 2, page 1665, reproduced with permission from De Backer D, Creteur J, Silva E, Vincent JL. Effects of dopamine, norepinephrine, and epinephrine on the splanchnic circulation in septic shock: Which is best? Crit Care Med 2003; 31: 1659 -1667
Norepinephrine vs. Dopamine
28 -day Survival De Backer D, et al. N Engl J Med 2010, 362; 9: 779 -789
Predefined subgroup analysis by type of shock De Backer D, et al. N Engl J Med 2010, 362; 9: 779 -789
Phenylephrine • Pure vasoconstrictor in general should be avoided – Decreases cardiac output • Rare exceptions – Cardiac output measured and high and difficulty with maintaining MAP with other vasopressor agents – Profound tachycardia or severe ventricular arrhythmias with norepinephrine
Initial Resuscitation of Persistent Hypotension or Lactate >4 Recommend Insertion central venous catheter Recommended goals : • Central venous pressure: 8– 12 mm Hg • Higher with altered ventricular compliance or increased intrathoracic pressure • Scv. O 2 saturation (SVC) 70% Grade 1 C
The Early Bird Gets the Worm
The Importance of Early Goal-Directed Therapy for Sepsis Induced Hypoperfusion NNT to prevent 1 event (death) = 6 -8 Mortality (%) 60 50 Standard therapy EGDT 40 30 20 10 0 In-hospital mortality (all patients) 28 -day mortality 60 -day mortality Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goaldirected therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345: 1368 -1377
Trials of Late Hemodynamic Optimization with Control Group Mortality > 20% After onset of organ failure Alia et al. 1999 Favors Optimization Favors Control Yu et al. 1998 Gattinoni et al. 1995 Hayes et al. 1994 Yu et al. 1993 OVERALL RESULT -0. 4 Kern and Shoemaker Crit Care Med 2002 0. 0 0. 4
Role of Collaboration ED ICU
Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010; 303(8): 739 -46.
Hospital Mortality and Length of Stay Jones, A. E. et al. JAMA 2010; 303: 739 -746. Copyright restrictions may apply.
Vasopressin • Continue to recommend against using high doses of vasopressin (unless salvage therapy) • Vasopressin. 03 units per min plus NE equivalent to norepinephrine alone – VASST trial
Steroid Therapy Figure 2 A, page 867, reproduced with permission from Annane D, Sébille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002; 288: 862 -871
CORTICUS: Results • No benefit in intent to treat – Mortality – Shock reversal • Earlier reversal of shock with steroids in those that had shock reversal
FRENCH TRIAL CORTICUS ++++ ++ < 8 hrs < 72 hrs Degree of Hypotension ++++ ++ Potential for Selection Bias Unlikely Yes Overall Severity of Illness Duration of Shock
Steroids Suggest intravenous hydrocortisone be given only to adult septic shock patients after blood pressure is identified to be poorly responsive to fluid resuscitation and vasopressor therapy Grade 2 C
Recombinant Human Activated Protein C (rh. APC) • Suggest use in patients with clinical assessment of high risk of death due to sepsis induced organ dysfunction typically with APACHE II 25 or greater or multiple organ failure • No absolute contraindications • Weigh relative contraindications Grade 2 B
PROWESS SHOCK
As to Guidelines Publications • “Knowledge is Good”
“Knowledge is Good”
Guidelines Are Not Enough • Protocols • Performance Improvement Programs
Severe Sepsis Resuscitation Bundle Complete tasks within 6 hours of identifying severe sepsis. 1. Measure serum lactate. 2. Obtain blood cultures prior to antibiotic administration. 3. Administer broad-spectrum antibiotic within 3 hours of ED admission and within 1 hour of non-ED admission. 4. In the event of hypotension and/or serum lactate > 4 mmol/L: a. Deliver an initial minimum of 20 m. L/kg of crystalloid or equivalent. b. Begin vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mm Hg. 5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L: a. Achieve a central venous pressure (CVP) of > 8 mm Hg b. Achieve a central venous oxygen saturation (Scv. O 2) > 70% or mixed venous oxygen saturation (Scv. O 2) > 65% Implement the 6 -hour bundle. Available at: http: //ssc. sccm. org/6 hr_bundles.
SSC Interactive Database
Surviving Sepsis Campaign: Phase III • A global, multi-center, 2 -year trial – Multiple hospital networks – 166 sites – 15, 022 patients • Primary outcome – The impact of a model for changing bedside management of sepsis • Secondary outcome – Mortality
Findings • Primary outcome of SSC: behavior change – 20% increase in bundle compliance over 24 months • Secondary outcome - Mortality -- 7. 0% ARR, 19% RRR -- 5. 4% ARR after severity adjustment
Septic Shock Research at Cooper
Intrathoracic Pressure Regulation (ITPR) in Porcine Peritonitis Septic Shock
p<0. 001 n=28
p<0. 001 n=28
: ITPR application and duration
FE 202158 • Vasopressin A 1 receptor agonist
Septic sheep – Traber et al.
V 1 a Receptor Agonist in a Rat Model of PAFInduced Hypotension & Vascular Leak Syndrome
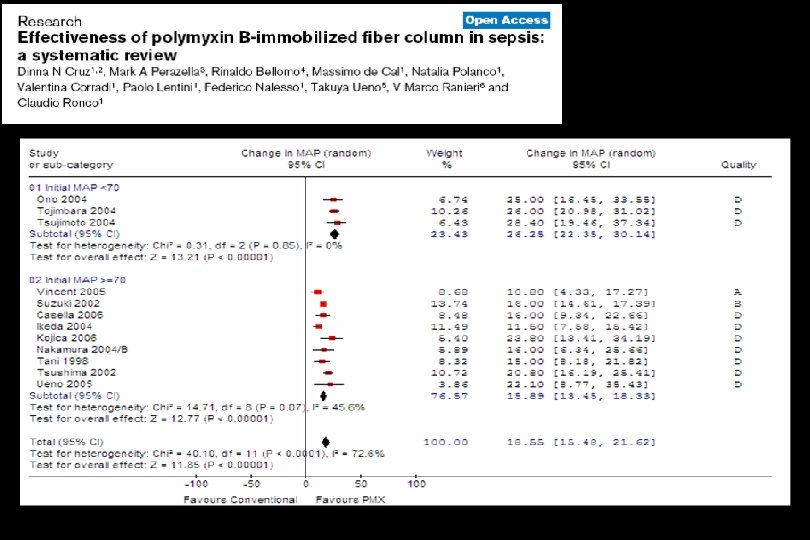
The EUPHRATES Trial Evaluating the Use of Polymyxin B Hemoperfusion in a Randomized controlled trial of Adults Treated for Endotoxemia and Septic shock
Sources of Endotoxin Endotoxemia Endotoxin shed from local bacterial infection Endotoxin translocation from GI Tract n Every human has 25 -30 grams of Endotoxin in their GI tract n Less than 0. 001 grams of Endotoxin is enough to kill a person
Sepsis and Endotoxin Opal SM, et al. Infect Dis, 1999
Intervention DIRECT HEMOPERFUSION WITH ADSORBENT COLUMN USING POLYMYXIN B IMMOBILIZED FIBER BLOOD TUBE Duration: 2 hours FEMORAL or IJ VEIN BLOOD PUMP Perfusion rate 80 -120 ml/min P ANTICOAGULANT 73
EUPHAS: 10 centres, Italy, randomized, unblinded Groups were equal at baseline
Endotoxin Activity Assay EAA™ The only FDA cleared test for detection of Endotoxin Spectral Diagnostics Inc. 76
THANK YOU