Core Concepts in Pharmacology and Medication Administration NRS






 Chemical name • (+/-)-2 -(p-isobutylphenyl) propionic acid Generic name • ibuprofen")

















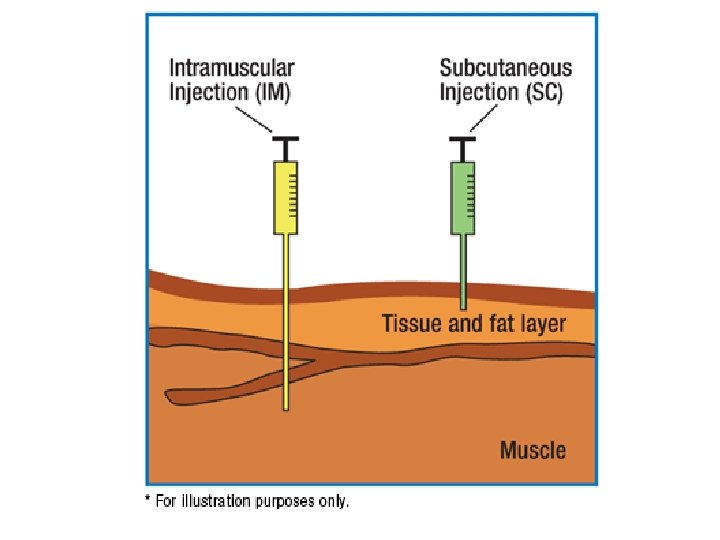
 • Intramuscular • Subcutaneous")
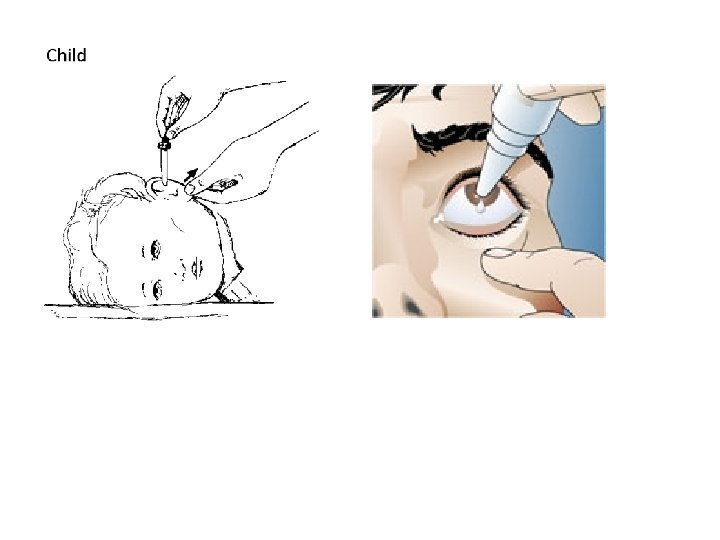
 • Eyes • Ears • Nose •")

 The biologic transformation of a drug into an inactive")
 Delayed drug metabolism results in: • Accumulation of drugs • Prolonged action")
 • Liver")






 • Antagonist-drug")








")







 • Carcinogenic-Causes cancer •")









 • Therapeutic index – The ratio between a drug’s therapeutic benefits and")
 Interactions may occur with other drugs or food • Drug interactions: the")
 • Drug interactions – Additive effect – Synergistic effect – Antagonistic effect")
 • Medication misadventures – Adverse drug events – Adverse drug reactions –")
 Some adverse drug reactions are classified as side effects • Expected, well-known")




 •")
 Assessment • Data collection – Subjective, objective – Data collected")



 • Close consideration of special situations • Prevention and reporting of")









 • Distribution – TBW 70% to 80% in fullterm infants,")
 • Metabolism – Liver immature, does not produce enough microsomal")
 • Excretion – Kidney immaturity affects glomerular filtration rate and")





 • Distribution – TBW percentages lower – Fat content increased")
 • Metabolism – Aging liver produces less microsomal enzymes, affecting")
 • Excretion – Decreased glomerular filtration rate – Decreased number")


 • Adverse drug events (ADEs) • Adverse drug")
 • By definition, all ADRs are also ADEs • But all")




 • Never assume anything about items not specified in a")
 • NEVER use “trailing zeros” with medication orders • Do")
 • ALWAYS use a “leading zero” for decimal dosages •")
 • Check medication order and what is available while using")
 • Always listen to and honor any concerns expressed by")





 • Check expiration dates • Check the patient’s identification")



 • Intramuscular (IM)")

 • Removing medications from ampules • Removing medications from vials •")


 – Subcutaneous (SC or")


 • Intramuscular injections – Ventrogluteal site (preferred) – Vastus lateralis site")





 • Volume-controlled administration set • Using electronic infusion pumps • Patient-controlled")


 • Nasal drugs – Drops – Spray • Inhaled drugs –")

 • Administering medications to the skin – Lotions, creams, ointments, powders")



- Slides: 172
Core Concepts in Pharmacology and Medication Administration NRS 110.
Introduction to Pharmacology : Classification of Therapeutic Agents • Drugs or Medicines • Biologics • Alternative Therapies • Prescription vs Over-the -Counter (OTC) Drugs
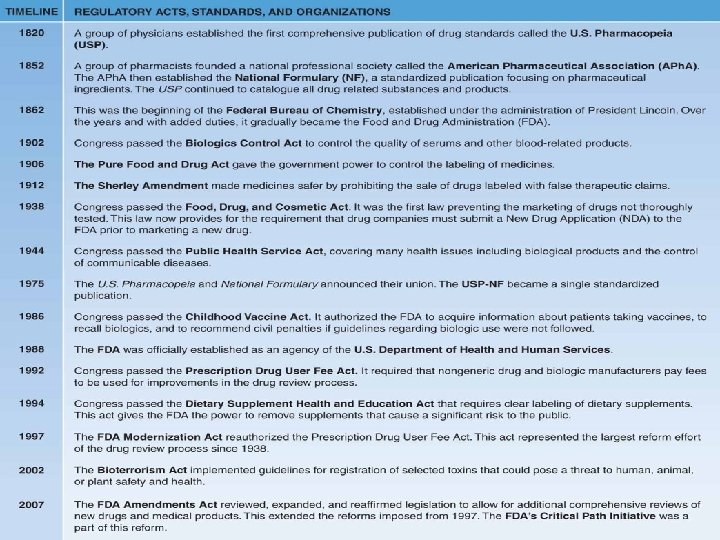
Drug Regulations and Standards • Formulary • Pharmacopoeia • U. S. Pharmacopoeia. National Formulary (USPNF) • Pure Food and Drug Act 1906 • Food, Drug, and Cosmetic Act 1938 • Dietary Supplement Health and education Act (1994) • Food and Drug Administration (1988)
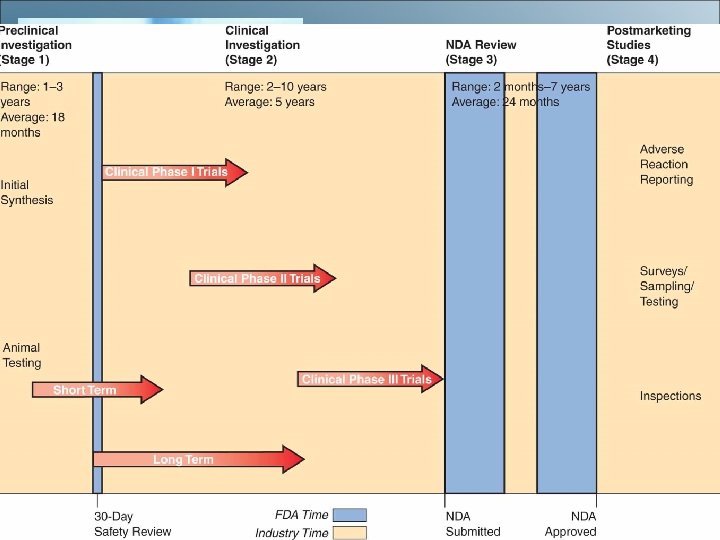
Stages for Drug Approval • • Preclinical Investigation Clinical Investigation NDA Review Postmarketing Surveillance Studies • Canadian Drug Standards
Pharmacologic Concepts
Drug Names Chemical name • Describes the drug’s chemical composition and molecular structure Generic name (nonproprietary name) • Name given by the United States Adopted Name Council Trade name (proprietary name) • The drug has a registered trademark; use of the name restricted by the drug’s patent owner (usually the manufacturer)
Drug Names (cont'd) Chemical name • (+/-)-2 -(p-isobutylphenyl) propionic acid Generic name • ibuprofen Trade name • Motrin®, Advil®
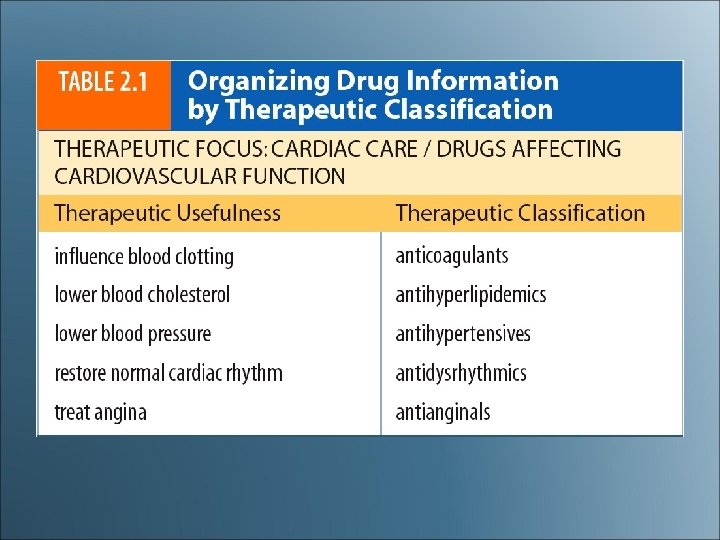
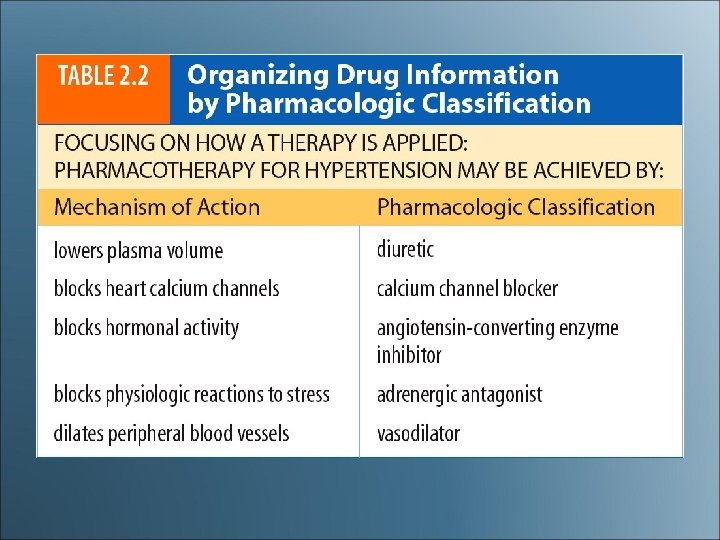
Pharmacological Concepts: Classification • Classification- Functional/Therapeutic Class vs Chemical/Pharmacologic Class • Medication classification indicates the effect of the med on the body system, the symptom the med relieves, or the med’s desired effect (e. g. oral hypoglycemics)
Pharmacological Concepts: Classification • A medication may also be part of more than one class • Aspirin is an analgesic, antipyretic, antiinflammatory, and antiplatelet
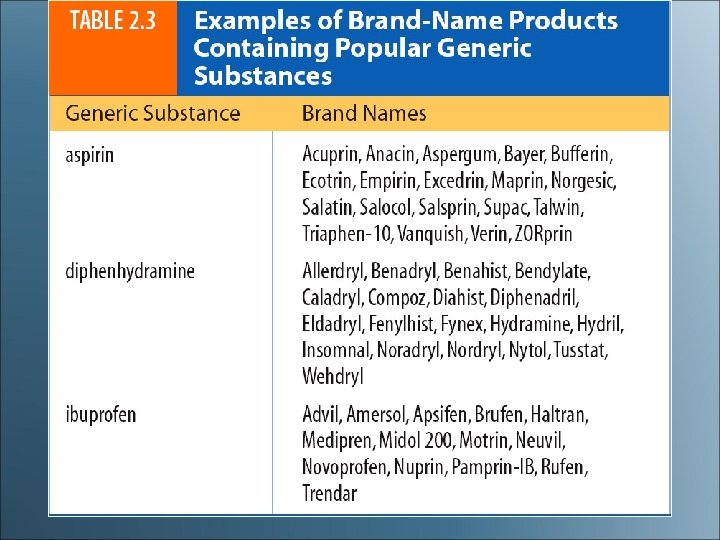
Brand-Name vs Generic Drugs • • • Bioavailability Bioequivalent Negative Formulary List
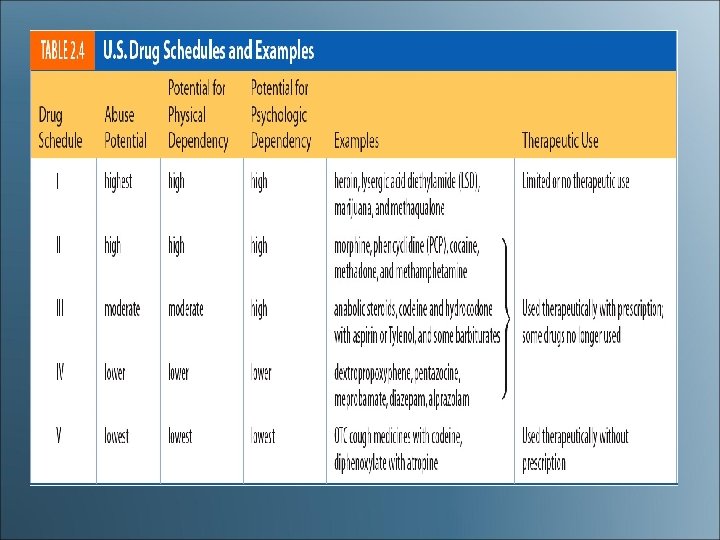
Controlled Substances • High potential for addiction or abuse • Placed into 5 categories or schedules (I-V) • Controlled Substance Act of 1970 • Drug Enforcement Administration (DEA)
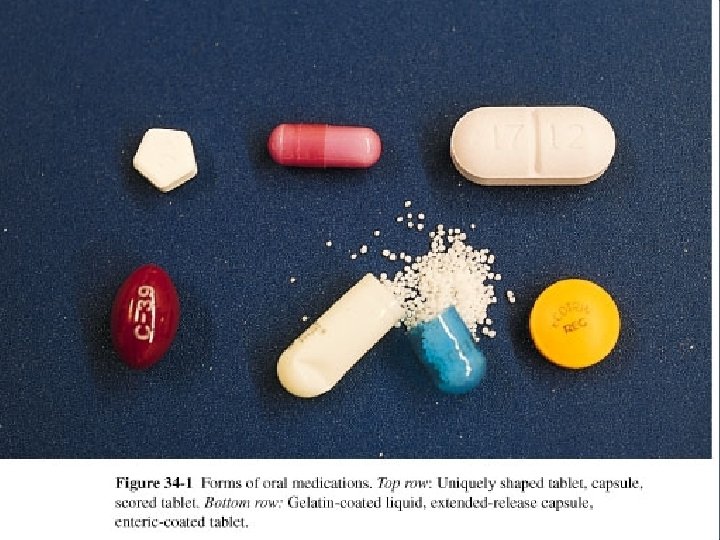
Pharmacological Concepts: Medication Forms • Medications are available in a variety of forms and preparations • The form of the med will determine its route of administration • Composition of med is designed to enhance its absorption & metabolism • Many meds are available in several forms
Medication Forms • • Tablet Capsule Elixir Sustained Release Enteric-coated Suppository Suspension Transdermal patch
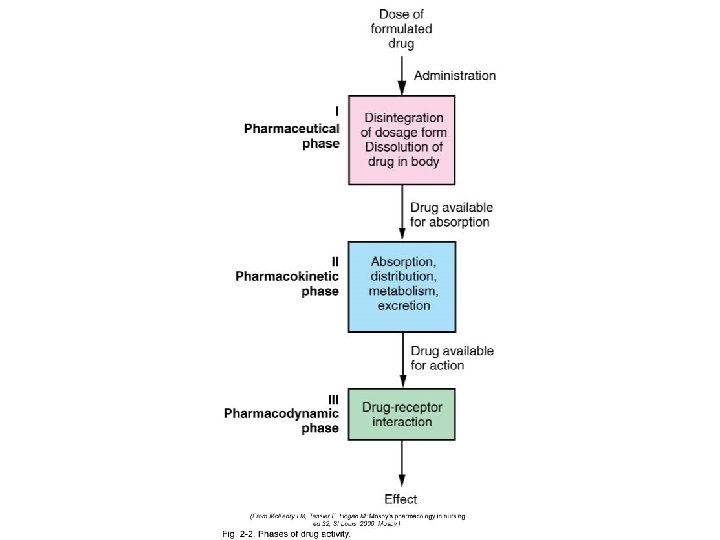
Pharmacokinetics • The study of what the body does to the drug – Absorption – Distribution – Metabolism – Excretion
Pharmacodynamics • The study of what the drug does to the body – The mechanism of drug actions in living tissues
Figure 2 -2 Phases of Drug Activity. (From Mc. Kenry LM, Salerno E: Mosby’s pharmacology in nursing—revised and updated, ed 21, St. Louis, 2003, Mosby. )
Pharmacotherapeutics The use of drugs and the clinical indications for drugs to prevent and treat diseases
Pharmacokinetics: Absorption • The rate at which a drug leaves its site of administration, and the extent to which absorption occurs
Factors That Affect Absorption • Administration route of the drug • Ability of Med to Dissolve • Food or other drugs administered with the drug • Body Surface Area • p. H of the absorptive surface • Rate of blood flow to the small intestine • Lipid Solubility of Med
Routes of Administration • A drug’s route of administration affects the rate and extent of absorption of that drug – Enteral (GI tract) – Parenteral – Topical
Enteral Route • Drug is absorbed into the systemic circulation through the oral or gastric mucosa, the small intestine, or rectum – Oral – Sublingual – Buccal – Rectal
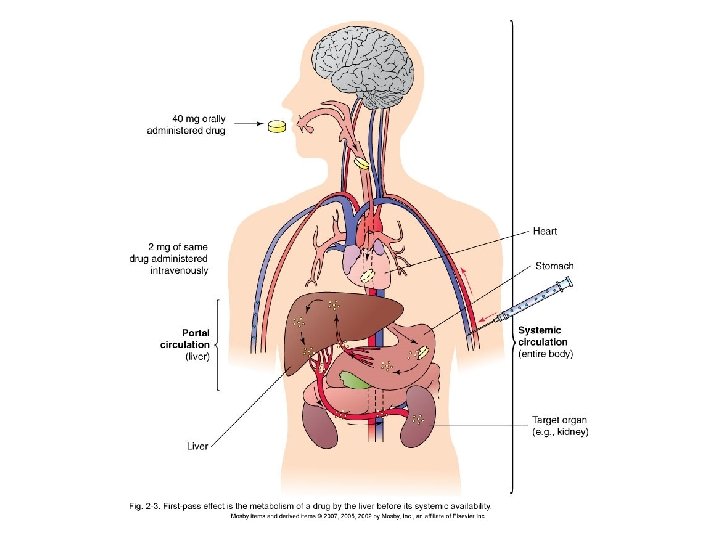
First-Pass Effect • The metabolism of a drug and its passage from the liver into the circulation – A drug given via the oral route may be extensively metabolized by the liver before reaching the systemic circulation (high firstpass effect) – The same drug—given IV— bypasses the liver, preventing the first-pass effect from taking place, and more drug reaches the circulation
Box 2 -1 Drug Routes and First-Pass Effects
Parenteral Route • Intravenous (fastest delivery into the blood circulation) • Intramuscular • Subcutaneous • Intradermal • Intrathecal • Intraarticular
Topical Route • Skin (including transdermal patches) • Eyes • Ears • Nose • Lungs (inhalation) • Vagina
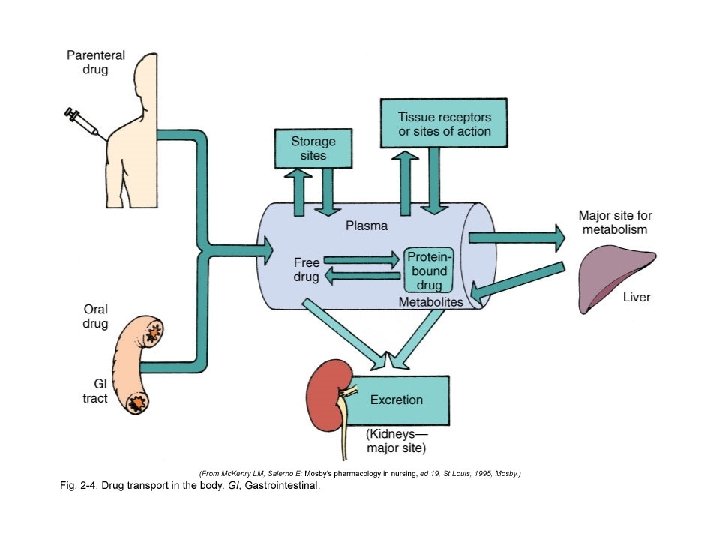
Distribution The transport of a drug in the body by the bloodstream to its site of action • Protein-binding • Water soluble vs. fat soluble • Blood-brain barrier • Areas of rapid distribution: heart, liver, kidney, brain • Areas of slow distribution: muscle, skin, fat
Metabolism (Also Known As Biotransformation) The biologic transformation of a drug into an inactive metabolite, a more soluble compound, or a more potent metabolite • • • Liver (main organ) Kidneys Lungs Plasma Intestinal mucosa
Metabolism/Biotransformation (cont'd) Delayed drug metabolism results in: • Accumulation of drugs • Prolonged action of the drugs Stimulating drug metabolism causes: • Diminished pharmacologic effects
Excretion The elimination of drugs from the body • Kidneys (main organ) • Liver • Bowel – Biliary excretion – Enterohepatic circulation
• 1. You are caring for a patient who has diabetes complicated by kidney disease. You will need to make a detailed assessment when administering medications because this patient may experience problems with: • A. Absorption • B. Biotransformation • C. Distribution • D. Excretion 35 - 41
Pharmacodynamics • Study of the mechanism of drug actions in living tissue • Drug-induced alterations to normal physiologic function • Positive change. Therapeutic effect-Goal of therapy
Mechanism of Action • Ways in which a drug can produce a therapeutic effect • The effects that a particular drug has depends on the cells or organ targeted by the drug • Once the drug hits “site of action” it can modify the rate at which a cell or tissue functions
Mechanism of Action • Receptor Interaction • Enzyme Interaction • Non-Specific Interaction
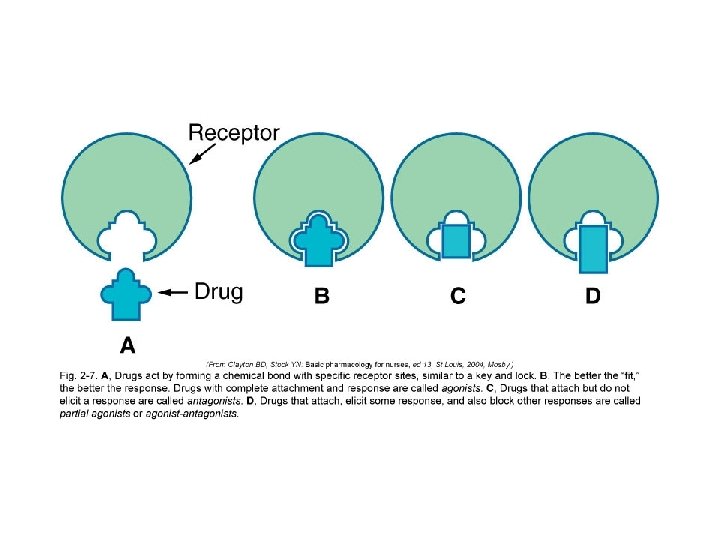
Receptor Interaction • Drug structure is essential • Involves the selective joining of drug molecule with a reactive site on the cell surface that elicits a biological effect • Receptor is the reactive site on a cell or tissue • Once the substance binds to and interacts with the receptor, a pharmacologic response is produced
Receptor Interaction • Affinity- degree to which a drug binds with a receptor • The drug with the best “fit” or affinity will elicit the best response • Drug can mimic body’s endogenous substances that normally bind to receptor site • Drugs that bind to receptors interact with receptors in different ways to either block or elicit a response
Receptor Interaction • Agonist-Drug binds to receptor-there is a response (Adrenergic Agents) • Antagonist-drug binds to receptor-no response -prevents binding of agonists (Alpha & Beta Blockers)
Enzyme Interaction • Enzymes are substances that catalyze nearly every biochemical reaction in a cell • Drugs can interact with enzyme systems to alter a response • Inhibits action of enzymesenzyme is “fooled” into binding to drug instead of target cell • Protects target cell from enzyme’s action (ACE Inhibitors)
Non-Specific Interaction • Not involving a receptor site or alteration in enzyme function • Main site of action is cell membrane or cellular process • Drugs will physically interfere or chemically alter cell process • Final product is altered causing defect or cell death • Cancer drugs, Antibiotics
The nurse is giving a medication that has a high first-pass effect. The physician has changed the route from IV to PO. The nurse expects the oral dose to be: 1. Higher because of the first-pass effect. 2. Lower because of the first-pass effect. 3. The same as the IV dose. 4. Unchanged.
. A patient is complaining of severe pain and has orders for morphine sulfate. The nurse knows that the route that would give the slowest pain relief would be which route? 1. IV 2. IM 3. SC 4. PO
Type of Medication Action • • Therapeutic Effect Side Effects Adverse Effects Toxic Effect Idiosyncratic Reactions Allergic Reaction Medication Interactions Iatrogenic Response
Therapeutic Effect • The expected or predictable physiological response a medication causes • A single med can have several therapeutic effects (Aspirin) • It is important for the nurse to know why med is being prescribed
Side Effects • Unintended secondary effects a medication predictably will cause • May be harmless or serious • If side effects are serious enough to negate the beneficial effect of meds therapeutic action, it may be D/C’d • People may stop taking medications because of the side effects
Adverse Effects • Undesirable response of a medication • Unexpected effects of drug not related to therapeutic effect • Must be reported to FDA • Can be a side effect or a harmful effect • Can be categorized as pharmacologic, idiosyncratic, hypersensitivity, or drug interaction
Adverse Effects • Adverse Drug Events • Adverse Drug Reactions (ADR)
Toxic Effect • May develop after prolonged intake or when a med accumulates in the blood because of impaired metabolism or excretion, or excessive amount taken • Toxic levels of opioids can cause resp. depression • Antidotes available to reverse effects
Idiosyncratic Reactions • Unpredictable effectsoverreacts or under reacts to a medication or has a reaction different from normal • Genetically determined abnormal response • Idiosyncratic drug reactions are usually caused by abnormal levels of drugmetabolizing enzymes (deficiency or overabundance)
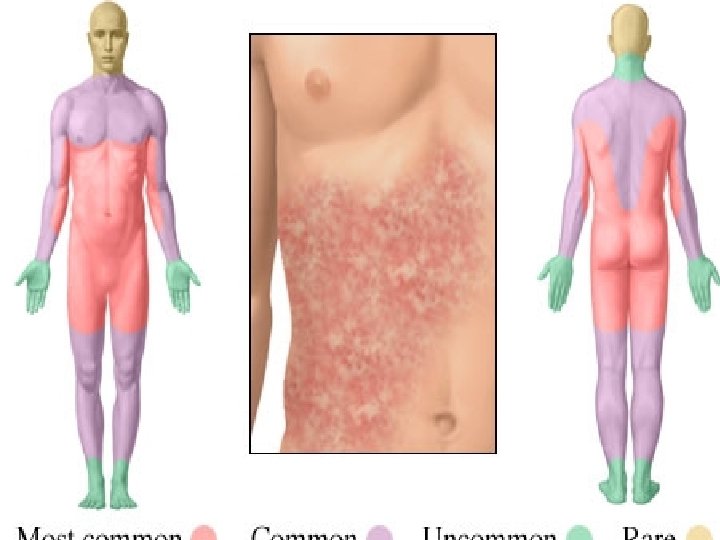
Allergic Reaction • Unpredictable response to a medication • Makes up greater than 10% of all medication reactions • Client may become sensitized immunologically to the initial dose, repeated administration causes an allergic response to the med, chemical preservative or a metabolite
Allergic Reaction • Medication acts as an antigen triggering the release of the body’s antibodies • May be mild or severe • Among the different classes of meds, antibiotics cause the highest incidence of allergic reaction • Severe reaction. Anaphylactic reaction • Mild reaction-hives, rash, pruritis
• 2. A postoperative client is receiving morphine sulfate via a PCA. The nurse assesses that the client’s respirations are depressed. The effects of the morphine sulfate can be classified as: • A. Allergic • B. Idiosyncratic • C. Therapeutic • D. Toxic 35 - 66
Other Drug Reactions • Teratogenic-Structural effect in unborn fetus (thalidomide) • Carcinogenic-Causes cancer • Mutagenic- Changes genetic composition (radiation, chemicals)
Drug Interactions • Occurs when one med modifies the action of another • Common in people taking several medications at once • One med may potentiate or diminish the action of another or alter the way it is absorbed, metabolized or eliminated • Warfarin and Amiodarone
Iatrogenic Responses • Unintentional adverse effects that occur during therapy • Treatment-Induced Dermatologic-rash, hives, acne • Renal Damage. Aminoglycoside antibiotics, NSAIDS, contrast medium • Blood Dyscrasias- Destruction of blood cells (Chemotherapy) • Hepatic Toxicity-Elevated liver enzymes (hepatitis-like symptoms)
Synergistic Effect • Effect of 2 meds combined is greater than the meds given separately • Alcohol & Antihistamines, antidepressants, barbiturates, narcotics • Not always undesirable, physician may combine meds to create an interaction that will have beneficial effects (Vasodilators & diuretics to control high BP)
Medication Dose Responses • Except when administered IV, meds take time to enter bloodstream • The quantity & distribution of med in different body compartments change constantly • Goal is to keep constant blood level within a safe therapeutic range • Repeated doses are required to achieve a constant therapeutic concentration of a med because a portion of med is always being excreted
Medication Dose Responses • Serum Half-Life: Time it takes for excretion processes to lower the serum medication concentration by ½ • Regular fixed doses must be given to maintain therapeutic concentration • Dosage schedules set by institutions (TID, q 8 h, HS, AC, STAT, PRN) • Peak & Trough levels • Therapeutic drug monitoring
Half-life • The time it takes for one half of the original amount of a drug in the body to be removed • A measure of the rate at which drugs are removed from the body
Onset, Peak, and Duration Onset • The time it takes for the drug to elicit a therapeutic response Peak • The time it takes for a drug to reach its maximum therapeutic response Duration • The time a drug concentration is sufficient to elicit a therapeutic response
Pharmacotherapeutics: Types of Therapies • • Acute therapy Maintenance therapy Supplemental therapy Palliative therapy Supportive therapy Prophylactic therapy Empiric
Monitoring • The effectiveness of the drug therapy must be evaluated • One must be familiar with the drug’s: – Intended therapeutic action (beneficial) – Unintended but potential side effects (predictable, adverse reactions)
Monitoring (cont'd) • Therapeutic index – The ratio between a drug’s therapeutic benefits and its toxic effects
Monitoring (cont'd) Interactions may occur with other drugs or food • Drug interactions: the alteration of action of a drug by: – Other prescribed drugs – Over-the-counter medications – Herbal therapies
Monitoring (cont'd) • Drug interactions – Additive effect – Synergistic effect – Antagonistic effect – Incompatibility
Monitoring (cont'd) • Medication misadventures – Adverse drug events – Adverse drug reactions – Medication errors
Monitoring (cont'd) Some adverse drug reactions are classified as side effects • Expected, well-known reactions that result in little or no change in patient management • Predictable frequency • The effect’s intensity and occurrence are related to the size of the dose
Adverse Drug Reaction An adverse outcome of drug therapy in which a patient is harmed in some way • • Pharmacologic reactions Idiosyncratic reactions Hypersensitivity reactions Drug interactions
Other Drug. Related Effects • • • Teratogenic Mutagenic Carcinogenic
Toxicology The study of poisons and unwanted responses to therapeutic agents
Table 2 -9 Common Poisons and Antidotes
The Nursing Process • • • Assessment Nursing diagnosis Planning (with outcome criteria) • Implementation • Evaluation
The Nursing Process (cont'd) Assessment • Data collection – Subjective, objective – Data collected on the patient, drug, environment • • Medication history Nursing assessment Physical assessment Data analysis
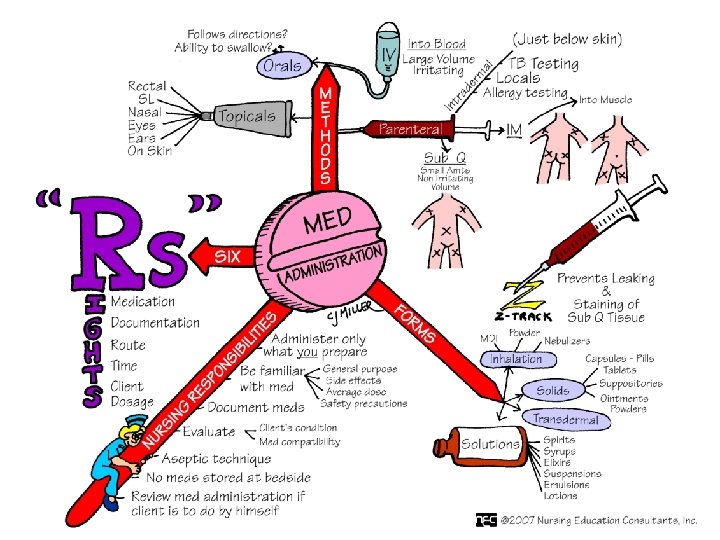
The “Seven Rights” • • Right drug Right dose Right time Right route Right patient Right to refuse Right documentation
Another “Right”—Constant System Analysis • A “double-check” • The entire “system” of medication administration • Ordering, dispensing, preparing, administering, documenting • Involves the physician, nurse, nursing unit, pharmacy department, and patient education
Other “Rights” • • • Proper drug storage Proper documentation Accurate dosage calculation • Accurate dosage preparation • Careful checking of transcription of orders • Patient safety
Other “Rights” (cont'd) • Close consideration of special situations • Prevention and reporting of medication errors • Patient teaching • Monitoring for therapeutic effects, side effects, toxic effects • Refusal of medication
Evaluation • Ongoing part of the nursing process • Determining the status of the goals and outcomes of care • Monitoring the patient’s response to drug therapy – Expected and unexpected responses
The day shift charge nurse is making rounds. A patient tells the nurse that the night shift nurse never gave him his medication, which was due at 11 PM. What should the nurse do first to determine whether the medication was given? 1. Call the night nurse at home. 2. Check the Medication Administration Record. 3. Call the pharmacy. 4. Review the nurse’s notes.
The patient’s Medication Administration Record lists two antiepileptic medications that are due at 0900, but the patient is NPO for a barium study. The nurse’s coworker suggests giving the medications via IV because the patient is NPO. What should the nurse do? 1. Give the medications PO with a small sip of water. 2. Give the medications via the IV route because the patient is NPO. 3. Hold the medications until after the test is completed. 4. Call the physician to clarify the instructions.
Psychosocial, Gender and Cultural Influences on Pharmacotherapy • Psychosocial Influences • Cultural and Ethnic Influences • Gender Influences
Life Span Considerations
Life Span Considerations • • • Pregnancy Breast-feeding Neonatal Pediatric Geriatric
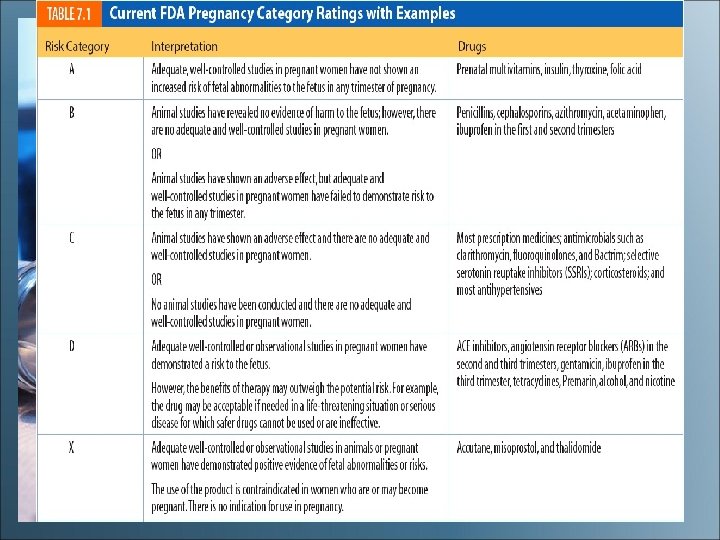
Pregnancy • First trimester is the period of greatest danger for drug-induced developmental defects • Drugs diffuse across the placenta • FDA pregnancy safety categories
Breast-feeding • Breast-fed infants are at risk for exposure to drugs consumed by the mother • Consider risk-to-benefit ratio
Pediatric Considerations: Pharmacokinetics • Absorption – Gastric p. H less acidic – Gastric emptying is slowed – Topical absorption faster through the skin – Intramuscular absorption faster and irregular
Pediatric Considerations: Pharmacokinetics (cont'd) • Distribution – TBW 70% to 80% in fullterm infants, 85% in premature newborns, 64% in children 1 to 12 years of age – Greater TBW means fat content is lower – Decreased level of protein binding – Immature blood-brain barrier
Pediatric Considerations: Pharmacokinetics (cont'd) • Metabolism – Liver immature, does not produce enough microsomal enzymes – Older children may have increased metabolism, requiring higher doses – Other factors
Pediatric Considerations: Pharmacokinetics (cont'd) • Excretion – Kidney immaturity affects glomerular filtration rate and tubular secretion – Decreased perfusion rate of the kidneys
Summary of Pediatric Considerations • Skin is thin and permeable • Stomach lacks acid to kill bacteria • Lungs lack mucus barriers • Body temperatures poorly regulated and dehydration occurs easily • Liver and kidneys are immature, impairing drug metabolism and excretion
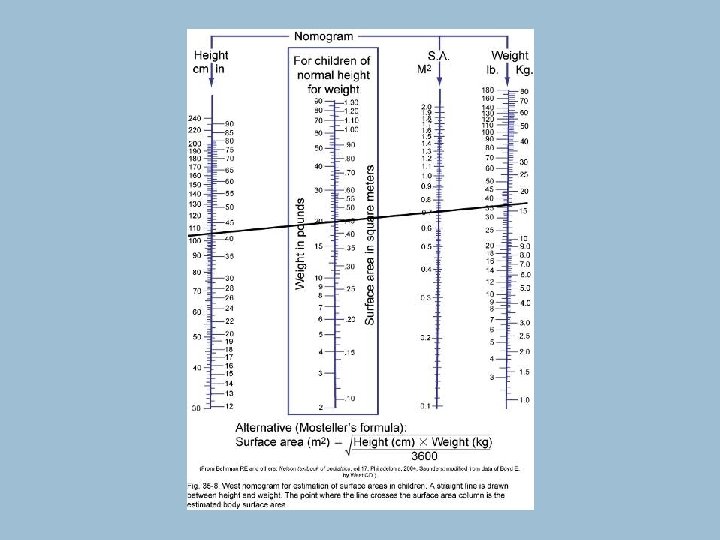
Methods of Dosage Calculation for Pediatric Patients • Body weight dosage calculations • Body surface area method
Geriatric Considerations • Geriatric: older than age 65 – Healthy People 2010: older than age 55 • Use of OTC medications • Polypharmacy
Table 3 -4 Physiologic changes in the geriatric patient
Geriatric Considerations: Pharmacokinetics • Absorption – Gastric p. H less acidic – Slowed gastric emptying – Movement through GI tract slower – Reduced blood flow to the GI tract – Reduced absorptive surface area due to flattened intestinal villi
Geriatric Considerations: Pharmacokinetics (cont'd) • Distribution – TBW percentages lower – Fat content increased – Decreased production of proteins by the liver, resulting in decreased protein binding of drugs
Geriatric Considerations: Pharmacokinetics (cont'd) • Metabolism – Aging liver produces less microsomal enzymes, affecting drug metabolism – Reduced blood flow to the liver
Geriatric Considerations: Pharmacokinetics (cont'd) • Excretion – Decreased glomerular filtration rate – Decreased number of intact nephrons
Geriatric Considerations: Problematic Medications • Analgesics • Anticoagulants • Anticholinergics • Antihypertensives • Digoxin • Sedatives and hypnotics • Thiazide diuretics
Medication Errors: Preventing and Responding
Medication Misadventures • Medication errors (MEs) • Adverse drug events (ADEs) • Adverse drug reactions (ADRs)
Medication Misadventures (cont'd) • By definition, all ADRs are also ADEs • But all ADEs are not ADRs • Two types of ADRs – Allergic reactions – Idiosyncratic reactions
Medication Errors • Preventable • Common cause of adverse health care outcomes • Effects can range from no significant effect to directly causing disability or death
Box 5 -1 Common classes of medications involved in serious errors
• http: //www. usp. org/pdf/ EN/patient. Safety/ismp. A bbreviations. pdf
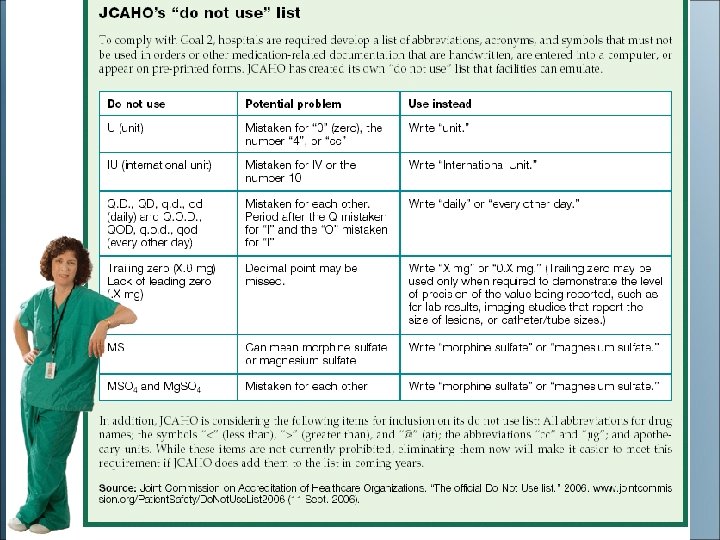
Preventing Medication Errors • Minimize verbal or telephone orders – Repeat order to prescriber – Spell drug name aloud – Speak slowly and clearly • List indication next to each order • Avoid medical shorthand, including abbreviations and acronyms
Preventing Medication Errors (cont'd) • Never assume anything about items not specified in a drug order (i. e. , route) • Do not hesitate to question a medication order for any reason when in doubt • Do not try to decipher illegibly written orders; contact prescriber for clarification
Preventing Medication Errors (cont'd) • NEVER use “trailing zeros” with medication orders • Do not use 1. 0 mg; use 1 mg • 1. 0 mg could be misread as 10 mg, resulting in a tenfold dose increase
Preventing Medication Errors (cont'd) • ALWAYS use a “leading zero” for decimal dosages • Do not use. 25 mg; use 0. 25 mg • . 25 mg may be misread as 25 mg • “. 25” is sometimes called a “naked decimal”
Preventing Medication Errors (cont'd) • Check medication order and what is available while using the “ 7 rights” • Take time to learn special administration techniques of certain dosage forms
Preventing Medication Errors (cont'd) • Always listen to and honor any concerns expressed by patients regarding medications • Check patient allergies and identification • Medication Reconciliation
Medication Errors • Possible consequences to nurses • Reporting and responding to MEs – ADE monitoring programs – USPMERP (United States Pharmacopeia Medication Errors Reporting Program) – Med. Watch, sponsored by the FDA – Institute for Safe Medication Practices (ISMP) • Notification of patient regarding MEs
• 3. Nurses are legally required to document medications that are administered to clients. The nurse is mandated to document: • A. Medication before administering it • B. Medication after administering it • C. Rationale for administering the medication • D. Prescriber’s rationale for prescribing the medication 35 - 129
• 4. If a nurse experiences a problem reading a physician’s medication order, the most appropriate action will be to: • A. Call the physician to verify the order. • B. Call the pharmacist to verify the order. • C. Consult with other nursing staff to verify the order. • D. Withhold the medication until the physician makes rounds. 35 - 130
Medication Administration
Preparing for Drug Administration • Check the “ 7 rights” • Standard Precautions: Wash your hands! • Double-check if unsure about anything • Check for drug allergies • Prepare drugs for one patient at a time • Check three times
Preparing for Drug Administration (cont'd) • Check expiration dates • Check the patient’s identification (2 identifiers) • Give medications on time • Explain medications to the patient • Open the medications at the bedside • Document the medications given before going to the next patient
Drug Routes & First Pass Effects • First Pass Routes- Oral, Rectal • Non-First Pass Routes- Aural, Buccal, Inhaled, Intraarterial, Intramuscular, Intranasal, Intraocular, Vaginal, Intravenous, Subcutaneous, Sublingual, Transdermal
Oral Route • Easiest, most commonly used • Slower onset of action • More prolonged effect • Preferred by clients • Sublingual Administration • Buccal Administration
Enteral Drugs • • • Giving oral medications Giving sublingual or buccal medications Liquid medications Giving oral medications to infants Administering drugs through a nasogastric or gastrostomy tube Rectal administration
Parenteral Route Injecting a medication into body tissues • Subcutaneous (SQ) • Intramuscular (IM) • Intravenous (IV) • Intradermal (ID) • Advanced techniques
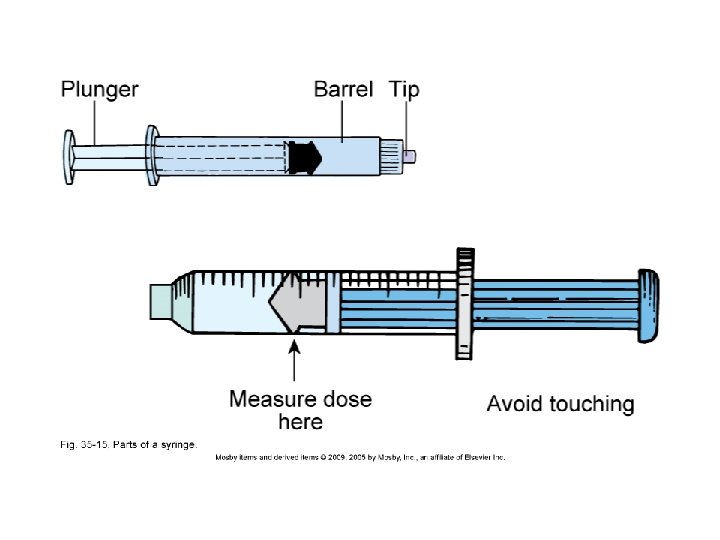
Parenteral Drugs • Never recap a used needle! • May recap an unused needle with the “scoop method” • Prevention of needlesticks • Filter needles
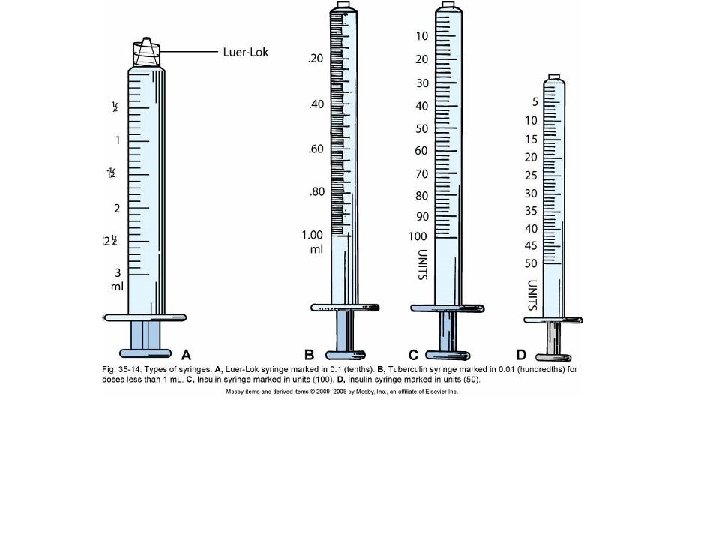
Parenteral Drugs (cont'd) • Removing medications from ampules • Removing medications from vials • Disposal of used needles and syringes • Needle Selection
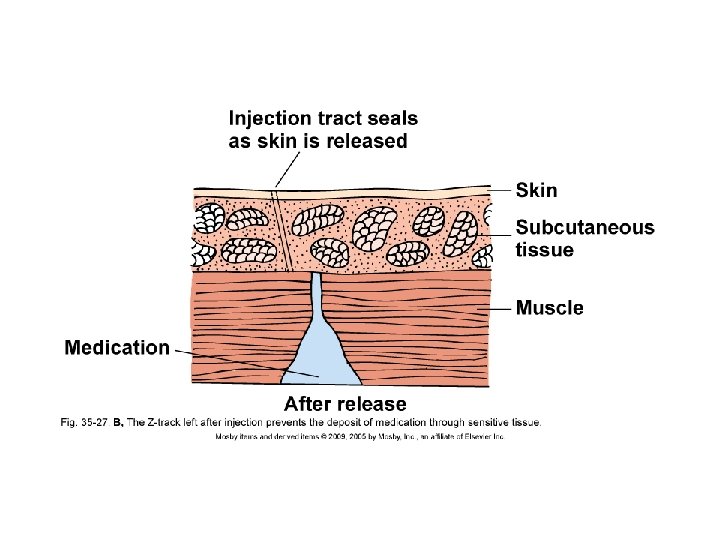
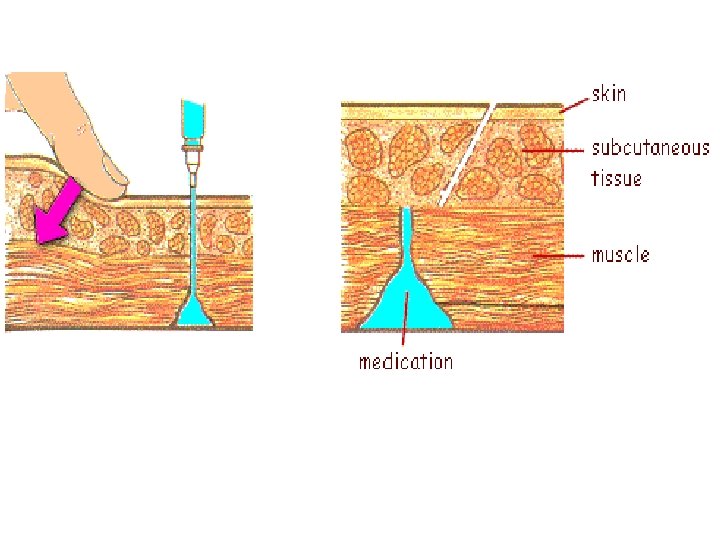
Injections • Needle angles for various injections – Intramuscular (IM) – Subcutaneous (SC or SQ) – Intradermal (ID) • Z-track method for IM injections • Air-lock technique
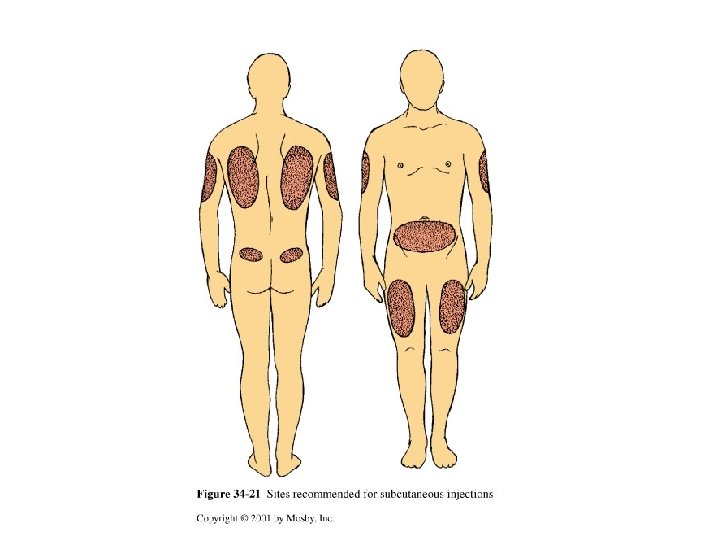
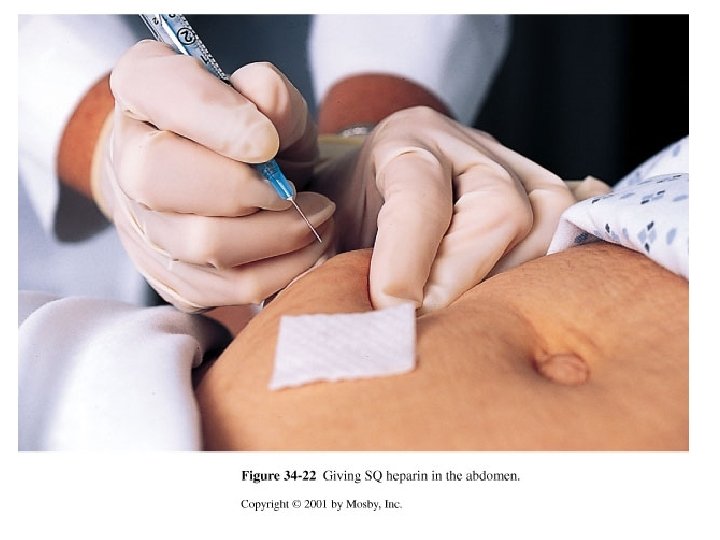
Injection Techniques • Intradermal injections • Subcutaneous injections – Insulin administration – Anticoagulant administration (Heparin/Lovenox)
Injection Techniques (cont'd) • Intramuscular injections – Ventrogluteal site (preferred) – Vastus lateralis site – Dorsogluteal site – Deltoid site
Preparing Intravenous Medications • • Needleless systems Compatibility issues Expiration dates Mixing intravenous piggyback (IVPB) medications • Labeling intravenous (IV) infusion bags when adding medications
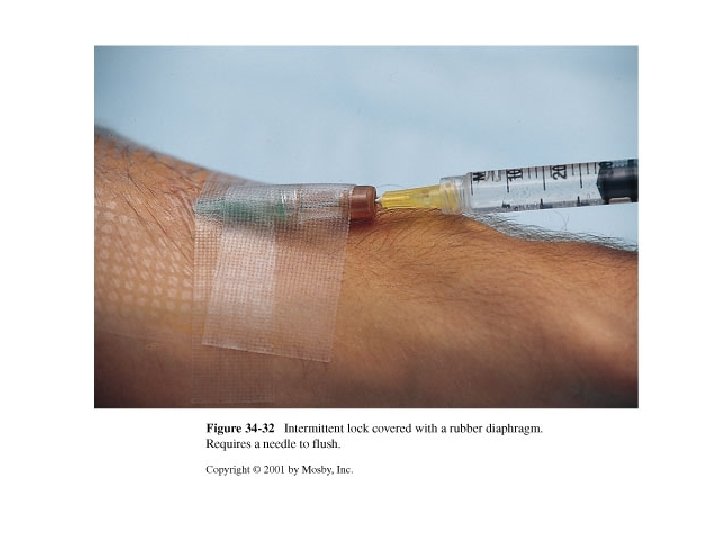
Intravenous Medications • Adding medications to a primary infusion bag • IVPB medications (secondary line) • IV push medications (bolus) – Through an IV lock – Through an existing IV infusion
Intravenous Medications (cont'd) • Volume-controlled administration set • Using electronic infusion pumps • Patient-controlled analgesia (PCA) pumps
Topical Drugs • Eye medications – Drops – Ointments • Ear drops – Adults – Infant or child younger than 3 years of age
Topical Drugs (cont'd) • Nasal drugs – Drops – Spray • Inhaled drugs – Metered-dose inhalers – Small-volume nebulizers
Topical Drugs (cont'd) • Administering medications to the skin – Lotions, creams, ointments, powders – Transdermal patches • Vaginal medications – Creams, foams, gels – Suppositories
Pediatric Drug Administration • • • Infancy Toddlers Preschool and School. Age Children • Adolescents